IVH has recently become a significant problem in pediatric neurosurgery. This is explained by the improvement in the quality of nursing for premature babies with low birth weight. According to the literature, among children weighing less than 2500 g, IVH occurs in 60% of cases. Neurosurgical assistance is required for children with severe IVH, leading to the development of progressive hydrocephalus. The severity of intraventricular hemorrhages directly depends on the degree of prematurity. The year 2012 was marked by the adoption of WHO live birth standards. Currently, babies weighing 500 grams are considered live births. Nursing children with extremely low body weight is significantly complicated by the high incidence of severe IVH among them. This is a category of patients for whom the timeliness and skill of providing assistance to them largely determines the degree of further disability. Providing assistance to this category of patients begins at the stage of the maternity hospital. The visiting team assesses the condition of the newborn patient and assesses his transportability.
The enlarged lateral ventricles of the brain are clearly visible. The severity of the condition is largely explained by severe intracranial hypertension.
In such cases, we begin treatment with a series of lumbar punctures. Contraindications to lumbar puncture may be the presence of occlusion or a bulging blood clot in the lumen of the ventricles. Sometimes it is possible to compensate for the process with a series of lumbar punctures. To reduce ICP we perform ventricular punctures. Multiple ventricular punctures are not advisable, since it has been proven that frequent ventricular punctures lead to the development of porencephalic cysts. Thus, for long-term unloading of the ventricular system, it is often necessary to resort to various drainage operations. For example, ventriculostomy followed by external drainage. This manipulation is performed under ultrasound control in order to visually control the placement of drainage into the lumen of the lateral ventricle. The image clearly shows the catheter in the lumen of the right lateral ventricle.
This image was taken intraoperatively:
This is necessary because drainage is sometimes left standing for a long time. Against the background of drainage, as a rule, hypertensive symptoms are relieved, hemodynamics are normalized, convulsive syndrome is stopped, and breathing is normalized.
The complexity of the situation is that, against the background of various drainage methods, it is extremely rare to achieve final normalization of liquor outflow. This condition is usually resolved by shunt surgery. But here, too, not everything is simple. It is sometimes possible to achieve cerebrospinal fluid sanitization sufficient to install a shunt only after 1-2 months. This turns this category of patients into a big problem for the department. External drainage requires constant attention and poses a serious risk of infection of the drainage system and the development of ventriculitis. For the last 6 years, we have practically not used external drainage in newborns.
Closed drainage techniques are used, such as the subgaleal reservoir and the installation of Omaya type reservoirs. We use these techniques as the first stage of treatment of hydrocephalus in premature infants with IVH, which allows us to delay shunt implantation until the cerebrospinal fluid is completely sanitized.
Subgaleal reservoir.
The essence of the method is to install a silicone catheter into the lateral ventricle and remove it into a reservoir formed under the aponeurosis. Liquor from the ventricular system rushes into the subaponeurotic reservoir, from where it can be periodically evacuated painlessly.
The reservoir is punctured with a thin intradermal needle 1 to 3 times a week, removing accumulated cerebrospinal fluid and introducing solutions of antiseptics and antibiotics. If possible, I transfer the patient to a day hospital for psychological rehabilitation of the mother. The reservoir acts as a receiver, port and shock absorber and allows for control of ventriculomegaly.
The advantage of this technique compared to external drainage is that it allows sanitization of the liquor system with minimal risk of infection and greatly facilitates patient care. Compared to external drainage, we obtained more encouraging results.
Signs and symptoms of cerebral ischemia in newborns
The disease manifests itself with obvious symptoms that attract attention.
- The child is easily excitable, cries for no reason, sleeps poorly, shudders, and has tremors.
- Muscle tone is reduced, the baby moves little, has difficulty sucking and swallowing.
- The fontanel is enlarged, intracranial pressure is increased due to the fact that fluid accumulates in the brain.
- Convulsions, twitching of the limbs and head, as well as comatose states with loss of coordination of movements and consciousness occur.
- The newborn's skin takes on a marbled hue.
- The functioning of the gastrointestinal tract is disrupted - bloating, constipation, and diarrhea are observed.
US – navigation.
Separately, I would like to dwell on interventions using ultrasound navigation. This type of intervention falls into the category of gentle and minimally invasive. If the surgeon is sufficiently qualified under ultrasound control, manipulations can be performed with high precision. If the child is an infant, then the sensor is installed on the membrane of the large fontanel. In older children, the sensor is placed on the dura mater, for which a trefination hole is applied; often this is not required; it is enough to install the sensor on the temporal bone, which remains “transparent” even in adolescents. Below is an example of the complicated course of hydrocephalus with the so-called. isolation of the fourth ventricle.
In this case, ultrasound navigation made it possible to pass the ventricular catheter through the foramen of Monroe, the third ventricle, recanalize the aqueduct and pass it into the fourth ventricle, thus conducting Panventriculostomy:
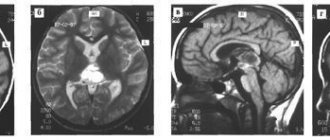
On the presented tomograms, a 10-year-old girl has an extensive cyst in the chiasmatic-sellar region, which impedes the outflow of cerebrospinal fluid through the foramina of Monroe and causes occlusive hydrocephalus.
Under ultrasound control, puncture of the cyst was performed through the foramen of Monroe, followed by catheterization and implantation of the Omaya reservoir. Subsequent tomograms confirm the accuracy of catheter placement. Hydrocephalus has decreased significantly.
Subsequently, regular (once a month) punctures of the reservoir were performed, which ensured relief of hydrocephalus. The child attends a regular school. Control MRI after a year. It can be seen that the cyst retains its volume, but the hydrocephalus has been relieved.
A very important problem in pediatric neurosurgery is the problem of purulent diseases. The most common are rhinogenic complications, as in this case contact abscess of the frontal lobe. CM. snapshot:
This example has more academic significance, because... At one time, as in this case, it was customary to remove abscesses openly in the capsule.
Postoperative photo:
It is clearly visible that the brain is straightened. The lateral ventricle is not damaged. Subsequently, after 6 months. The child underwent cranioplasty surgery. Discharged without neurological deficit.
Currently, we practically do not use removal of an abscess in a capsule. Modern techniques are minimally invasive. We carry out catheterization of the abscess under ultrasound navigation and evacuation of pus, which makes it possible to easily cure even small and deeply located abscesses, as in this case in a teenager with Down's disease.
Introduction
Neonatal intracerebral hemorrhage (ICH) in full-term newborns includes hemorrhages into the brain parenchyma in the first 28 days of life, confirmed by neuroimaging studies or autopsy, in contrast to premature newborns, in whom hemorrhages develop from the germinal matrix [1].
The outcomes of ICH are severe and depend on the area and size of the lesion: severe motor impairment, cognitive deficits, behavioral changes, symptomatic epilepsy, etc. [2]. According to topographical characteristics, IUDs can be located in the cortex, white matter, cerebral hemispheres (most often in one), subcortical formations, and brain stem structures. Most often located in the temporal region. Morphologically, they can be divided into hemorrhages of the type of hematoma or hemorrhagic impregnation. ICH can develop as a result of both traumatic (asphyxia, birth injuries: traumatic damage to blood vessels as a result of deformation and displacement of the brain due to the configuration of the head) and atraumatic (hemocoagulation disorders, thrombocytopathy, leukemia, thrombosis of blood vessels and sinuses, arteriovenous malformations) causes [3] . Also, according to some authors, hemorrhages can be a consequence of previous viral infections, incl. chickenpox, neuroAIDS and acute respiratory viral infections (ARVI) [4, 5].
In accordance with the standards of medical care, all premature newborns, regardless of the presence of neurological symptoms, undergo an ultrasound examination of the brain to detect brain lesions, while in full-term newborns - only if there are appropriate indications. However, according to morphologists, intracerebral hematomas are a common incidental finding during sectional studies of full-term newborns who died from other causes [6].
The purpose of the work was to analyze clinical cases and consequences of asymptomatic ICH in full-term newborns whose mothers suffered acute viral infections during pregnancy.
Clinical case 1
Full-term girl S. from the 1st pregnancy, 1st birth at 40 weeks, born with low gestational weight (2640 g), height 50 cm. At the time of birth, the mother’s age was 24 years. A study of the mother's medical history revealed the presence of hypothyroidism in the stage of medical compensation (hypothyroidism since the age of 18).
In the first and second trimesters (6 and 20 weeks) of this pregnancy, the mother suffered from acute respiratory viral infection (at 20 weeks with a rise in temperature to 38.5°C), complicated by sinusitis. In the third trimester, oligohydramnios was detected at 30 weeks, compensated chronic fetoplacental insufficiency (CFPI) at 40 weeks without circulatory disorders.
Delivery at 40 weeks via vaginal birth. Long waterless period (13 hours 25 minutes), light waters. Chorioamnionitis was diagnosed during childbirth.
The child's condition after birth is satisfactory. Apgar score in the first minute was 7 points, in the fifth – 8.
Routine activities were carried out in the delivery room, skin-to-skin contact, and breast-to-breast contact. The cry is loud, the chest is sucking, the heart rate (HR) is 144 beats/min, the number of respirations is 42 per minute, SpO2 is 90–94%, muscle tone, the range of motor movements is sufficient, physiological reflexes are evoked, unstable. In the neonatal department, the condition remained satisfactory. From the first day, a soft systolic murmur was heard at Botkin's point. Muscle tone is moderately uniformly reduced, reflexes are symmetrical and unstable.
On the fifth day before discharge from the maternity hospital, neurosonography (NSG) was performed, which revealed a focal change in the area of the right thalamus in the form of a highly echogenic zone of round shape with clear contours measuring 7.0×3.8 mm (echo signs of hemorrhage in the right thalamus) . Multilocular subependymal cysts on the right size 14.5×5.7 mm, on the left – 12.6×4.0 mm. Cysts in the middle third of the choroidal plexuses of the right lateral ventricle with a diameter of 7.0 mm, and of the left lateral ventricle with a diameter of 8.7 mm (Fig. 1A).
Cerebral vascular Doppler (DCMA): anterior cerebral artery resistance index (ACA IR) – 0.63 cm/s (normal peripheral resistance), basilar artery resistance index (BA IR) – 0.65 cm/s (normal peripheral resistance) , internal cerebral vein (IMV) – 7.7 cm/s (slight increase in blood flow velocity in the deep veins of the brain), the nature of the Doppler curve is not changed.
Since the maternity hospital was closed for planned treatment, the child was transferred to the Children's Hospital in the children's psychoneurological department on the 6th day and discharged after 9 days. Taking into account the stability of the condition and the small size of this focal change, multislice computed tomography (MSCT) and magnetic resonance imaging (MRI) were not performed.
The condition at discharge was satisfactory, the child was active. I gained weight without vomiting. Hand tremors were noted periodically. Muscle tone is variable. Physiological reflexes in full. Somatic status without features. Body weight at discharge was 2930 g (+619 g).
Infectious immunology using enzyme-linked immunosorbent assay (ELISA): 10 days after birth, immunoglobulin G (IgG) to the Epstein–Barr virus nuclear antigen (EBVNAIgG) was detected; IgM, IgG to cytomegalovirus (CMV), HSV (herpes virus) were not detected.
On the 15th day, during NSG, focal changes in the right thalamus were revealed (echo signs of hemorrhage). Subependymal cysts on the right, left. Left choroidal plexus cyst. DSGM: PMA IR – 0.78, OA IR – 0.84, SMA IR – 0.78, VMV – 8.5 cm/s, laminar flow. Increased peripheral resistance in cerebral arteries.
During a follow-up examination at 3 months by a neurologist, spontaneous motor activity (stiffness, hand tremor) was observed. Cranial nerves (CN) – tongue tremor. Muscle tone is increased in the distal sections. Tendon reflexes are animated, S=D. Physiological reflexes by age. Support on the lower limbs is slightly reduced, with a tendency towards the outer edge and toe. The support on the elbows is slightly reduced. NSG was also performed: a slight expansion of the subarachnoid space in the posterior sections to 4.4 mm. In the sub-ependymal zones of the cyst: on the right – 5×2.5 mm, on the left – 4×4 mm. Moderate increase in echogenicity in the periventricular zones. Heterogeneity of the right visual thalamus due to point echogenic structures with small areas of rarefaction. DSHM: PMA IR – 0.69 cm/s, OA IR – 0.62, VMV – 11.7 cm/s, the nature of the Doppler curve is not changed (Fig. 1B).
The following conclusion was given: pyramidal insufficiency due to perinatal hypoxic-hemorrhagic encephalopathy of moderate severity.
The child is currently under dynamic observation by a neurologist.
Clinical case 2
Full-term girl F. from the 3rd pregnancy, 1st birth at 39.6 weeks. At the time of the child's birth, the mother's age was 26 years. The history revealed syphilis in 2011 (deregistered in 2013), postoperative hypothyroidism in 2021, compensated with medication at the time of pregnancy. Undeveloped 1st pregnancy at 20 weeks in 2021 after resection of the thyroid gland due to postoperative hypothyroidism, 2nd pregnancy – ectopic (tubectomy performed).
In the 1st and 3rd trimesters (13 and 34 weeks), the mother suffered a threatened miscarriage (TPM). In the second and third trimesters (20 and 29 weeks) she suffered from acute respiratory viral infection without fever. Also in the first trimester, marginal placentation and mild anemia were detected; in the third trimester - gestational diabetes mellitus at 27–28 weeks.
Childbirth at 39.6 weeks through the vaginal birth canal, the anhydrous interval was 3 hours 39 minutes, the waters were light. The child was born with a body weight of 3540 g and a height of 54 cm. The Apgar score in the first minute was 8 points, in the fifth minute – 9.
Condition after birth is satisfactory. The cry is loud, heart rate – 142 beats/min, respiratory rate – 42 per minute, SpO2 – 93%, muscle tone, range of movements is sufficient. In the neonatal department, his condition was satisfactory, he absorbed enteral nutrition and sucked the breast well. On the 3rd day, the yellowness of the skin increased, and phototherapy was performed.
When performing NSG on the 3rd day, a focal change in the right temporal region was revealed in the form of a highly echogenic area of rounded shape with clear boundaries measuring 15.1×13.8×9.8 mm, heterogeneous in structure, without a sign of blood flow on color Doppler mapping ( CDK). No dislocation of the middle structures was detected. Cysts of the left choroidal plexus were found in the lower third, measuring 4x4 and 3x3 mm. The lateral ventricles of the brain are slit-like. The external cerebrospinal fluid spaces are not dilated (Fig. 2A).
DSHM: ACA IR – 0.64, OA IR – 0.65, right MCA IR – 0.70, VMV – 5.5 cm/s. Slight asymmetry of blood flow resistance in the ACA and MCA basins (peripheral resistance in the cerebral arteries is not increased). The speed of blood flow in the deep veins of the brain is not changed.
To clarify the nature of the identified changes, MSCT was performed on the 8th day of life: MSCT signs of intracerebral hemorrhage in the right temporal region (9 × 10 × 22 mm) (Fig. 3).
On the 15th day of life, a repeat NSG study was performed: the size of the focal change did not increase, the echogenicity decreased slightly, and the contour was blurred (Fig. 2B).
DSGM: PMA IR – 0.84 cm/s, OA IR – 0.86 cm/s, VMV – 5 cm/s. High vascular resistance in the area of the ACA, OA. The speed of blood flow in the deep veins of the brain is not changed.
On the 21st day, no dynamics of focal changes were detected (Fig. 2B).
Examination by a neurologist on the 5th day: moderate muscle hypotonia, normoreflexia, unstable physiological reflexes. The support reflex is positive. Tendon reflexes are alive, S=D.
Examination by a neurologist on the 10th day: chin tremor. Half-flexion pose. Dystonia of muscle tone. Tendon reflexes are alive, S=D. Physiological reflexes: sucking, proboscis are animated, Babkin, Bauer, automatic gait, Monroe, phase I, phase II, defenses are unstable. The cranial nerves are intact. The shoulder girdle is raised and fixed.
Infectious immunology using ELISA on the 15th day of life: IgG-negative. Antibodies to HSV type 1, 2: IgM-negative, IgG-positive. Antibodies to CMV: IgM-negative, IgG-positive. Increased IgG avidity to CMV.
During NSG at 1 month and 7 days of life, a significant decrease in size, decreased echogenicity, and focal changes in the right temporal region (intracerebral hematoma) were detected. Cysts of the left choroidal plexus (Fig. 2D).
DSGM: PMA IR – 0.80, OA IR – 0.81, VMV – 7.7 cm/s. High resistance of blood flow in the ACA, OA basin. The speed of blood flow in the deep veins of the brain is not changed. The type of Doppler curve is not changed.
Examination by a neurologist in the follow-up room (1 month and 7 days): satisfactory condition, thumb to palm. TBIs are intact. Muscle tone is diffusely reduced, D=S. Tendon reflexes are of medium vivacity, D=S. Physiological reflexes are reduced and unstable. Conclusion: muscle hypotonia due to perinatal hypoxic hemorrhagic encephalopathy, moderate. Delayed speech development.
The child continues to be monitored by a neurologist.
Clinical case 3
Girl T. from the 2nd pregnancy, 2 abdominal births at 37–38 weeks, born with low gestational weight (2340 g), height 49 cm. At the time of birth, the mother’s age was 27 years.
From the woman’s medical history it is known that the first pregnancy ended in childbirth at 30 weeks. The woman is a carrier of homozygous MTYFR PAI1 polymorphism. No changes in the coagulogram were detected during observation by a hematologist during pregnancy. According to the hematologist, there was no need for hemostasis correction. Homocysteine – 6.76 µmol/l (normal – 2.90–11.00).
In the first trimester, pregnancy proceeded without pathology. In II there was circulatory disorder 1A at 25 weeks. In the third trimester, the mother suffered from chickenpox at 30 weeks and gestational diabetes mellitus at 34–35 weeks.
Abdominal birth at 37–38 weeks. The child's condition after birth is satisfactory. The Apgar score in the first minute is 8 points, in the fifth minute it is 8.
Routine activities were carried out in the delivery room, skin-to-skin contact, and breast-to-breast contact. The cry is loud, the chest is sucked, there is a moderate uniform decrease in muscle tone, unstable physiological reflexes.
On the 3rd day, NSG was performed: focal changes were revealed in the form of zones of high echogenicity with clear boundaries in the cortical sections of the parietal region, local expansion of the grooves in the convexital sections with echogenic content. Subependymal cyst on the left. Choroid plexus cyst on the left. Increased peripheral resistance in cerebral arteries (Fig. 4A). The child was transferred to the second stage of neonatal care for observation and monitoring of the condition. During control sonographic studies on the 8th day: no increase in focal changes was detected (Fig. 4B).
Infectious immunology using ELISA on the 12th day: antibodies to the capsid antigen of the Epstein-Barr virus (Ig VCA) were detected, avidity - 87%, IgG to CMV, avidity - 81%, Ig G to the herpes simplex virus (HSV), avidity - 91%.
At discharge, the patient’s condition was satisfactory, moderate muscle hypotonia remained, she absorbed enteral nutrition well, did not regurgitate, weight gain was +350 g. She was discharged on the 16th day of life.
NSG in the follow-up room:
- at 1 month – the conclusion is the same, in dynamics the echogenicity of the described focal changes has decreased significantly;
- at 3 months – no focal changes were detected, cortical zones without features. The subarachnoid space is 2.1–2.9 mm, the interhemispheric fissure in the anterior sections is 2.5 mm, in the posterior sections it is single-circuit. Subependymal cyst on the left. Choroid plexus cyst on the left.
DSGM: PMA IR – 0.67, OA IR – 0.65, VMV – 10 cm/s.
Now the child is 1 year and 5 months old: according to his mother, he walks well, learns to jump, eats with a spoon, speaks 20 words, plays with toys, puts them in a box, has good onomatopoeia, names body parts.
Discussion
This article presents cases of intracerebral hemorrhages of various locations found in newborns of the physiological department during routine echographic screening in the first 2–5 days of life, who were born with a good Apgar score and did not have cerebral dysfunction.
Sonography of newborns was performed on PHILIPS CX 50 devices with a microconvex sensor with a frequency of 5-8 MHz and a LOGIQ-e linear sensor with a frequency of 10-13 MHz through natural acoustic windows: anterior fontanel, anterolateral, posterolateral fontanel.
In the given clinical examples, there are hemorrhages in the subcortical structures (thalamus), in the deep white matter of the brain (temporal region of the right hemisphere), and cortical parts of the brain.
Children were born to young mothers whose pregnancy occurred against the background of a viral infection and endocrine-metabolic syndrome (hypothyroidism, postoperative hypothyroidism, drug-compensated, gestational diabetes mellitus). In various cases, childbirth was complicated by chorioamnionitis and a long anhydrous interval.
In all clinical cases, there was no evidence for the traumatic nature of childbirth and the presence of birth injuries (large birth tumor, excessive head configuration, asymmetrical head configuration, cutaneous hemorrhagic syndrome, as well as skull fractures and cephalohematomas, see table).
Thus, in the analyzed cases, the newborns did not suffer asphyxia during childbirth, there were no severe respiratory disorders, decompensated or compensated acidosis, significant hemodynamic disturbances during labor or after birth, which could lead to ischemic or hemorrhagic damage in the brain and cause cerebral vascular disease. disasters.
After birth and subsequently, the general condition of the newborns did not suffer; the children sucked well and absorbed enteral nutrition. The neurological status included moderate muscle hypotonia, unstable physiological reflexes, and hand tremor.
Subsequently, during follow-up observations of children, these focal changes in the brain were either not detected or significantly decreased in volume. Dynamic echographic studies did not form porencephalic cysts, but revealed a tendency to increase peripheral resistance in the cerebral arteries, asymmetry of blood flow in the arteries of the circle of Willis and a slight expansion of the external liquor spaces. In the neurological status, there was a decrease or increase in muscle tone and reflexes, moderately pronounced signs of pyramidal insufficiency, and a moderate delay in speech development.
According to the literature, in 38% of children with congenital viral infection, neuroimaging reveals periventricular ICH [7]. The pathogenetic factor of hemorrhagic brain lesions in children whose mothers suffered an infectious disease during pregnancy may be the tropism of viruses to all epithelial cells, incl. to the endothelium of cerebral vessels. This leads to changes in the characteristics of the vascular walls, the development of vasculitis and, as a consequence, to ICH [3].
All children are currently undergoing dynamic observation by a neurologist.
conclusions
ICH in full-term newborns can be asymptomatic and develop against the background of infections in mothers during pregnancy, and therefore for early diagnosis it is necessary to introduce neuroimaging screening in full-term newborns at risk in all maternity hospitals for timely diagnosis, early initiation of therapy and improved outcomes in the recovery period.
Treatment of cerebral ischemia in newborns
The goal of treatment is to restore normal blood circulation in the brain tissue, prevent pathological changes and eliminate the consequences of ischemia. For stage 1 disease, treatment usually involves prescribing massage to improve blood circulation.
For diseases of the 2nd and 3rd degrees, drug therapy and surgery are used to remove a blood clot in the vessel and restore the structure of the vascular bed. In difficult cases, the baby undergoes a rehabilitation course of intensive therapy.
Risk factors
Various vascular and neurological pathologies, problems with blood pressure (especially hereditary) in the mother should alert the doctor who is managing the pregnancy. Also, risk factors for cerebral ischemia in a child are:
- mother's age is more than 35 years;
- endocrine diseases;
- premature, prolonged labor;
- multiple pregnancy;
- late toxicosis;
- failure of the mother to follow a healthy lifestyle;
- exacerbation of chronic or acute diseases in the mother during pregnancy.
Prognosis and consequences of cerebral ischemia
It is much more effective to eliminate ischemia itself after the birth of a baby than to treat its complications. Among the consequences of cerebral ischemia of the 2nd degree:
- sleep disorders;
- headache;
- irritability;
- isolation;
- physical inactivity.
- Stage 3 disease has severe consequences:
- cerebral palsy;
- attention deficit disorder;
- mental retardation;
- Graefe's symptom, etc.
If all actions to eliminate ischemia were carried out by doctors in a timely manner, then the symptoms disappear during the rehabilitation period, which usually lasts 6-12 months.
How does cerebral ischemia occur?
In 70% of cases, ischemia occurs in the fetus in the womb and is associated with the formation of a blood clot in one of the vessels supplying the brain, or with insufficient development of the vessel. Most often, the disease is diagnosed in premature babies whose vascular system is not yet fully formed.
As a result, an insufficient amount of blood enters the vital organ, and with it, oxygen. Delay in providing medical care leads to damage to larger areas of the brain, cerebral hemorrhage and other serious consequences.
Cerebral ischemia grade 2
A dangerous form of the disease. It is characterized by:
- severe apnea (stopping breathing during sleep);
- decreased grasping and sucking reflexes;
- weak muscle tone;
- increase in head shape due to fluid accumulation;
- lack of coordination;
- loss of consciousness;
- changes in skin color.
Most often, grade 2 ischemia manifests itself in the first day of a newborn’s life, and symptoms can be observed for 2-4 weeks. At this time, the child is carefully monitored by doctors, and he undergoes a course of therapy. If necessary, surgery is performed to remove the blood clot.