More about the encephalogram
The essence of the examination is to record the electrical activity of neurons in the structural formations of the brain.
An electroencephalogram is a kind of recording of neural activity on a special tape using electrodes. The latter are attached to areas of the head and record the activity of a certain area of the brain. The activity of the human brain is directly determined by the work of its midline formations - the forebrain and the reticular formation (connecting neural complex), which determine the dynamics, rhythm and construction of the EEG. The connecting function of the formation determines the symmetry and relative identity of signals between all brain structures.
The study is prescribed if there are suspicions of various disorders of the structure and activity of the central nervous system (central nervous system) - neuroinfections such as meningitis, encephalitis, poliomyelitis. With these pathologies, the activity of the brain changes, and this can be immediately diagnosed on the EEG, and in addition, the localization of the affected area can be established. An EEG is carried out on the basis of a standard protocol, which records measurements taken while awake or asleep (in infants), as well as using specialized tests.
The main tests include:
- photostimulation - exposure of closed eyes to bright flashes of light;
- hyperventilation - deep, rare breathing for 3-5 minutes;
- opening and closing eyes.
These tests are considered standard and are used for encephalograms of the brain in adults and children of any age, and for various pathologies. There are several additional tests prescribed in individual cases, such as: clenching your fingers into a so-called fist, staying in the dark for 40 minutes, depriving yourself of sleep for a certain period, monitoring night sleep, and passing psychological tests.
These tests are determined by a neurologist and are added to the main tests performed during the examination when the doctor needs to evaluate specific brain functions.
Preparing for an EEG
- A few days before encephalography, you must stop taking alcoholic beverages and psychotropic drugs. If the patient is constantly taking anticonvulsants or neuroleptics, this must be reported to the doctor performing electroencephalography
- A few hours before the EEG, you can eat, but avoid drinking strong tea, coffee, or Coca-Cola
- Typically, an electroencephalogram is recorded within twenty to thirty minutes. Therefore, you must be prepared to remain motionless for half an hour.
- Before the examination, you must wash your hair and free your hair from clips.
- It is advisable to have a towel (napkins) with you so that after the EEG you can clean the skin of a special gel that is applied to the areas where the electrodes are located.
Taking these simple steps makes it easier to study the bioelectrical activity of brain cells and increases the accuracy of EEG results.
What can be assessed with an EEG?
This type of examination allows you to determine the functioning of parts of the brain in different states of the body - sleep, wakefulness, active physical, mental activity and others. EEG is a simple, absolutely harmless and safe method that does not require disruption of the skin and mucous membrane of the organ.
Currently, it is widely in demand in neurological practice, since it makes it possible to diagnose epilepsy and highly identify inflammatory, degenerative and vascular disorders in the brain. The study also provides identification of the specific location of neoplasms, cystic growths and structural damage as a result of trauma.
EEG using light and sound stimuli makes it possible to distinguish hysterical pathologies from true ones, or to identify simulation of the latter. The study has become almost indispensable for intensive care units, providing dynamic monitoring of comatose patients.
Electroencephalography: indications
- Epilepsy (diagnosis of the disease, assessment of the effectiveness of prescribed drug treatment)
- Convulsive seizures in diseases of the brain (meningitis, encephalitis, tumors, injuries, intoxications, etc.)
- An EEG of the brain is also prescribed for repeated fainting that occurs without any apparent reason
- Sudden pain in the head, dizziness, darkening of the eyes, if such conditions are often repeated, also requires examination of the encephalogram by a neurologist
- Sleep disorders: sleepwalking, sudden attacks of uncontrollable sleepiness (narcolepsy), repeated episodes of sleep apnea, and other symptoms associated with sleep-wake disturbances. To find out the reason for their appearance, along with other research methods, it is recommended to conduct electroencephalography, including EEG monitoring and video monitoring for several hours, during night sleep and even during the day
- Frequent tics (especially common ones), hyperkinesis
- Delayed speech and psychomotor development in children, anxiety disorders and behavioral disorders
- When conducting medical commissions, examinations for permission to work associated with increased danger (pilots, machinists, divers, public transport drivers, special forces employees, etc.)
- Electroencephalography can also be performed for research purposes.
Process of studying the results
The analysis of the results obtained is carried out in parallel during the study, and during the recording of indicators, and continues after its completion. When recording, the presence of artifacts is taken into account - mechanical movement of electrodes, electrocardiograms, electromyograms, and induction of mains current fields. The amplitude and frequency are assessed, the most characteristic graphic elements are identified, and their temporal and spatial distribution is determined.
Upon completion, a patho- and physiological interpretation of the materials is made, and on its basis an EEG conclusion is formulated. Upon completion, the main medical form for this study, called the “clinical electroencephalographic report”, is filled out, compiled by the diagnostician based on the analyzed data from the “raw” recording.
The transcript of the EEG conclusion is formed on the basis of a set of rules and consists of three sections:
- Description of the leading types of activity and graphic elements.
- Conclusion after description with interpreted pathophysiological materials.
- Correlation of indicators of the first two parts with clinical materials.
The main descriptive term in EEG is “activity”, it evaluates any sequence of waves (sharp wave activity, alpha activity, etc.).
The essence of the photostimulation technique
Photostimulation of the eyes is a long-practised, but still relevant, method of treating the organ of vision, which boils down to applying light signals to each eye in turn. In this case, the patient uses special dark glasses. The rhythm of the supplied light signals, their intensity and frequency, are selected in such a way as to have a positive effect on the visual system, through stimulation of the visual analyzer, as well as the brain that processes the information received. This method is aimed at training the internal capabilities of the body, without external interference in its work. This helps to achieve success literally in 7 or 10 sessions, which usually constitute a course of treatment.
Types of human brain activity recorded during EEG recording
The main types of activity that are recorded during the study and subsequently subjected to interpretation and further study are wave frequency, amplitude and phase.
Frequency
The indicator is estimated by the number of wave oscillations per second, recorded in numbers, and expressed in a unit of measurement - hertz (Hz). The description indicates the average frequency of the activity being studied. As a rule, 4-5 recording sections of duration are taken, and the number of waves in each time interval is calculated.
Amplitude
This indicator is the range of wave oscillations of the eclectic potential. It is measured by the distance between the peaks of waves in opposite phases and is expressed in microvolts (µV). A calibration signal is used to measure the amplitude. If, for example, a calibration signal at a voltage of 50 µV is determined on a record with a height of 10 mm, then 1 mm will correspond to 5 µV. In deciphering the results, interpretations are given to the most common meanings, completely excluding rare ones.
Phase
The value of this indicator evaluates the current state of the process and determines its vector changes. On the electroencephalogram, some phenomena are assessed by the number of phases they contain. Oscillations are divided into monophasic, biphasic and polyphasic (containing more than two phases).
Rhythms of brain activity
The concept of “rhythm” in the electroencephalogram is considered to be a type of electrical activity related to a certain state of the brain, coordinated by appropriate mechanisms. When deciphering the EEG rhythm indicators of the brain, its frequency corresponding to the state of the brain region, amplitude, and its characteristic changes during functional changes in activity are entered.
How is electroencephalography performed?
Encephalography should be performed in a specialized medical institution and the recording and subsequent analysis of the EEG should be carried out by an experienced functional diagnostics doctor, or even better, a neurologist (neurophysiologist).
- The patient takes a comfortable position in a lying or sitting position. A set of electrodes, built into a special elastic cap, which is selected according to the size of the patient’s head, is attached to the head of the patient.
- It is important to remain still while recording the electroencephalogram and, if possible, relax the muscles of the body. This will improve the quality of the EEG and facilitate its subsequent interpretation
- Then the electroencephalograph is turned on, the recording of the bioelectrical activity of the brain begins and its transmission from the electrodes to the EEG apparatus, where the received information is amplified, processed and printed in the form of a graphic curve.
In total, the electroencephalogram in standard mode is recorded for twenty to thirty minutes.
Functional tests during EEG
After a standard recording, several functional stress tests are performed to reveal hidden disturbances in the activity of neurons (nerve cells) in the brain on the encephalogram.
- Periodic opening and closing of the eyes during electroencephalogram recording
- Photostimulation, that is, irritation of the visual analyzer with bright flashes of light (the patient’s eyes are closed)
- Taking deep breaths for 1-2 minutes while recording the EEG (hyperventilation)
- At the doctor’s request, the patient performs light gymnastic isometric exercises (clenching fingers into a fist, tensing the abdominal muscles)
- If necessary, certain medications can be used to stimulate the bioelectrical activity of neurons.
Functional tests in some cases make it possible to record paroxysmal activity and other disorders that are not detected by standard EEG recordings.
EEG monitoring and video EEG monitoring
Often, to identify pathological changes (hidden convulsive activity of the brain), an electroencephalogram can be performed during sleep or vice versa - after deliberate deprivation of night sleep. In addition, in recent years, EEG monitoring has become increasingly widespread, that is, long-term recording of an electroencephalogram - for an hour or two, and sometimes for 8-12-24 hours. Such a long-term study significantly increases the information content of the EEG and makes it possible to identify hidden changes in brain activity or, conversely, to exclude their presence.
The information value of electroencephalography for the attending physician increases significantly when using video EEG monitoring, that is, simultaneous recording of the encephalogram and video recording of the patient during the study. Often, this technique makes it possible to record major and minor epileptic seizures, as well as to associate existing changes in the EEG with the patient’s motor activity and other phenomena (falling asleep, waking up, snoring and periods of sleep apnea).
Video-EEG monitoring is also prescribed for distinguishing between epileptic seizures and syncope of somatic origin (with arrhythmia, vegetative-vascular dystonia, endocrine disorders, panic attacks), diagnosing sleepwalking and sleep talking, nightmares, tics and hyperkinesis. Video EEG monitoring is also used to resolve various issues related to admission to certain types of work, when assessing work capacity, and deciding on the abolition of anticonvulsants during long-term remission of epilepsy.
How is an EEG performed on a child’s brain?
An electroencephalogram can be recorded at any age - adults, teenagers, preschool children and even newborns.
- If an EEG is done in the first months of a child’s life, then it is necessary to feed the baby before the study
- During the procedure itself, a child up to one year old is held in the mother's arms
- At the age of three years, electroencephalography is performed in a state of sleep.
- An older child is alone in the EEG room, and the study is performed while awake. In this regard, it is important to calm the baby down and give him the opportunity to get used to an unfamiliar environment.
Rhythms of a waking person
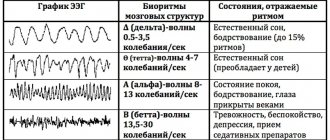
Brain activity recorded on the EEG in an adult has several types of rhythms, characterized by certain indicators and states of the body.
- Alpha rhythm. Its frequency remains in the range of 8–14 Hz and is present in most healthy individuals – more than 90%. The highest amplitude values are observed when the subject is at rest, in a dark room with his eyes closed. It is best identified in the occipital region. It is fragmentarily blocked or completely subsides during mental activity or visual attention.
- Beta rhythm. Its wave frequency fluctuates in the range of 13–30 Hz, and the main changes are observed when the subject is active. Pronounced fluctuations can be diagnosed in the frontal lobes under the obligatory condition of active activity, for example, mental or emotional arousal and others. The amplitude of beta oscillations is much less than alpha.
- Lambda rhythm. It has a small range - 4–5 Hz, and is triggered in the occipital region when it is necessary to make visual decisions, for example, when searching for something with open eyes. The vibrations disappear completely after concentrating your gaze on one point.
- Mu rhythm. Defined by the interval 8–13 Hz. It starts in the back of the head, and is best observed in a calm state. Suppressed when starting any activity, not excluding mental activity.
EEG classification according to Luders
The EEG classification according to Lüders1 is very detailed, it includes both artifacts and rare types of EEG.
- Slow activity Slow down background activity
- Transient slowdown
- Continued deceleration
- Spikes
- Excessive fast activity
- Alpha Coma
- Temporal deceleration in the elderly
Rhythms in sleep
A separate category of types of rhythms that manifest themselves either in sleep conditions or in pathological conditions includes three varieties of this indicator.
- Delta rhythm. Characteristic of the deep sleep phase and for comatose patients. It is also recorded when recording signals from areas of the cerebral cortex located on the border with areas affected by oncological processes. Sometimes it can be recorded in children 4–6 years old.
- Theta rhythm. The frequency interval is within 4–8 Hz. These waves are triggered by the hippocampus (information filter) and appear during sleep. Responsible for high-quality assimilation of information and forms the basis of self-learning.
Based on the results obtained during EEG recording, an indicator is determined that characterizes a complete all-encompassing assessment of the waves - bioelectrical activity of the brain (BEA). The diagnostician checks the EEG parameters - frequency, rhythm and the presence of sharp flashes that provoke characteristic manifestations, and on these grounds makes a final conclusion.
Appartment eye treatment at MGK
MGK specialists have developed and successfully used special programs for hardware eye treatment in children and adults. The procedures are carried out using the most modern equipment (including devices “Spekl M”, “Visotronic M”, “Monobinoscope”) using combinations of medications, and can be prescribed to adults and young patients. After carrying out the necessary diagnostic studies, an individual hardware treatment regimen is selected for each patient, which is then adjusted in accordance with the current results. The procedures are carried out under the supervision of highly qualified specialists, do not cause discomfort and do not require any restrictions in the usual way of life.
The cost of hardware eye treatment for adults and children is determined by the method used in therapy, the number of procedures, etc. and, as a rule, is determined by the attending ophthalmologist, based on the patient’s age, characteristics of the disease, etc. You can see the prices for hardware retinal stimulation in MGC on various devices by following the link.
In the medical department, everyone can undergo examination using the most modern diagnostic equipment, and based on the results, receive advice from a highly qualified specialist. We are open seven days a week and work daily from 9 a.m. to 9 p.m. Our specialists will help identify the cause of vision loss and provide competent treatment for identified pathologies. Experienced doctors, detailed diagnostics and examination, as well as the extensive professional experience of our specialists allow us to ensure the most favorable result for the patient.
You can find out the cost of a particular procedure or make an appointment at the Moscow Eye Clinic by calling multi-line phone 8 (daily from 9:00 to 21:00, free for mobile phones and regions of the Russian Federation) or using the online registration form.
Decoding of electroencephalogram indicators
In order to decipher the EEG and not miss any of the smallest manifestations in the recording, the specialist needs to take into account all the important points that may affect the indicators being studied. These include age, the presence of certain diseases, possible contraindications and other factors.
Upon completion of the collection of all research data and their processing, the analysis is completed and then a final conclusion is formed, which will be provided for making a further decision on the choice of therapy method. Any disturbance in activity may be a symptom of diseases caused by certain factors.
Alpha rhythm
The normal frequency is determined in the range of 8–13 Hz, and its amplitude does not go beyond 100 μV. Such characteristics indicate a healthy state of a person and the absence of any pathologies. The following are considered violations:
- constant fixation of the alpha rhythm in the frontal lobe;
- exceeding the difference between the hemispheres by up to 35%;
- constant violation of wave sinusoidality;
- presence of frequency dispersion;
- amplitude below 25 μV and above 95 μV.
The presence of disturbances in this indicator indicates a possible asymmetry of the hemispheres, which may be the result of oncological tumors or pathologies of cerebral circulation, for example, stroke or hemorrhage. A high frequency indicates brain damage or TBI (traumatic brain injury).
A complete absence of the alpha rhythm is often observed in dementia, and in children, deviations from the norm are directly related to mental retardation (MDD). Such a delay in children is evidenced by: disorganization of alpha waves, shift of focus from the occipital region, increased synchrony, short activation reaction, overreaction to intense breathing.
These manifestations can be caused by inhibitory psychopathy, epileptic seizures, and a short reaction is considered one of the primary signs of neurotic disorders.
Beta rhythm
In the accepted norm, these waves are clearly detected in the frontal lobes of the brain with a symmetrical amplitude in the range of 3–5 μV, recorded in both hemispheres. A high amplitude leads doctors to think about the presence of a concussion, and when short spindles appear, to the occurrence of encephalitis. An increase in the frequency and duration of spindles indicates the development of inflammation.
In children, the pathological manifestations of beta oscillations are considered to be a frequency of 15-16 Hz and a high amplitude present - 40-50 µV, and if its localization is the central or anterior part of the brain, then this should alert the doctor. Such characteristics indicate a high probability of delayed development of the baby.
Delta and theta rhythms
An increase in the amplitude of these indicators above 45 μV on a constant basis is characteristic of functional brain disorders. If the indicators are increased in all brain regions, then this may indicate severe dysfunction of the central nervous system.
If a high amplitude of the delta rhythm is detected, a tumor is suspected. Inflated values of the theta and delta rhythm recorded in the occipital region indicate a child’s lethargy and a delay in his development, as well as impaired circulatory function.
Classification by E.A. Zhirmunskaya
A system for describing EEG types (patterns) and groups was proposed by E.A. Zhirmunskaya in 1984 and is still the basis for visual, verbal assessment of EEG. It should be noted that according to the classification of E.A. Zhirmunskaya's (1991) concept of EEG type refers only to resting EEG recorded in subjects in a state of passive wakefulness, with their eyes closed, and does not include changes that occur in response to efferent stimuli.
The advantage of this classification is the ability to give a general description of the EEG. This creates a certain convenience for the subsequent formation of a conclusion by a medical specialist. At the same time, when making a judgment about the type of EEG, the nature of the EEG pattern in various types of epilepsy is not taken into account, and the focus of pathological activity is not highlighted. According to the classification of E.A. Zhirmunskaya distinguishes 5 types of EEG.
Type I – organized (normal EEG)
The main component of the EEG is the α rhythm, regular in frequency, clearly modulated into spindles, with a medium and high index, with well-defined zonal differences. The α rhythm has the highest amplitude (50-70 μV) in the occipital leads. Towards the anterior parts of the cortex, the severity of the α rhythm decreases. The wave shape is usually smooth. In the temporal regions of the cortex, the α rhythm is presented in the form of fragmentary low-amplitude spindles.
Slow waves are almost not pronounced. δ-activity can also be recorded in the form of single diffuse waves of small amplitude (Fig. 1).
It is advisable to classify EEG with a less ordered structural and spatial organization as this type, the main criterion of which is pronounced α-activity (Fig. 2).
EEGs belonging to type I are interpreted as the ideal norm or as slight changes within the acceptable range of the norm.
Rice. 1. Male, 46 years old.
Electroencephalogram within the age norm. The α-rhythm is modulated, zonal differences are clearly expressed, fragmentary θ- and δ-waves are recorded in the anterior sections
Rice. 2. Man, 72 years old.
Electroencephalogram within the age norm. The α-rhythm is weakly modulated, zonal differences are clearly expressed. Diffuse θ- and δ-activity is recorded in the fronto-central regions
Type II – hypersynchronous (monorhythmic)
It may have variants with a predominance in all areas of the brain or only the α-rhythm, low-frequency ß-activity, or rhythmic θ-activity. The main thing in the structure of this type is the high index of regular fluctuations of biopotentials with the loss of their zonal differences.
Various options for such enhancement of activity synchronization are possible: with preservation and even enhancement of α-range oscillations; with the disappearance of α-activity and its replacement by low-frequency ß-activity or θ-activity. The main characteristic of this type of EEG is the increased regularity of oscillations in the α- (less often ß- or θ-) ranges with the absence of zonal differences.
The option when the α-rhythm dominates, unmodulated or weakly modulated with mild or distorted zonal differences and the absence of fast and slow activity, refers to a moderately disturbed EEG (Fig. 3, 4).
When regular ß-activity with a frequency of 14-25 Hz of small amplitude predominates, the EEG is also considered moderately impaired. In the presence of moderately high or high ß-activity, the EEG is characterized as significantly impaired (Fig. 5).
Rice. 3. Woman, 60 years old.
Encephalopathy. The electroencephalogram shows a hypersynchronous weakly modulated α-rhythm, enhanced in all leads, zonal differences are reduced
Rice. 4. Man, 50 years old.
Symptomatic partial epilepsy. The electroencephalogram shows a hypersynchronous weakly modulated α-rhythm, enhanced in the frontal-central-parietal regions of the brain, zonal differences are reduced, synchronous bilateral discharges of α- and δ-wave complexes periodically occur
Rice. 5. Male, 45 years old.
A complex of functional disorders in the intestines, a feeling of discomfort, increased emotionality. The electroencephalogram shows hypersynchronous high-amplitude ß-activity, enhanced in all leads
Type III – desynchronous (normal variant)
EEG is characterized by low-amplitude bioelectrical activity with the absence or sharp decrease in the number of α-waves. ß-Activity is moderate, diffuse θ- and δ-waves of small amplitude are noted (Fig. 6).
EEGs classified as types II and III reflect regulatory changes in brain activity. In type II, there is a weakening of the activating influences on the cortex from the reticular formation of the brain stem and an increase in deactivating influences from other parts of the limbic-reticular complex.
In type III, on the contrary, there is an increase in activating influences from the reticular formation of the brain stem, which is expressed in desynchronization of α-activity on the EEG. EEGs classified as types II and III reflect regulatory changes in brain activity. Types II and III EEG can occur in patients with neuroses, vegetative-vascular dystonia, cervical osteochondrosis and a number of other diseases.
Rice. 6. Male, 19 years old.
There are no neurological complaints. The electroencephalogram shows low-amplitude bioelectrical activity with the presence of irregular diffuse Θ- and δ-waves. α-Activity is fragmentary and low-amplitude. Variant of the norm
Type IV – disorganized (with a predominance of α-activity)
On the EEG, the main activity is α-activity. In this case, there is significant disorganization of the α-rhythm in all parameters: frequency, amplitude, waveform, distortion of zonal differences. This disorganized α rhythm can dominate all areas of the brain. ß-Activity is also often enhanced, often represented by low-frequency oscillations and increased amplitude; there is an increase in the index of θ- and δ-waves with a fairly high amplitude, the appearance of peaks, sharp waves, flashes and complexes in different areas of the brain. This type of EEG reflects changes in biopotentials in many diseases, which can be associated with microstructural lesions in different parts of the brain, including the cerebral cortex. This category includes atherosclerosis, transient ischemic attacks, neuroinfections, and closed craniocerebral injuries (Fig. 7; 8; 9). Disturbances of the walls of brain vessels and microscopic lesions of brain tissue that occur in these diseases are accompanied by changes in metabolism and neurodynamic disorders. This is accompanied by dysfunction in the activity of the regulatory systems of the brain.
Rice. 7. Male, 38 years old.
5 years ago there was a severe traumatic brain injury with loss of consciousness, loss of ability to work: impaired coordination of movement, slowness of speech. The electroencephalogram was recorded against the background of restoration of working capacity, disorganization of the α-rhythm in shape and frequency, the presence of θ-, δ-rhythm and sharp waves were noted
Rice. 8. Male, 31 years old.
Rice. 9. Woman, 22 years old.
Prolactinemia. The electroencephalogram shows disorganization of the α-rhythm, the presence of sharp waves, and groups of θ-activity
Type V – disorganized (with a predominance of θ- and δ-activity)
δ-Activity is poorly expressed. Amplitude level is medium or high. The type is characterized by the weak presence of α-activity. Fluctuations in biopotentials in the α-, ß-, θ- and δ-ranges are recorded without a clear sequence (Fig. 10).
Type V means that in patients it is no longer regulatory, but microstructural lesions in the cerebral cortex that come to the fore. If there is an EEG of this type, there is every reason to talk about organic brain damage. If an EEG of this type shows a clear focus of pathological activity or a distinct interhemispheric asymmetry, we can assume the presence of a gross macrofocal lesion in one of the brain hemispheres (Fig. 11). In the presence of local pathological activity, it is recommended to view the EEG in bipolar montage mode, which will clarify the localization of the lesion (Fig. 12, 13). The appearance of both local and diffuse pathological phenomena and paroxysmal discharges most often accompanies this particular type of EEG, although it can also occur against the background of any other type of EEG.
Rice. 10. Woman, 66 years old. Secondary generalized convulsive attack.
Cyst in the right anterior frontal region. On the electroencephalogram, fluctuations in the biopotentials of the α-, ß-, Θ- and δ-ranges are recorded without any clear sequence. A clear focus of δ activity is detected in the right temporal region
Rice. 11. Male, 24 years old.
At the age of 8 years he was operated on for a tumor in the left frontotemporal region. At the age of 10, a tumor of the optic chiasm was discovered; bone grafting was not performed. Currently there are generalized seizures at night. The electroencephalogram shows disorganized bioelectrical activity and the presence of local δ-activity in the fronto-parietal-temporal region of the left hemisphere
Rice. 12. Woman, 19 years old.
Partial epilepsy. The electroencephalogram shows disorganized bioelectrical activity, the presence of local δ-activity in the central region of the left hemisphere and the temporal region of the right hemisphere, and a focus of ß-activity in the parietal regions of the right hemisphere
Rice. 13. Woman, 19 years old. Partial epilepsy.
With bipolar montage, the same segment of the electroencephalogram is presented as in Fig. 2.43 δ-activity in leads F3-C3, SZ-RZ and in leads F8-T4 is recorded in antiphase, which suggests the presence of lesions in the left central region (C3) and in the right temporal region (T4) respectively.
Decoding values in different age intervals
An EEG recording of a premature baby at 25–28 gestational weeks looks like a curve in the form of slow flashes of delta and theta rhythms, periodically combined with sharp wave peaks 3–15 seconds long with a decrease in amplitude to 25 μV. In full-term infants, these values are clearly divided into three types of indicators. During wakefulness (with a periodic frequency of 5 Hz and an amplitude of 55–60 Hz), the active phase of sleep (with a stable frequency of 5–7 Hz and a fast low amplitude) and quiet sleep with flashes of delta oscillations at a high amplitude.
Over the course of 3-6 months of a child’s life, the number of theta oscillations is constantly growing, while the delta rhythm, on the contrary, is characterized by a decline. Further, from 7 months to a year, the child develops alpha waves, and delta and theta gradually fade away. Over the next 8 years, the EEG shows a gradual replacement of slow waves with fast ones - alpha and beta oscillations.
Until the age of 15, alpha waves predominate, and by the age of 18, the BEA transformation is complete. Over the period from 21 to 50 years, stable indicators remain almost unchanged. And from 50, the next phase of rhythmicity restructuring begins, which is characterized by a decrease in the amplitude of alpha oscillations and an increase in beta and delta.
After 60 years, the frequency also begins to gradually fade, and in a healthy person, manifestations of delta and theta oscillations are noticed on the EEG. According to statistics, age indicators from 1 to 21 years, considered “healthy,” are determined in subjects 1–15 years old, reaching 70%, and in the range of 16–21 – about 80%.
EEG classification according to Jung
Jung (1953) distinguishes four variants of an unchanged EEG:
- The alpha electroencephalogram contains a well-defined alpha rhythm, the frequency of which fluctuates by no more than 1–1.5 waves per second. Low amplitude beta waves occur in short bursts in the precentral region. Theta waves are barely visible.
- The beta electroencephalogram is dominated by waves with a frequency of 16 to 25 per second with an amplitude of 20–30 μV, recorded partly continuously in the recording, partly in the form of separate groups or series.
- A flat EEG contains a very rare low-amplitude alpha rhythm, a beta rhythm that is small and difficult to distinguish, and flat theta waves are also found. Similar EEGs occur in more than 10% of healthy people. Flat EEGs with an accelerated main type of activity can be detected during mental stress. Transient flattening of the EEG is also detected when alpha waves are blocked during the stage of falling asleep (referred to by some authors as stage zero, for example, Roth, 1962).
- An irregular EEG contains an alpha rhythm, the average frequency of which fluctuates ± 1.5 waves per second. The maximum amplitude of the alpha rhythm in the occipital leads is not clearly expressed. Theta waves, superimposed on alpha waves, are more pronounced in the anterior and temporal regions than in the parietal regions, where they are sometimes visible as components of the lower harmonics of the alpha rhythm.
Such irregular EEGs occur in healthy people as often as flat EEGs. They are more common in youth and in older age and present difficulties in distinguishing them from EEGs with pronounced frequency instability, which represent a transition to dysrhythmia. Transient EEG irregularity occurs during hyperventilation and during the stage of falling asleep.
The most common diagnosed pathologies
Thanks to the electroencephalogram, diseases such as epilepsy or various types of traumatic brain injury (TBI) are quite easily diagnosed.
Epilepsy
The study allows you to determine the localization of the pathological area, as well as the specific type of epileptic disease. At the time of a convulsive syndrome, the EEG recording has a number of specific manifestations:
- pointed waves (peaks) - suddenly rising and falling can appear in one or several areas;
- the combination of slow pointed waves during an attack becomes even more pronounced;
- sudden increase in amplitude in the form of flashes.
The use of stimulating artificial signals helps in determining the form of epileptic disease, since they provide visibility of hidden activity that is difficult to diagnose with EEG. For example, intense breathing, requiring hyperventilation, leads to a decrease in the lumen of blood vessels.
Photostimulation is also used, carried out using a strobe (a powerful light source), and if there is no reaction to the stimulus, then most likely there is a pathology associated with the conduction of visual impulses. The appearance of non-standard vibrations indicates pathological changes in the brain. The doctor should not forget that exposure to powerful light can lead to an epileptic seizure.
3.6. Temporal lobe epilepsy
general characteristics
Temporal lobe epilepsy is a locally caused, often symptomatic, form of epilepsy in which the epileptic focus is localized in the temporal lobe.
Temporal lobe epilepsy manifests itself as simple, complex partial and secondary generalized seizures or a combination thereof.
The most typical signs of temporal lobe epilepsy are: the predominance of psychomotor seizures, a high frequency of isolated auras, oroalimentary and carpal automatisms, frequent secondary generalization of seizures [Troitskaya L.A., 2006].
Complex partial (psychomotor) seizures can begin with or without a preceding aura and are characterized by loss of consciousness with amnesia, lack of response to external stimuli, and the presence of automatisms.
Auras include epigastric (tickling, epigastric discomfort), mental (fear), olfactory, vegetative (pallor, redness of the face), intellectual (feeling of something already seen, already heard, derealization), auditory (auditory illusions and hallucinations (unpleasant sounds, voices, difficult-to-describe auditory sensations)) and visual (illusions and hallucinations in the form of micro- and macropsia, flashes of light, the sensation of an object being removed) aura.
Automatisms are divided into oroalimentary (smacking, chewing, licking lips, swallowing); facial expressions (various grimaces, facial expressions of fear, surprise, smiling, laughter, frowning, forced blinking), gestural (patting one's hands, rubbing one's hand on one's hand, stroking or scratching one's body, sorting through clothes, shaking off, shifting objects, and looking around , marking in place, rotating around its axis, standing up; it was revealed that automatisms in the hand are associated with damage to the ipsilateral temporal lobe, and dystonic positioning of the hand is associated with the contralateral one); outpatient (trying to sit down, stand up, walking, seemingly purposeful actions); verbal (speech disorders: slurred muttering, pronouncing individual words, sounds, sobbing, hissing; it was revealed that seizure speech is associated with damage to the dominant hemisphere, and aphasia and dysarthria - to the subdominant).
It has been noted that in children under 5 years of age, as a rule, there is no clearly identifiable aura, oroalimentary automatisms predominate and motor activity is most pronounced at the time of the attack.
The duration of psychomotor temporal paroxysms varies from 30 s to 2 min. After an attack, confusion, disorientation, and amnesia are usually observed [Atlas..., 2006]. Seizures occur both while awake and during sleep.
More often, in patients with psychomotor temporal paroxysms, clinical symptoms occur in a certain sequence: aura, then interruption of motor activity (maybe with a stoppage of gaze), then oroalimentary automatisms, repeated carpal automatisms (less often other automatisms), the patient looks around, then movements of the whole body .
Simple partial seizures often precede the onset of complex partial and secondary generalized seizures.
Simple partial motor seizures are manifested by local tonic or clonic-tonic convulsions, contralateral to the focus; postural dystonic paroxysms (in the contralateral hand, foot); versive and phonatory (sensory aphasia) seizures.
Simple partial sensory seizures are manifested by olfactory, gustatory, auditory, complex visual hallucinations and stereotypical non-systemic dizziness.
Simple partial vegetative-visceral attacks are manifested by epigastric, cardiac, respiratory, sexual and cephalgic paroxysms.
Simple partial seizures with impaired mental functions are manifested by dreamlike states, phenomena of derealization and depersonalization, affective and ideational (“failure of thoughts,” “whirlwind of ideas”) paroxysms [Temporal…, 1992, 1993; Petrukhin A.S., 2000].
With temporal lobe epilepsy, there are also so-called “temporal syncopes”, starting with an aura (usually dizziness) or without it and characterized by a slow shutdown of consciousness followed by a slow fall. During such attacks, oroalimentary or gestural automatisms may be noted; slight tonic tension of the muscles of the limbs, facial muscles [Late-onset..., 1994].
Epileptic activity from the temporal lobe often spreads to other areas of the brain. Clinical signs indicating the spread of epileptic activity to other parts are versive movements of the head and eyes, clonic twitching of the face and limbs (with the spread of epileptic activity to the anterior parts of the frontal lobe and premotor zone), secondary generalization with the manifestation of generalized tonic-clonic seizures (with involving both hemispheres of the brain in the process).
Neurological status is determined by the etiology of temporal lobe epilepsy.
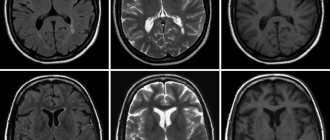
Electroencephalographic patterns
Interictal EEG may not show pathological patterns. Spike, sharp waves, peak-wave, polypeak-wave activity or bursts of theta waves can be recorded in the temporal, frontotemporal, central-parietal-temporal and/or parieto-occipital-temporal leads regionally or bilaterally (bilaterally synchronous with one-sided accent or independently); regional temporal slowing of electrical activity; general slowdown in core activity. Generalized peak-wave activity with a frequency of 2.5–3 Hz may be observed [Kaplov V.A., Ovnatanov B.S., 1987]; generalized epileptiform activity with emphasis and/or spread from the temporal region. An atypical absence pattern is a common finding. Sometimes pathological changes have a frontal focus (
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
).
Seizure EEG is characterized by local low-amplitude beta activity or slowing (first in the theta and then in the delta range) of electrical activity bitemporally or locally in the temporal leads. Then the pathological activity may spread beyond the temporal region [TassiL.et.al., 2001].
Within 10–40 s from the onset of clinical manifestations of an attack, a lateralized appearance of rhythmic theta or alpha activity (with a frequency of 5 counts/s or more) is possible [Ictal..., 1989; Walczak TS et. al., 1992]. Seizure EEG can also be represented by epileptiform activity in the temporal region [Petrukhin A.S., 2000]. In the post-attack period, slow activity on the side of the lesion is often detected.