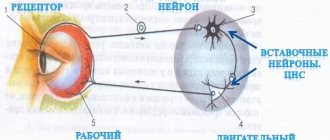
The brain is the control center of our body. All feelings, thoughts or actions are caused by the work of the central nervous system. The brain controls the body by sending electrical signals along nerve fibers, which are first connected to the spinal cord and then dispersed to various organs (the peripheral nervous system). The spinal cord is a “cord” of nerve fibers and is located in the middle of the spinal column. The brain and spinal cord together form the central nervous system ( CNS ).
The brain and spinal cord are bathed in a clear fluid called cerebrospinal fluid, or cerebrospinal fluid for short.
The CNS is made up of billions of nerve cells called neurons. To support neurons, so-called glial cells are also present. Sometimes glial cells can become malignant, causing glial brain tumors. Different areas of the brain control different organs of the body, as well as our thoughts, memories and feelings. There is, for example, a speech center, a vision center, etc.
Central nervous system tumors can develop in any area of the brain, arising from:
- The cells that directly make up the brain;
- Nerve cells entering or exiting;
- Meninges.
The symptoms of tumors are primarily determined by their location, so in order to understand why certain symptoms occur, it is necessary to have an understanding of the anatomy and basic mechanisms of functioning of the central nervous system.
Anatomy
Meninges
The skull protects the brain. Inside the skull there are three thin layers of tissue enclosing the brain. These are the so-called meninges. They also perform a protective function.
Forebrain
The forebrain is divided into two halves - the right and left hemispheres of the brain. The hemispheres control our movements, thinking, memory, emotions, feelings and speech. When nerve endings leave the brain, they cross - they go from one side to the other. This means that the nerves that originate from the right hemisphere control the left side of the body. Therefore, if a brain tumor causes weakness in the left side of the body, it is localized in the right hemisphere. Each hemisphere is divided into 4 regions called:
- Frontal lobe;
- Temporal lobe;
- Parietal lobe;
- Occipital lobe.
The frontal lobe contains areas that control personality, thinking, memory and behavior. The back of the frontal lobe contains areas that control movement and feeling. A tumor in this part of the brain can also affect a patient's vision or sense of smell.
The temporal lobe controls behavior, memory, hearing, vision and emotions. Also located here is the area of emotional memory, and therefore swelling of this area can cause strange feelings that the patient has already been somewhere or done something before (the so-called déjà vu).
The parietal lobe is responsible mainly for everything related to language. The tumor here can affect speech, reading, writing and understanding words.
The occipital lobe contains the visual center of the brain. Tumors in this area can cause vision problems.
Tentorium
The tentorium is a flap of tissue that is part of the meninges. It separates the hindbrain and brainstem from the rest of the brain. Doctors use the term "supratentorial" to mean tumors located above the tentorium other than the hindbrain (cerebellum) or brain stem; “infratentorial” - located below the tentorium - in the hindbrain (cerebellum) or in the brain stem.
Hindbrain (cerebellum)
The hindbrain is also called the cerebellum. It controls balance and coordination. For example, cerebellar tumors can lead to loss of balance or difficulty coordinating movements. Even something as simple as walking requires precise coordination—you have to control your arms and legs and make the right moves at the right time. As a rule, we don’t even think about it - the cerebellum does it for us.
Brain stem
The brain stem controls body functions that we don't usually think about. Blood pressure, swallowing, breathing, heartbeat - all of the above are controlled by this area. The 2 main parts of the brain stem are called the pons and medulla oblongata. The brainstem also includes a small area above the pons called the midbrain.
The brain stem, among others, is the part of the brain that connects the forebrain (cerebral hemispheres) and the cerebellum to the spinal cord. All nerve fibers leaving the brain pass through the bridge, further following into the limbs and torso.
Spinal cord
The spinal cord is made up of all the nerve fibers that run down from the brain. In the middle of the spinal cord there is a space filled with cerebrospinal fluid. The likelihood of primary tumor development in the spinal cord exists, but is extremely small. Some types of brain tumors can spread to the spinal cord, and radiation therapy is used to prevent this. Tumors grow into the spinal cord and compress nerves, causing many different symptoms depending on the location.
Pituitary
This small gland is located right in the center of the brain. It produces many hormones, due to which it regulates various functions of the body. Pituitary hormones control:
- Height;
- Speed of most processes (metabolism);
- Production of steroids in the body;
- The production of eggs and their ovulation - in the female body;
- Sperm production – in the male body;
- The mammary glands produce their secretions after the birth of a child.
Ventricles
The ventricles are spaces inside the brain filled with a fluid called cerebrospinal fluid, or cerebrospinal fluid for short. The ventricles connect to the space in the center of the spinal cord and to the membranes covering the brain (meninges). Thus, fluid can circulate around and through the brain, as well as around the spinal cord. The fluid is mostly water with some protein, sugar (glucose), white blood cells, and some hormones. A growing tumor can block fluid circulation. As a result, the pressure inside the skull increases due to the increasing volume of cerebrospinal fluid (hydrocephalus), which causes corresponding symptoms. In some types of brain tumors, cancer cells can spread into the cerebrospinal fluid, causing symptoms similar to meningitis - headaches, weakness, problems with vision and motor function.
Neurological symptoms related to the anatomical structure of the spinal cord and spine
Knowledge of the anatomical structure of the spinal cord (segmental principle) and the spinal nerves extending from it allows neuropathologists and neurosurgeons in practice to accurately determine the symptoms and syndromes of damage. During a neurological examination of the patient, going from top to bottom, the upper limit of the onset of sensitivity and motor activity of the muscles is found. It should be remembered that the vertebral bodies do not correspond to the spinal cord segments located underneath them. The neurological picture of spinal cord damage depends on the damaged segment.
As a person grows, the length of the spinal cord lags behind the length of the surrounding spine.
During its formation and development, the spinal cord grows more slowly than the spine. In adults, the spinal cord ends at the level of the body of the first lumbar L1 vertebra. The nerve roots extending from it will go further down to innervate the limbs or pelvic organs.
The clinical rule used to determine the level of damage to the spinal cord and its nerve roots is:
- cervical roots (except for the C8 ) leave the spinal canal through the foramina above their corresponding vertebral bodies,
- The thoracic and lumbar roots leave the spinal canal under the vertebrae of the same name,
- the upper cervical segments of the spinal cord lie behind the vertebral bodies with the same numbers,
- the lower cervical segments of the spinal cord lie one segment above the corresponding vertebra,
- the upper thoracic segments of the spinal cord lie two segments higher,
- the lower thoracic segments of the spinal cord lie three segments higher,
- The lumbar and sacral segments of the spinal cord (the latter form the conus medullaris) are localized behind the vertebrae Th9 - L1 .
To clarify the distribution of various pathological processes around the spinal cord, especially with spondylosis, it is important to carefully measure the sagittal diameters (lumen) of the spinal canal. The normal diameters (lumen) of the spinal canal in an adult are:
- at the cervical level of the spine - 16-22 mm,
- at the thoracic level of the spine - 16-22 mm,
- at the level of the lumbar vertebrae L1 - L3 - about 15-23 mm,
- at the level of the lumbar vertebrae L3 - L5 and below - 16-27 mm.
Radiosurgery (gamma knife) of tumors and arteriovenous malformations of the brain
“Gamma Knife” is a device for carrying out high-precision simultaneous irradiation of various pathological formations of the brain. It uses gamma ray energy from radioactive cobalt-60. However, unlike other radiation treatment installations that use Co60, the Gamma Knife is based on the method of stereotactic targeting of radiation to the irradiated object. Irradiation is carried out using 201 focused sources. In this case, the radiation from each of them separately does not have a damaging effect on the brain, but converging at one point (isocenter), they give a total radiation sufficient to cause the desired biological effect in the pathological focus (video). This allows, in most cases, to avoid radiation damage to healthy brain tissue beyond the visible boundaries of the tumor or arteriovenous malformation. The radiation dose is large enough to achieve the desired effect after a single procedure (session duration reaches several hours). Therefore, this type of radiation treatment is called radiosurgery, in contrast to radiotherapy - when the patient is given up to 30-40 sessions in small doses. Powerful radiation damages the DNA of pathological cells and cell membranes, as a result of which the uncontrolled growth of the tumor is disrupted. In the walls of blood vessels, proliferation of the endothelium (the inner layer of the vascular wall) occurs, as a result of which their lumen narrows and completely closes. Thus, the blood supply (or blood supply) changes dramatically and, ultimately, the tumor or AVM decreases, and in some cases disappears after some time.
Today, Gamma Knife is the “gold” standard of radiosurgery in neurosurgical practice due to its high accuracy. The irradiation error on the Gamma Knife does not exceed 0.5 mm (as stated by the manufacturer), but in reality it is no more than 0.2 mm. Such radiation accuracy is not currently available to other radiosurgical units created on the basis of linear accelerators (Novalis, CyberKnife). This quality plays a leading role in cases of localization of the pathological focus in functionally important areas or in the vicinity of radiosensitive structures (for example, the optic nerve or brain stem). Precision is ensured, among other things, by rigid fixation of the head in the frame, which is an indispensable attribute of stereotactic neurosurgery in general, and radiosurgery in particular.
The concept of radiosurgery
Radiosurgery is a method of high-precision irradiation of a pathological intracranial lesion, using a large dose of radiation (from 20 to 100 Gy at the isocenter), at a time, using stereotactic technique through the intact skull. The term was proposed by the Swedish neurosurgeon L. Leksell in 1951. The first device for radiosurgery was designed by L. Leksell and biophysicist B. Larsson in the late 50s of the 20th century and was subsequently called the Gamma Knife for its unsurpassed accuracy. The Gamma Knife device occupies a special place in the neurosurgical arsenal, being a highly specialized instrument for the non-invasive treatment of a wide range of intracranial pathologies (oncology, vascular malformations, trigeminal neuralgia). It should be especially emphasized that the Gamma Knife was initially structurally intended for radiosurgery of exclusively intracranial “targets”. An exception is the latest version of the device - Gamma Knife Perfexion (began to work in our Center on June 2, 2011), which implements the possibility of radiosurgical irradiation of pathological objects, including. at the cervical level of the spinal cord and spine.
How does this happen?
The patient comes to the doctor on the appointed day. During the conversation with the neurosurgeon-radiologist, all the features of the upcoming procedure are explained. Then a CT and/or MRI study is performed, on the basis of which the neurosurgeon-radiologist calculates the optimal radiation plan, taking into account all significant signs of a brain tumor. During the entire treatment session, the patient’s head is specially fixed and motionless in the same coordinate system with the Gamma Knife rays. Quiet, pleasant music sounds. Doctors monitor the patient's condition using special video cameras. After the procedure is completed, the patient can return home and even immediately begin their daily activities. Subsequently, it is necessary to undergo periodic examinations with CT or MRI in order to monitor the obtained clinical effect.
Indications for Gamma Knife radiosurgery
- All benign brain tumors
- Neuromas of the acoustic nerve and other cranial nerves
- Meningiomas of any location
- Pineal tumors
- Pituitary tumors
- Cancer metastases to the brain (up to 10) (see brain cancer signs)
- Arteriovenous malformations and cavernous angiomas
- Primary intracerebral tumors (from I to IV degrees of malignancy) - when continued growth occurs after surgical treatment, radiation therapy and chemotherapy (see signs of brain cancer)
- Trigeminal neuralgia
It should be especially emphasized that radiosurgical treatment is indicated for patients at that stage of the disease when the pathological focus is still small in size (up to 3-3.5 cm) and does not cause severe neurological symptoms, with a satisfactory quality of life, i.e. with minimal or moderate symptoms of a benign tumor or brain cancer. This is of particular importance when the lesion is localized in inaccessible or difficult to access and functionally important areas of the brain. Radiosurgery is also indicated in cases where previous surgery did not lead to complete elimination of the disease, or when it recurs. For elderly and weakened patients, if indicated, radiosurgical treatment is also preferable, because It is much easier to tolerate than surgery. In some situations (for example, with metastatic cancer), radiosurgery has advantages over conventional radiation therapy, in particular for tumors that are resistant to conventional radiation. Currently, radiosurgery using the Gamma Knife is most widely used in neuro-oncology. The main goal of treatment is to control the growth of the pathological tumor. This means that the treatment result is more successful the longer after radiosurgery there are no signs of continued tumor growth.
However, not all types of brain pathology are subject to radiosurgery. Of course, there are certain contraindications to its implementation - for example, the large size of the pathological focus (more than 3-3.5 cm). This is due to the fact that when a large target is irradiated, the risk of local post-radiation complications increases.
The use of radiosurgery is also contraindicated in the case of rapidly developing symptoms of brain compression, for example, by a large tumor.
It should be clearly understood that radiosurgery using Gamma Knife is a modern, highly effective and promising method of treatment. This is confirmed by the enormous experience of its use in developed countries for more than 30 years. However, like any other treatment method, it has its advantages and disadvantages.
Remember, indications and contraindications for radiosurgical treatment can only be determined by a qualified neurosurgeon or radiologist with appropriate training.
How does Gamma Knife differ from conventional neurosurgical intervention?
The main advantages of Gamma Knife stem from its non-invasiveness. To carry out treatment, there is no need for lengthy preoperative preparation and, what is much more important, for postoperative treatment and rehabilitation. Particular attention should be paid to the success of this type of treatment in patients for whom conventional surgery is contraindicated due to the presence of severe concomitant diseases, as well as when the pathological process is localized in deep and functionally important areas of the brain. In addition, there is no risk of anesthetic and surgical complications (bleeding, inflammation, liquorrhea, etc.) inherent in conventional neurosurgical operations. The possibility of outpatient treatment of serious brain pathologies (tumors, AVMs) leads to significant savings in material resources. Several years ago, in Germany, researchers calculated that a neurosurgical operation, along with the entire range of treatment and rehabilitation services, for a patient who could potentially undergo Gamma Knife treatment would cost him (or the state, or the insurance company) approximately twice as much. The unique capabilities of stereotactic radiosurgery using the Gamma Knife installation do not yet allow us to answer the most difficult question of our patients, “how long do they live with brain cancer,” but, by providing high local control of tumor growth, they also allow maintaining the quality of life of patients.
Embryonic development of the vertebrate nervous system
The closure of the neural tube begins in the middle of the embryo, then the process spreads to the head and tail ends of the embryo, where the openings - the anterior and posterior neuropores - remain open for some time (Fig. 7).Rice. 7. Early stages of neural tube formation using the example of human brain development (after: Nieuwenhuys R. et al., 1999). A–D – reconstruction of the appearance of the human embryo and the initial stages of the formation of the neural tube, E–H – transverse sections of the embryo at these stages of development; 1 – ectoderm, 2 – neural plate, 3 – amnion foramen, 4 – medullary plate, 5 – neural fold, 6 – neural groove, 7 – neural tube, 8 – brain rudiment, 9 – anterior neuropore, 10 – posterior neuropore, 11 – neural crest, 12 – pterygoid plate, 13 – lateral plate, 14 – basal plate, 15 – cavity of the primary cerebral ventricles, 16 – rudiments of the spinal ganglia
Even at the stage of neuropore closure, rostro-caudal differentiation of the neural tube of the embryo begins. The neural tube (believed to be under the inducing influence of the notochord) gradually sinks into the mesoderm of the embryo and, under the influence of mesodermal somites, is divided into segmental sections - neuromeres or prosomeres. Somites are located on the sides of the neural plate and are pressed into it, determining the configuration of future parts of the brain (Fig. 8).
Subsequently, the head somites fuse and form three main segments: premandibular, mandibular and hyoid. The boundary of the head segments is the region of the ear capsule, behind which from 2–3 to 10–12 trunk segments are formed (depending on the group of vertebrates). At the same time, the system of cranial nerves is formed. Each segment is innervated by certain pairs of nerves: premandibular - terminal and oculomotor nerve (III); mandibular - trigeminal (V) and trochlear (IV) nerves; hyoid – abducens (VI) and facial (VII) nerves. The two segments following the head are innervated by the glossopharyngeal (IX) and vagus (X) nerves, respectively. The rostral trunk somites in higher vertebrates are innervated by the accessory nerve system (XI), which includes a different number of roots depending on the number of trunk somites. The hypoglossal nerve (XII), which innervates the hypobranchial muscles, which develops from the anlage of the trunk segments, is similar in function to the ventral (somatomotor) roots of the spinal nerves that innervate the striated muscles of the trunk and limbs.
The anterior end of the tube at the end of the 3rd week of development, due to active processes of proliferation and migration of neurons in the brain wall, expands and forms 3 primary brain vesicles. The cranial bladder forms the primary forebrain, Prosencephalon , the middle bladder - the primary midbrain Mesencephalon , and from the third bladder the primary hindbrain Rhombencephalon develops . Next are the structures of the developing spinal cord - Medulla spinalis (Fig. 9).
Rice. 9. Development of the human brain (according to: Sade, Ford, 1976). A–B – stages of three (a) and five (b–e) brain vesicles; top view (A) and side view (B); 1–3 – primary: forebrain (1), middle (2), rhomboid (No.) brain; 4 – anlage of the spinal cord, 5 – optic cup, 6–10 – parts of the brain: terminal (6), intermediate (7), middle (8), posterior (9), medulla (10); 11 – hemispheres of the telencephalon, 20 – cerebellum, 22 – spinal cord, V–IX – cranial nerves. Arrows - bends of the neural tube (s.i. - midbrain, sh.i. - cervical, m.i. - pavement)
The spinal cord is formed from the caudal parts of the neural tube. It is a part of the central nervous system, in the structure of which the features of the embryonic stages of vertebrate brain development are most clearly preserved: the tubular nature of the structure and segmentation.
After the formation of the brain vesicles, complex processes of internal differentiation and growth begin in the nervous system. Already at the early stages of development of the embryo, the neural tube is divided over a considerable length by the boundary groove, sulcus limitans, running along the ventricular surface, into two sections: dorsal - pterygoid plate , and ventral - basal plate . The areas of the brain that develop from the pterygoid plate contain sensory nuclei, and those from the basal plate contain motor and autonomic nuclei. The rostral part of the neural tube does not contain a basal plate and is entirely derived from the pterygoid. The parts of the brain containing derivatives of both plates - middle, posterior, medulla - are often combined under the name "brain stem" .
Changes in the development of the neural tube are accompanied by the formation of several bends at the boundaries of the anlage of various parts of the brain. During the first two months of embryonic development, the main (midbrain) bend is formed when the forebrain and diencephalon bend forward and downward. Then two more (cervical and bridge) bends are formed. At the same time, the first and third primary brain vesicles are each divided into two. The stage of five brain bubbles begins. The telencephalon becomes the most rostral, then the intermediate brain (Diencephalon). After the intermediate brain comes the midbrain (Mesencephalon). The primary hindbrain vesicle is divided into the hindbrain (Metencephalon) and the medulla oblongata (Medulla oblongata). The prosencephalon includes derivatives of the first six prosomeres (neuromeres) P1–P6. The midbrain is subsequently formed from P1 structures. Prosomeres P2 and P3 develop into the thalamus and prethalamus, respectively. The telencephalon and hypothalamus develop from prosomeres P4–P6. From the more caudal segments of the neural tube (rhombomeres), the structures of the brainstem and spinal cord develop.
After the formation of the brain vesicles (5–10 weeks of development), complex processes of internal differentiation and growth of various parts of the brain and spinal cord occur in the structures of the developing nervous system.
The formation of parts of the brain is under the control of the so-called. “secondary organizers” - groups of cells that synthesize a number of morphogenetic factors, the concentration gradient of which determines the direction of migration and differentiation of different brain structures (Table 2; Fig. 9,).
Table 2. Genes and their expression products that control various processes of development of brain regions and structures (according to: Obukhov, 2008).
| Function | ||
| Dlx 1, Dlx 2, Dlx 5 | Subpallium (ganglionic eminences), diencephalon | Migration of subpallial neuroblasts, migration of neurons into the cortex from the ganglionic eminences of the anterior medullary vesicle |
| Emx 1, Emx 2 | Finite brain | Cell proliferation in the developing brain, neuroblast migration |
| Lhx 1, Lhx 2, Lhx 5 | Forebrain, cerebral cortex | Formation of subcortical and cortical (archicortex) sections of the hemispheres |
| Nkx 2.1 Nkx 2.2 | Ventral hemispheres | Proliferation and migration of neuroblasts in the striatum |
| Otx 1, Otx 2 | Forebrain, midbrain, anterior brainstem | Formation of the structure of the hemispheres, including the cerebral cortex |
| Pax 3, Pax 6 | Forebrain | Migration of neuroblasts in the dorsal hemispheres |
The development of the forebrain rudiment is controlled by a small group of cells located at the top of the neural tube and called the anterior neural ridge (ANR) and cells at the border of the second brain vesicle - zona limitans interthalamica (ZLI). The structures of the midbrain, hindbrain, medulla oblongata and the upper segments of the spinal cord are controlled by another organizer - the isthmic organizer (ISO).
During the perinatal period, the formation of the internal structure of the brain ends. Active myelination of the brain and spinal cord begins. However, these processes do not end with birth. It has been shown that for quite a long time (months and years) after birth, the maturation and differentiation of nervous structures and conductive tracts occurs. Moreover, it has now become clear that during the adult period, the formation of new populations of neurons and glial cells occurs due to the preservation of NSC populations in the brain structures.