Perinatology is a science leading from obstetrics to pediatrics. Studies the period of intrauterine development of a child from the 22nd week of a woman’s pregnancy.
Perinatal practice often diagnoses a choroid plexus cyst in a newborn. Education does not have a negative impact on a child. The danger lies in diseases that provoke neoplasms. Perinatology scientists argue: some call choroid plexus cysts a marker of chromosomal abnormalities, but without confirming this.
To avoid consequences, expectant mothers undergo timely diagnosis and find out the causes of the pathology. Based on the size and location of the cysts, the doctor prescribes treatment. Therapy helps eliminate cysts completely or slow down their growth.
What is a choroid plexus cyst?
A choroid plexus cyst is a cavity in the brain. Its walls are formed from cells and tissue. They have clear rounded borders. Inside, the cavity is filled with cerebrospinal fluid or cerebrospinal fluid.
The overwhelming majority of pathology cases are benign. Disorders appear due to the rapid growth of the cystic sac. The neoplasm compresses nearby tissues. This disrupts cerebral circulation and negatively affects nerve cells.
To detect a bubble with liquid, screening is performed. It is a complex of studies to identify the risks of developing diseases in the fetus. Diagnosis is carried out after 20 weeks of pregnancy. The discovery of cysts does not cause concern to doctors, because they have almost no effect on intrauterine development.
Causes
During embryogenesis, the formation of blood vessels precedes the formation of brain matter and the formation of neurons. The choroid plexus is located in the ventricles of the brain, its purpose is to produce cerebrospinal fluid or cerebrospinal fluid. It is formed from the tissues of the pia mater and contains blood vessels and nerve endings that transmit information.
The plexus is formed as follows: the wall of the brain bladder at the site of the future ventricle retains a single-layer structure, which does not differentiate into nervous tissue. Outside, it is adjacent to the pia mater, rich in blood vessels. Gradually it bends and penetrates into the lining of the brain bladder. They grow together, forming many new vessels, from which the plexus is formed.
Choroid plexuses in the fetus are formed at 18-19 weeks. It is during this period that an ultrasound scan can reveal the first signs of cysts, which look like echo-negative formations. Most often, between 20 and 24 weeks, when the brain is actively forming, the size of the cyst decreases and it completely disappears.
The development of the fetus is continuous, constant differentiation of organs and tissues occurs. But if something goes “wrong”, the “deficiency of building material” is replaced by a cyst. The replacement is temporary - the child will be born, and during the first year of life he will develop the necessary structural units.
All that is needed from parents and doctors is to control the development process and create optimal growth conditions for the baby. You only need to worry if the cyst increases in size and does not decrease.
What are the causes of cyst formation?
Based on the time of formation, cysts are divided into two types. When detected at 20 weeks, it is the intrauterine type. In other cases, the cystic sac of the brain is fixed after birth.
In the fetus
The choroid plexus is a paired system. It originates in the ventricles. A pair of plexuses indicates the formation of the left and right hemispheres in the fetus. The vascular plexuses do not have nerve endings. Their main function is to produce cerebrospinal fluid to nourish the brain.
The part of the child’s brain is actively developing and accumulating fluid. During the formation of a cystic sac, the cerebrospinal fluid is located between the plexuses. Then it forms into bubbles. Sometimes this indicates mutation ability. Doctors rarely associate neoplasms with mental disorders. Failure of chromosome division leads to the formation of cavities with fluid.
In 90% of cases, by 28 weeks the cysts resolve on their own and do no harm. But in rare pathologies, the cystic sac remains in the head cavity. For a long time there are no symptoms. In adults, it is diagnosed only on MRI or CT scans.
In a newborn
A choroid plexus cyst in an infant develops under the influence of infectious diseases. In the plexuses of blood vessels, cystic sacs form against the background of negative situations. More often this influence on the mother’s body while carrying a child:
- Herpes virus.
- Infectious diseases (ARVI, influenza, measles).
- Oxygen starvation of the fetus.
- Birth injuries.
- Change or disruption of blood flow.
Education will not affect the brain function of a newborn. The doctor will prescribe treatment only in rare cases of complications when the cyst develops rapidly. Then the child needs constant supervision of parents and a specialist. Signs of complications include frequent excessive regurgitation or vomiting, poor coordination of movements and increased or decreased muscle tone in the child.
In rare cases, the baby suffers from strabismus and convulsions. Symptoms worsen the baby’s life and provoke negative physical development.
What to do if a cyst is discovered in infancy?
Basically, to ensure that the pathology does not interfere with the child’s development. A damaged subependymal area indicates that the child suffered several episodes of hypoxia in utero, or was infected.
The cyst can also replace the site of hemorrhage in the wall of the ventricle. A fairly common cause is the herpes virus; it is considered one of the causes of the formation of brain cysts. Brain damage is caused by difficult childbirth. The main thing is that the size of the cyst should not increase in the baby and development should be disrupted.
The size of the cyst is monitored using ultrasound, which is done at 3, 6, 9 and 12 months. Usually by a year, often earlier, the cyst disappears. It is also necessary to monitor the timing of development and the general condition of the child. The slightest delay requires help and correction.
The following complaints indicating increased intracranial pressure should cause alarm, especially if they appear for the first time:
- constant crying and screaming;
- general increased irritability;
- vomit;
- refusal to eat;
- convulsive attacks.
Such conditions are rare, but parental awareness is the key to ensuring that the baby grows up healthy. An enlarged cyst immediately changes the child’s behavior.
Does it matter whether the side is right or left?
Hardly ever. A cyst of the right choroid plexus is as little dangerous as a formation on the left. In half of all cases of diagnosis, the cysts turned out to be bilateral. This is especially true for formations found in the fetus. There are times when cerebrospinal fluid is already being produced, and the growth of the ventricle simply “does not have time.” Then the cerebrospinal fluid becomes blocked in the middle of the vessels, which can represent a cyst. Such cavities sometimes persist until adulthood, without revealing themselves in any way. Liquor, in contact with the villi of the plexus, has the ability to exchange substances.
Asymptomatic cysts, especially those discovered by chance, do not require treatment. They do not have any effect on the functioning of the nervous system, motor or mental function.
Choroidal cyst
This is the only formation of its kind that requires surgical treatment. The choroidal plexus is located under the large fontanel, and its cyst does not allow the fontanel to close in due time. Normally, complete closure of the fontanelle should occur by the end of the first year of life. This is the deadline; for many babies it closes by six months. A child with a delay in closing the fontanel is sent for an ultrasound examination, where everything is discovered.
Choroidal cysts resolve spontaneously in less than half of cases. The size of this cyst is always substantial, and the baby suffers from excess volume inside the skull.
The baby may be concerned about:
- involuntary twitching of arms and legs;
- convulsive reactions to any violation of the regime or a cold;
- constant drowsiness or increased irritability;
- impaired coordination of movements;
- headache;
- visual impairment.
The large fontanel bulges, pressing on it sharply increases the child’s anxiety or can cause a convulsive attack.
Removal is performed after a complete thorough ultrasound diagnosis (neurosonography) and MRI. Pediatric neurosurgeons perform the removal. The diagnosis of a choroidal cyst is not a death sentence . If you seek help in a timely manner, surgical intervention can completely cure your baby.
Types of vascular cysts
Perinatology divides cystic formations into three types. They are divided according to the process of formation and location in the head. There are pseudocysts on the left, right and bilateral. Depending on the type, treatment and further actions are adjusted.
Vascular cyst of an infant
Localization left and right
Pathology is determined before birth. Unilateral formation does not affect the nervous system. In 5% of cases, active accumulation of cerebrospinal fluid is observed. In infants they appear due to trauma and oxygen deprivation.
Bilateral pseudocysts
They have a complex development mechanism. They require careful monitoring by the doctor and parents of the child in the womb and after birth. There are three types of pseudocysts: choroidal, subependymal and arachnoid.
Choroidal cyst
This is a neoplasm of the choroid plexus of the 3-4 ventricles. The reasons for its appearance are ARVI or flu during pregnancy, hypoxia during childbirth. As education increases, the child experiences frequent and severe headaches, and there is a risk of seizures and twitching of the limbs.
Diagnosis is carried out using an ultrasound machine through the large fontanel. Treatment is most often surgical with the use of medications. This view needs to be removed. The probability of spontaneous resorption is only 45%.
Subependymal cyst
Pathology develops under the lining of the brain cavity. A possible cause is damaged walls of small vessels. They are injured when the child passes through the birth canal. 2-3 capillaries are damaged, and blood flows under the membrane.
The blood is replaced by cerebrospinal fluid, as a result of which a cystic sac appears in the vessels. With normal physical development of the child, it subsides and resolves. This takes approximately a year. A subependymal cyst in a child does not require monitoring or treatment. Dynamics of self-healing – 98%. Neurologists do not consider it necessary to re-diagnose.
Arachnoid cyst
Localized between the soft and hard membranes of the brain. The causes may be infectious diseases, complicated pregnancy and childbirth. A cystic sac does not cause any discomfort to the child. When enlarged, it puts pressure on the meninges on both sides and causes discomfort, as it can reach 0.9 mm.
Necessary treatment is carried out only under the supervision of a doctor. In this case, a specialist can make an accurate diagnosis and select the right medications. Treatment is carried out by eliminating symptoms: headache, vomiting, restless sleep and seizures. Swelling of brain tissue is also prevented and the outflow of cerebrospinal fluid is normalized.
Dr. Evgeny Komarovsky reassured parents whose children were diagnosed with cerebral pseudocysts. The doctor explained that ultrasound often diagnoses pseudocysts in infants. But medicine has not yet identified the reason for the appearance of round tumors. What is clear is that by the age of one year, the blisters resolve in the vast majority of babies. The doctor calls such findings a reason for parents to worry and unnecessary intervention.
Regardless of the type of cyst, you should consult your doctor. You need to carefully understand the diagnosis. According to ICD-10, disease code D32.0 should be checked. After this, decide whether the child’s treatment will be justified.
Pediatric neurosurgeon
AnonymousJanuary 6, 2014, 03:30
Hello, Rezeda Maratovna!
My daughter was born premature at 29 weeks (weight - 1190g, height - 39cm, head circumference - 26cm, chest circumference - 23cm, Apgar score - 4/7). The pregnancy proceeded without complications. At week 28, my water started leaking (2 weeks before I had a slight cold). She laid down for storage. The diagnosis was made: high lateral tear of the amniotic sac, colpitis. She completed a course of antibiotics (cefotaxime) and 3 injections to mature the child’s lungs. At 29 weeks - premature natural birth. She started breathing on her own. Diagnosis at birth: RDS type 1, cerebral ischemia grade 1-2, acute period, sm depression. According to NSG + ultrasound: signs of immaturity of the central nervous system, subependymal pseudocyst in the right caudothalamic sulcus 4x6 mm. On the 1st day she was transferred to the intensive care unit of the Ufa Russian Children's Clinical Hospital. She spent 5 days in intensive care (nursing in an incubator, spontaneous breathing with additional oxygenation through nasal cannulas). Then another month in ONiPN. Diagnosis at discharge (1 month 4 days): cerebral ischemia of the 2nd degree, acute period, tone disorders; MARS: patent foramen ovale. According to the NSG: ventricles 1-1-1, in the projection of the caudothalamic notch on the right there is a cyst of a heterogeneous structure 13x5 mm, PPP-4, immaturity of the brain, hyperechoPVO. At 2 months, we went to the Russian Children's Clinical Hospital for a neuropathologist, a follow-up room, and had an NSG done. Diagnosis after examination: PPP of the central nervous system, recovery. period, with tone disturbances. According to NSG: ventricles 2-2-2, in the projection of the caudothalamic notches on BOTH sides, subependymal cysts with septa inside are identified: on the right 10x5mm, on the left 11x7mm; the interhemispheric fissure is slightly expanded to 5 mm, the intrathecal space in the projection of the frontal lobes is 2-3 mm wide. Treatment was prescribed: 1) neurologist - exercise therapy, massage, Elkar 5 drops. 3 times a day.; 2) pediatrician - ferrum lek and vitamin D. Now about our daughter: we are now 3 months old (from birth): we are gaining weight well (currently 3900g), normal appetite, active, she smiles until she coos (groans), she practically holds her head up by herself , lying on her stomach, she tries to raise her head (it doesn’t always work), she began to fix her gaze on people and objects, and studies with her eyes. But often the hands are clenched into fists, sometimes there is a tremor of the chin and waves of the hands, very rarely - he cries in his sleep and suddenly calms down. In general, he sleeps well, except for periods when his tummy bothers him. Need your advice! Is the prescribed treatment enough in this case??? I am very worried about the cysts - as I understand it, at first there was one, but now there are two. But the doctors said nothing about this! (The ultrasound doctor only said that the structure of the cysts had changed and that was good. Also, that they would most likely resolve on their own, it was a matter of time). What to do??? The next control was scheduled at 4 months (i.e. in a month). Wait? ReplyDelete
Diagnostics
During pregnancy, a woman undergoes mandatory tests. The first signs of the disorder are detected in the prenatal period. Early screening allows changes in the choroid plexus to be monitored through repeat diagnostics.
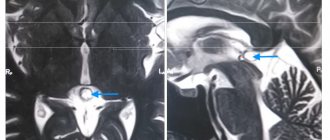
During the first period of a child’s life, the child is monitored through ultrasound. This procedure is mandatory. Allows you to determine whether there is damage to the ventricle. In addition, ultrasound can show a bilateral formation.
If the cyst does not shrink and causes specific symptoms, an MRI or CT scan is used. This diagnosis is carried out one year after birth. Until this point, the cyst can resolve on its own. Once the diagnosis is confirmed, the neurologist registers the child to monitor his condition.
Treatment of pathology
The prognosis for cystic formation of the choroid plexus is positive. No therapy or drug intervention is required. Treatment is prescribed in cases of rapid growth of cysts. This provokes an increase in intracranial pressure, disrupts blood circulation in the brain and the transmission of nerve impulses. The neurologist determines the treatment tactics: therapy or surgery.
Drug therapy
The reason that causes the pathological growth of the cystic sac is an infectious disease. In this case, the doctor prescribes antiviral and antibacterial drugs. They are indicated for a pregnant woman to prevent the growth of tumors in the lateral ventricle of the brain. An analysis is required to confirm the infection.
When prescribing treatment for a baby with an enlarging cystic sac, the neurologist is guided by test results and ultrasound. Treatment is adjusted depending on the symptoms. For headaches, medications are prescribed to normalize blood circulation. Diuretics reduce intracranial pressure. For convulsions and twitching of the limbs, anticonvulsants are prescribed. A mild sedative is prescribed if the child is overexcited and does not sleep well.
Surgical intervention
Prescribed in extreme and rare cases. Surgery prevents the risk of complications of symptoms. In the future he will maintain normal mental and physical development. Surgical intervention in this case can be of two types: bypass surgery and trepanation.
Bypass surgery is a procedure with minimal trauma. Fluid is pumped out of the cystic cavity through special tubes. There is a risk of infection, so antibiotic therapy is carried out. This eliminates the development of inflammation and damage to brain tissue. High probability of relapse.
Trepanation is an extremely dangerous method. Prescribed in case of ineffectiveness of other procedures. At a more mature age, neurological pathologies may appear.
Possible prevention of pathology
In the event of the birth of a child, the prevention of his health depends on the mother. A woman should try to avoid hypothermia and not visit crowded places where she can get an infection. Smoking, drinking alcohol and lack of physical activity pose a great danger. In this case, the fetus does not receive enough oxygen.
From the very beginning of pregnancy, it is necessary to register with a gynecologist. As prescribed by the doctor, go to specialists and take the necessary tests. If an infection occurs, you must carefully follow the instructions and recommendations of a specialist.