3 January 2021
22613
0
3.7 out of 5
Some diseases of the spine, vascular disorders and even endocrine pathologies can provoke the occurrence of such an unpleasant and very detrimental condition as cervical myelopathy. It is accompanied by disturbances in sensitivity and mobility, and can also lead to serious complications. Therefore, it is important to diagnose it in the early stages of development, establish the cause of its occurrence and effectively influence it in order to avoid worsening the condition.
Myelopathy concept
Myelopathy is a comprehensive definition of spinal cord disorders of a dystopic nature and any etiology. It can be a complication against the background of diseases of the spine and joints, vascular degenerative processes, injuries, metabolic or infectious processes, and therefore the final diagnosis should be clarified by explaining the nature of the origin of the disease - ischemic, compression, etc.
The vast majority of myelopathies have an onset outside the spinal substance, as developed against the background of:
- osteochondrosis;
- vertebral fractures;
- spondylosis;
- intoxication (toxins, radiation, etc.);
- atherosclerosis;
- diabetes mellitus and other pathologies of the spine, blood vessels and endocrine system.
The following most common cases of myelopathy are caused by direct damage to the spinal substance:
- injuries;
- infections;
- tumor;
- heredity.
As an exception, the disease may develop after a lumbar puncture. The compression type (with compression of the spinal cord) predominates over all others.
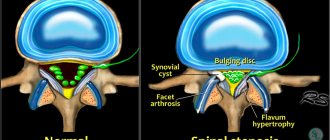
Myeloradiculopathy in spinal stenosis
Myelopathy and myeloradiculopathy are the most serious consequences of various diseases of the spinal column.
Myelopathy is a collective term for any damage or compression of the spinal cord of various origins. For example, brain damage due to infectious diseases, degenerative processes, cancer, radiation or radiation exposure, injuries or hematomas, etc.
Myeloradiculopathy is a complex of reversible and irreversible processes that occur as a result of damage to the spinal cord itself, its membranes, spinal nerve roots and blood vessels, which is accompanied by liquorodynamic and rheological disorders.
The development of myelopathy and myeloradiculopathy is largely facilitated by congenital or acquired narrowing of the spinal canal (stenosis), resulting in a discrepancy between the parameters of the osteoligamentous sheath of the inner walls of the canal and the neurovascular and cerebral structures located in them.
Over time, a pathological situation associated with mechanical compression of soft tissues, circulatory disorders and the movement of cerebrospinal fluid is created and progresses, which already requires appropriate treatment.
Causes and classification of stenosis
Quite common causes of narrowing of the spinal canal are progressive dystrophic processes in the intervertebral discs, joints and ligaments in combination with congenital (genetic, hereditary) or constitutional features of the structure of the spine, the vertebral bodies themselves, processes and/or arches, in which there is a relatively small capacity of the dural sac .
Dystrophic pathologies:
- osteochondrosis;
- herniation or protrusion of intervertebral discs with (or without) calcification of the fibrous ring (dense membrane) of the disc;
- vertebral instability;
- spondylolisthesis;
- proliferation of osteophytes;
- hypertrophy of intervertebral joints and/or ligamentum flavum;
- arthrosis of the joints and other diseases.
For ease of designation, the following classification of stenosis has been introduced into medical terminology:
By distribution (localization) along the spinal column:
- cervical region;
- chest;
- lumbar
By degree of damage:
- monosegmental;
- polysegmental;
- intermittent;
- total.
By stages of development:
- dynamic;
- fixed (for spondylolisthesis, prolapsed (herniated) intervertebral disc).
Hernial protrusions and osteochondrosis, as it progresses, cause fixed segmental stenosis of the spinal and radicular canals.
Spinal instability and spondylolisthesis are dynamic disorders, provided that the initial canal width is anatomically sufficient. In this case, surgery to introduce a stabilization system completely eliminates all disturbing symptoms.
Multiple lesions of intervertebral discs, ligaments and joints, such as in primary osteoarthritis (especially in older people), cause polysegmental narrowing of the spinal canal.
With spondyloarthrosis or the formation of intervertebral hernias in the lateral (side) plane, partial stenosis occurs at several levels, interspersed with healthy areas, which is usually called intermittent.
Symptoms
Lateral stenosis, as a rule, causes compression of one nerve canal and root, which is manifested by signs of monoradiculopathy.
Narrowing of the central canal is usually combined with compression of the nerve structures of the cauda equina and has symptoms of polymyeloradiculopathy with ischemic signs.
Neurological signs of lumbar spinal stenosis in most patients are expressed in the form of pain in the lumbar region, buttocks and lower extremities, lumbar ischialgia, accompanied by a feeling of heat or cold, as well as:
- Paresthesias turning into motor disorders in combination with mild or absent neurological signs of damage to the nerve roots. It is this pathology that in the later stages of the disease develops into compression-ischemic myeloradiculopathy or transverse spinal cord lesion syndrome.
- Neurogenic intermittent claudication syndrome, which is observed in most patients, regardless of the location of the stenosis in the spinal canal.
- Constantly present mechanical pressure, transient ischemia of the spinal cord and nerve roots, causes chronic vasospasm, venous and liquor hypertension, which with prolonged exacerbation turns into myelopathy.
- Compression of the cauda equina manifests itself in motor and reflex disorders, loss of sensitivity (hyposthesia) of the skin of the lower extremities. As it progresses, asymmetric muscle hypertrophy, hyporeflexia, and cramps of individual muscle groups occur. In the later stages of the disease, dysfunction of the pelvic organs (urinary or fecal incontinence) appears, especially during fast walking, prolonged standing or during physical activity.
Impaired muscle activity of the lower extremities in lumbar spinal stenosis
Against the background of spinal canal stenosis at the waist level, the majority of patients (more than 43%) experience persistent muscle wasting of the legs. At the same time, not only the ability of muscle fibers to contract and relax changes, but also qualitative changes progress.
For example, when staying in static poses for a long time, the muscles are forced to remain in a contracted state and undergo spatial deformation. So some fibers are overstretched, while others, on the contrary, go into a state of hypertonicity, which subsequently causes residual changes and a significant increase in pain.
Thus, when diagnosing and prescribing treatment for spinal stenosis, in addition to identifying the location and degree of compression of the spinal cord, destruction of the osseous-ligamentous apparatus and other pathologies, it is necessary to examine the condition of the patient’s muscle tissue.
It is recommended to supplement the usual examinations for this disease (MRI and CT) with electromyography (EMG). It allows you to assess the neuromotor functionality of the spine, both in patients with various pathologies of the musculoskeletal system, and in healthy people. Electromyography can serve as a qualitative indicator of the effectiveness of the treatment and in the early stages diagnose the prerequisites for the development of stenosis.
Clinical studies tested the condition of the muscles (calf and tibia) of the lower extremities at rest and after exercise in patients suffering from lumbar stenosis. The choice of muscles is due to the fact that the gastrocnemius is involved in the movement of the foot in the sagittal plane and helps stabilize the body during movements (running, walking), the tibialis muscle extends, lifts and adducts the foot, and is involved in supination.
When recording and analyzing EMG potential indicators, an initial decrease in the number of active (recruited) motor units and the distribution of potentials over time was noted. The condition worsened significantly after exercise, and pain and intermittent claudication also intensified.
Thus, a decrease in the bioelectrical activity of muscle tissue of the lower extremities, especially after stress tests, is associated with a slowdown, partial or complete blockade of excitation conduction in nerve and muscle fibers.
Treatment
Persistent narrowing of the spinal canal, causing compression of the spinal cord, nerve roots, dysfunction of internal organs, intractable pain syndrome, myelopathy and myeloradiculopathy, requires surgical intervention. The type of surgery depends on the type of stenosis, its location and other anatomical features of the body.
For example, with polysegmental spread of pathology in the lumbar region, a vertebral or radicular decompressive laminectomy is performed on 2-3 segments of the spinal column. A particularly good result and minimal risk of developing spinal instability is shown by surgery in elderly people (over 60 years old) with pronounced rigidity of the muscles and ligaments of the back, but with a certain osteophytosis.
Monosegmental stenosis is operated on using laminectomy or facetectomy at the level of the affected area. In patients with unilateral radicular compression, manifested by neurological symptoms, gentle decompression of the nerve roots can be performed with resection (removal) of the central part of the facet joint and pathological soft tissues (hernias or protrusions of discs, fibrous tissue, hypertrophied ligamentum flavum or posterior longitudinal ligament, etc.) . Lateral stenosis (side) is treated with facetectomy and foraminotomy.
As preventive measures and for the treatment of the initial stages of stenosis, we can recommend: therapeutic exercises, various types of massages, water treatments, swimming, physiotherapeutic procedures, manual therapy.
Author: K.M.N., Academician of the Russian Academy of Medical Sciences M.A. Bobyr
Classification by type
In neurological practice, myelopathy is divided according to etiology:
- spondylogenic – on the spine;
- ischemic – disruption of blood supply to blood vessels;
- post-traumatic – a consequence of mechanical impact with the occurrence of compression on the tissue;
- infectious – for severe bacterial infections (AIDS, syphilis, enterovirus, etc.);
- carcinomatous – against the background of oncology and lesions of the central nervous system;
- toxic – due to intoxication of central nervous system cells or diphtheria;
- radiation – after exposure to radiation (including during the treatment of cancer tumors);
- demyelinating – hereditary or newly acquired demyelization of the central nervous system;
- metabolic - a rare disorder of the metabolism or endocrine system.
Depending on the cause of occurrence, the symptoms of myelopathy may give a different clinical picture.
Types, classification, diagnosis of forms of myelopathy
By the term “myelopathy”, neurologists understand a group of different diseases accompanied by damage to the spinal cord and brain.
Clinical symptoms of the complex of nosologies are characterized by a long course with intervals of relapses and exacerbations. The main task of diagnosing myelopathy is to identify the cause of pathological conditions accompanied by decreased muscle tone, sensory and motor disorders. Modern clinical and instrumental methods (MRI of the brain, angiography, electroencephalography) are sufficient to verify pathological conditions.
MRI of cervical myelopathy
Symptoms of myelopathic processes
Symptoms of the disease are a series of nonspecific neurological manifestations that poorly reflect the etiological picture. Signs directly depend on the severity of damage to the spinal substance. General symptoms for all types of myelopathies:
- paresis, paralysis, muscle hypertonicity;
- hyporeflexia;
- hypoesthesia;
- paresthesia;
- dysfunction of the pelvic region.
Specific symptoms depend on the type of pathology, the presence of factors inherent in the underlying disease (tumors, infections, fractures, intoxication, etc.) and complications associated with this.
Brief information
The described type of pathological deviation of the spinal cord, which has a degenerative-dystrophic nature, has various sources of formation: the presence of a tumor, damage, atherosclerotic lesions, vertebrogenic and dysmetabolic. The most common form in modern neurology is considered to be a vertebrogenic disease - discogenic myelopathy. Based on the name of the disease, we can conclude that the main problem of the anomaly is closely associated with the harmful phenomena occurring in the intervertebral disc.
Often, the disease manifests itself as a result of complications after the onset of osteochondrosis of the vertebral region. According to average statistical data, experts report that people aged 45 to 60 years, in particular males, are most susceptible to the described pathology. When the body is damaged, complaints develop and intensify, which last from several months to long painful years. In fairly rare cases, the presented deviation may occur due to injury. During this process, its acute course begins, and specialists consider it in the form of a post-traumatic form.
Diagnosis of the disease
The diagnostic series involves the identification (exclusion) of processes that are symptomatically similar to myelopathy and the detection of factors that provoked dystrophic spinal changes.
Laboratory diagnostics:
- CBC – general blood test;
- BAC – biochemical blood test.
Instrumental examination of the spinal column:
- X-ray;
- MRI;
- EMG – electromyography;
- ENG – electroneurography;
- lumbar puncture;
- angiography (computer or magnetic).
If it is not possible to do magnetic resonance imaging, then it is replaced by discography and/or myelography. The presumed infectious origin of the disease requires additional clinical studies of the biomaterial:
- blood sterility test;
- RPR sample;
- PCR diagnostics;
- culture of a spinal cord fluid sample.
Based on indications, the patient's neurologist can refer him for a consultation with specialized specialists - a vertebrologist, geneticist, oncologist, etc.
Symptoms and diagnostic methods
Signs are determined by the segment of damage and the main cause.
Basically, typical symptoms are observed:
- The mobility of the limbs is sharply limited.
- Decreased and sometimes increased sensitivity.
- Urinary retention.
- Muscle tone increases.
- Defecation is disrupted.
The picture of the course of the disease of all forms is similar. First, painful sensations appear in the affected area of the spine, and then neurological symptoms develop.
When a disease has a complex genesis, that is, origin, the possibility of other pathologies with similar symptoms should immediately be excluded. Therefore, in addition to examination and palpation, additional research is necessary.
First of all, a laboratory blood test is done (general and determining the amount of inflammatory proteins), and the cerebrospinal fluid is also examined.
As a hardware examination, they are used:
- Radiography. The method allows you to visualize the condition of the bones of the spine.
- MRI. The presence of tumors and the presence of deformation or compression of the spinal cord are detected.
- Electromyography. Assess the level of damage to peripheral nerves and the central nervous system.
Using this diagnostic algorithm, the condition of the spinal cord is determined most reliably.
Treatment of the disease and consequences
Therapeutic tactics are determined by the etiological and clinical picture. It represents a complex of therapeutic measures to eliminate the causative pathology and symptoms.
The most important goal of treatment of compression type pathology is the elimination of compression pressure. For this purpose, the following activities are carried out:
- removal of tumors, hematomas, Urban wedge;
- cystic drainage;
- laminectomy;
- spinal disc puncture;
- Fasectomy;
- micro- or discectomy (for intervertebral hernia).
The ischemic type of myelopathy is based on the exclusion of compressive conditions of the vessels. Since vascular abnormalities are the cause of most myelopathic conditions, the treatment package for almost all patients includes their therapy with special drugs:
- antispasmodics;
- vasodilators;
- supporting blood supply.
The toxic type requires detoxification procedures, and the infectious type requires effective antibacterial treatment. The greatest difficulty is in the fight against the hereditary type of demyelinating pathology and the carcinomatous type with the presence of hemoblastosis. Most often, treatment measures are aimed at relieving symptoms.
The therapeutic course necessarily includes drugs to increase metabolic processes in cells and reduce the risk of hypoxia - neuroprotective, vitamin, and metabolic agents. The treatment course includes physical procedures recommended by a physiotherapist to increase physical activity, prevent bedsores, etc.
Myelopathy of the thoracic and lumbar spine
In the thoracic spine, myelopathy occurs less frequently than in other segments, since the segment is fixed by the ribs and has little mobility. The main cause of the nosological form is a herniated intervertebral disc. The probability of developing the disease exceeds one percent.
The anatomical structure creates difficulties in treatment. The most effective way to treat pathology is surgery. It is important to diagnose using MRI, as medical errors occur when specialists verify thoracic myelopathy in the form of a tumor or inflammatory process. Thoracic disorders due to hernia require careful diagnosis. The test should measure the size of the spinal canal.
Most often, lesions occur in the lumbar region. During walking and carrying heavy objects, this area experiences maximum pressure, leading to degenerative processes and the formation of marginal osteophytes along the contours of the vertebrae. Vertebrogenic spinal syndrome appears in a number of diseases:
- Inflammation of the spinal column;
- Presence of fragments;
- Narrowing of the spinal canal by a tumor;
- Damage to blood vessels;
- Bone destructive changes after injuries.
Chronic vertebrogenic myelopathy develops slowly, but gradually progresses. Inflammatory areas are eliminated using decompression. Surgical intervention is aimed at removing infiltrative fluid and freeing a section of the spinal cord.
Lumbar syndromes develop slowly, but strong compression is accompanied by the rapid formation of a persistent clinical picture.
Spinal infarction is the last stage of spinal injury, accompanied by irreversible changes. Tissue necrosis leads to paralysis of parts of the body that are innervated by the damaged area. The provoking factor of the pathology is vascular thrombosis (formation of blood clots).
Signs of lumbar myelopathy:
- Urinary and rectal disorders occur when spinal nerves are damaged at the lumbar level. Weakness of the abnormal reflex is the first manifestation of compression in the area of the second lumbar vertebra;
- Muscle sensitivity disorder, paresis of the legs, thighs, feet, lower extremities are caused by infringement of the spinal cord at the level of the lumbar, gluteal region;
- Complete paralysis of the limbs is formed due to severe compression of the second lumbar vertebra.
A qualified neurologist will be able to correctly diagnose the level of damage to the spinal column.
Signs of vascular myelopathy
Vascular myelopathy is provoked by degenerative-dystrophic changes in the spine (osteochondrosis, spondylosis), traumatic injuries, and disorders of the blood coagulation system. The pathology is accompanied by loss of sensation in the legs and arms. A disorder of motor innervation is accompanied by paresis and paralysis of muscles.
Impaired blood supply to the arteries leads to muscle weakness and a decrease in the trophic properties of tissues. The condition is called vertebrogenic lumbargia, which causes pain in the hips, knee joints, legs, and feet.
Clinical symptoms of myelopathic syndrome
Specific signs:
- Segmental - linear stripes of increased sensitivity, weakening of tendon reflexes;
- Motor – destruction of the tendon reflexes of Babinsky, Akhilov;
- Vegetative – urinary retention, bladder spasm;
- Painful – pain between the shoulder blades, radicular pain in different parts of the spinal column.
Features of compression myelopathy
The causes of compression of the brain and spinal cord are numerous. The most common etiological factors:
- Displaced vertebral fractures;
- Protrusion of the intervertebral disc into the spinal canal;
- Internal hemorrhage;
- Purulent infections;
- Spinal neoplasms;
- Congenital anomalies of the spinal column in children;
- Complications after spinal puncture;
- Age-related changes.
Spondylogenic pathology occurs after back injuries and cerebral palsy.
Discirculatory myelopathy
Congenital and acquired anomalies of the arteries of the small pelvis, abdomen, and spinal column lead to a dyscirculatory form of the disease. A complex of pathological disorders is accompanied by a sudden contraction of the femoral muscles and loss of sensory sensitivity.
Doctors carry out differential diagnosis of pathology with a group of dangerous conditions:
- Funicular myelosis;
- Amyotrophic lateral sclerosis (ALS);
- Meningomyelitis.
Dyscirculatory disorders are characterized by changes in many internal organs. The absence of specific symptoms precludes early detection.
Ischemic myelopathy
Lack of oxygen supply leads to ischemic changes. Degenerative diseases with morphological disorders lead to pathological disorders:
- Subchondral osteosclerosis of the endplates;
- Cracks, prolapse of intervertebral discs;
- Lack of B vitamins.
Ischemic vascular damage in elderly people is caused by the presence of atherosclerotic plaques and blood clots inside the artery. The anterior horns of the spinal cord are sensitive to hypoxia.
Degenerative myelopathy
A complex of degenerative-dystrophic diseases leads to chronic damage to the spinal cord. The condition progresses over several years. The final result is transverse destruction of the spinal cord with segmental sensory disorders.
Forecast and preventive measures
The prognosis for compression myelopathy is quite satisfactory if areas of tissue compression are detected and eliminated on time. If the disease is ischemic in nature, progression of the disease is possible, but regular therapeutic courses on blood vessels provide stable remission. For the radiation, carcinomatous, hereditary type, the prognosis is usually unfavorable.
To prevent myelopathic processes, it is necessary to prevent and promptly eliminate any disorders associated with vascular and spinal disorders.
You can undergo diagnostics and establish the exact cause of the disease, and receive recommendations for a course of treatment at our medical center. Specialists of the Consultative and Diagnostic Center (formerly the National Diagnostic Center) will help you cope with the developing disease. Click the “SIGN UP” button or call the numbers listed on the website and come see us.
What is the manifestation of discogenic myelopathy?
The main problem that arises with this damage to the body is a gradually increasing deficit of motor and sensory function of a neurological nature. Motor failures are distinguished by low tone and strength of the muscle area, and deformation of tendon reflexes. At points below the levels of myelopathic activity, complaints belong to the spastic sphere, and those places where pathology occurs are peripheral. Problems in the functioning of the sensory function are expressed in a decrease in the degree on the upper and deep layer, paresthesia is formed. In addition, with the presented illness, a person develops unilateral changes at the point where the anomaly was localized. In the future, it is able to switch to a healthy part of the body. At some points, patients are diagnosed with incontinence or, conversely, difficulty urinating. In addition, myelopathy causes radiculitis, but the pain is of moderate severity and takes second place in comparison with motor symptoms.
The cervical variety of the disease consists of the formation of peripheral paresis in the upper extremities and spastic deformities in the lower extremities. Paresthesia on the hands, weak hypoesthesia of the superficial layer, an irregular decrease in the degree of sensitivity in the hands, a decrease or complete loss of all types of sensory properties in the body or legs are noted. The painful condition can cause muscle problems in the proximal areas of the arms. The described pathology can develop in combination with vertebral artery syndrome. In such situations, simultaneously with the symptoms described above, the patient experiences signs of dyscirculatory encephalopathy, that is:
- Conditions of spinning in the head.
- Low ability to remember certain points.
- Vestibular ataxia.
- Presence of noise.
- Sleep problems and more.
The lumbar form of the disease manifests itself in peripheral paresis of the lower extremities, which is accompanied by the appearance of muscle atrophy, low or complete absence of knee and Achilles activity, disturbances in the functioning of the urinary system, as well as sensitive ataxia. Also, experts report that the disease can provoke the formation of intermittent claudication syndrome, which will require differential examination with atherosclerosis and endarteritis of the vascular system of the extremities of an obliterating nature.
List of sources
- Agasarov L., Petrov A. Neurovertebrogenic syndromes // MG. - 2003. - No. 24. - P. 8-9.
- Kamalov I.I. Degenerative-dystrophic changes in the spine / I.I. Kamalov // Vertebroneurology. - 1995. - No. 1-2. — P. 24-31.
- 3abbarova A.T. Centromedullary cervical myelopathy: clinical significance of the spondylogenic factor and the “tight cistern magna” syndrome / A.T. Zabbarova, E.I. Bogdanov // Nevr. messenger Journal named after V.M. Bekhtereva - 2011. -No. 1. - P. 87-90.
- Gorbunov F. E., Penionzhkevich D. Yu. Cervical myelopathy and its treatment by physical factors / To help the practitioner, 2001-N 6, p. 46-50.
- Nekrasov A.K., Nekrasov M.A., Igoshin Yu.A., Seregin A.B., Shevchuk V.V., Gogolev A.Yu. Acute discogenic lumbar myelopathy: clinical characteristics and course options" Bulletin of the Ivanovo Medical Academy T. 12, N° 3-4, 2007
How to get rid of discogenic myelopathy?
In the case of a pathological process with further spread of the described discogenic phenomenon, doctors resort to surgical procedures. To rid the patient of a hernia that was not complicated by the formation of myelopathy, conservative treatment methods are used, for example, dry or underwater traction of the spinal area.
Often, experts use a decompression surgical technique called laminectomy. In some cases, doctors use fastectomy as an addition to get the most effective relief from the pathology. To treat the lumbar perimeter, puncture decompression is suitable. Radial treatment options are required only when large hernias form. In such a situation, specialists perform a discectomy or microdiscectomy.
In the postoperative period, complex therapy is needed that will help restore a person’s strength lost after the body is damaged by myelopathy. To develop motor functions, doctors prescribe pharmacological preparations (vitamin complexes, in particular elements of group B, metabolites and vascular agents), massage sessions, exercise therapy, hydrotherapy using pine, radon and other components, as well as mud therapy and other types of reflexology techniques.
Forecast
In 60% of patients with myelopathy, complete/partial regression of neurological symptoms is observed. In 20% of patients, the condition does not change significantly and remains stable, but functional adaptation to the resulting neurological defect is noted, and in 10% of patients there is progression with a gradual worsening of symptoms.
With chronic compression myelopathies, irreversible destructive changes increase in muscle tissue, nerves and directly in the spinal cord - muscle atrophy , proliferation of connective tissue. Therefore, even in cases where the compressive factor is eliminated, it is impossible to restore full sensory/motor functions, and the resulting neurological disorders are irreversible, which causes disability for the patient.