The brain is one of the most complex structures studied in physiology. It consists of several parts, each of which is unique and no less difficult for science. The brainstem, which is a part of the brain, seems to be its most interesting component, because responsible for the functioning of many systems. In recent years, scientists have been able to study it in detail and give precise characteristics. Knowledge of the structure and functions of the brain stem will allow you not only to increase your erudition, but also to avoid some diseases associated with the head.
Stem section
The first living beings to appear on Earth had only a medulla oblongata. It was he who provided them with all the necessary instincts that helped them survive. But this is not enough, because... they needed to constantly develop their reflexes and thinking. After some time, new organisms began to be born with larger brains. Such changes occurred shortly before the appearance of man, with whom the formation of the cerebellum occurred. The remaining parts of the brain began to form only hundreds of years later.
The brain stem, which appeared during evolution, was responsible for ensuring respiratory function and blood supply to all necessary parts of the body. As it developed, it began to consist of a huge number of different centers, which began to form a very complex system. Now this section is a necessary part of the brain, without which life is impossible.
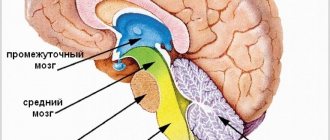
It is located between the large opening of the head in the occipital region and the slope of the inner part of the skull. The trunk extends the spinal cord, connecting it with the main one located inside the head. Its length is about 7 cm, and it includes several separate parts that are very important for the body.
How and why was the brain stem formed?
All the functions of the stem department have long been defined. His research is carried out by neurophysiologists, anatomists and other doctors. The basis for the emergence of a full-fledged trunk was the medulla oblongata. The brain stem is a very complex system in which many processes occur simultaneously.
The first creatures that came onto land had only a medulla oblongata, which allowed them to be guided by primitive instincts. During evolution, it was necessary to improve reflexes, reactions and thinking. The big brain appeared much later, when animals already had thinking. After the appearance of erect man, the cerebellum formed in the cranium. And with subsequent generations, the brain acquired more and more convolutions, cortex, nerve nuclei and other elements that are characteristic of modern man.
Useful to know: Convolutions and grooves located in the brain: structure, functions and description
Now the main tasks of the trunk are to ensure breathing and blood circulation, and their regulation. The structure fully supports human life, so pathologies are extremely dangerous. Cerebral edema is quite dangerous. In this case, the barrel moves lower, where it is clamped in the occipital foramen. Then full functioning is impossible, which causes a lot of consequences.
to contents ^
Anatomical features
The brain is a complex organ that acts as the center of the human nervous system. Scientists estimate that it may contain more than 20 billion different neurons that transmit signals to other parts of the body. The brain stem includes several sections, each of which is responsible for specific functions. There are 5 of them in total:
- Oblong;
- Intermediate;
- Rear;
- Average;
- Finite.
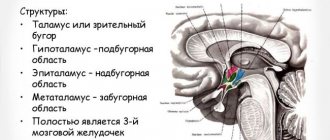
Anatomy also involves the identification of several equally important parts: the cerebral cortex, the cerebellar cortex, the vermis with nuclei, the pons, the thalamus, the hypothalamus, the pituitary gland, the basal ganglia.
The structure itself presents the following picture:
- The medulla oblongata acts as a continuation of the spinal cord, emerging from the vertebral region. It contains two types of substance: white and gray. The function of the first is to conduct information between body systems. The second is the nerve nuclei, which mature by age 7.
- Valoriev Bridge. It is the next section emerging from the medulla oblongata, located in the middle part of the trunk, formed by the base, quadrigeminal, components of the cranial ventricles and tegmentum. Consists of longitudinal and transverse fibers. The former are built from neural clusters, presented in the form of nuclei, from which the latter pass. The latter include the upper and lower layers, through which pyramidal paths are laid.
- Cerebellum. It consists of small hemispheres that are covered with white and gray matter. Reaches its maximum size by the age of 15.
- Midbrain. Attached to the cerebellum by two peculiar legs, it includes 2 visual and 2 auditory sections in the form of separate tubercles through which nerve fibers pass.
- Hemisphere cortex. Between the hemispheres is the corpus callosum, which provides communication between all parts. All thought processes take place in the cortex.
The structure of the brain stem includes another significant section. It is called the reticular formation, which includes dendrites and axons that form the reticulum, which is a special network. The main function of this area is to manage information transmitted from the brain to other parts of the body. There are 2 types of information conduction: afferent, which directs data to the formation, and efferent, which performs the opposite effect.
The brain is well protected. Three shells are responsible for this: soft, hard, arachnoid. Additional protection is provided by the surface of the skull.
Interaction with other parts of the brain
The human central nervous system is a unique formation, under the control of which all internal systems of the body function, be it breathing or heartbeat.
An important role in this is played by the brain stem, which contains nuclei - the nerve centers of the corresponding structures.
With the help of them, the human body, at the subconscious level, carries out various reflexes that are under the control of the brain stem, and maintains the constancy of the internal environment, senses aromas, hears, sees and touches the world around us.
Cranial nerve nuclei
One of the most important components of the brain stem is the cranial nerve nuclei, which extend from its base. They are located between the rear and oblong parts, with a small number of them located on the bridge. The nuclei consist of nerve endings that have a direct effect on the trunk. They are presented in the form of branches that penetrate through its most important parts.
Each core has its own purpose. The following nerves emerge from this zone:
- Olfactory;
- Visual;
- Oculomotor;
- Facial;
- vestibulocochlear;
- Block;
- Discharge;
- Trigeminal;
- Glossopharyngeal;
- Sublingual;
- Additional;
- Wandering.
Their full functioning is very important for the human body. Dysfunction of any nerve can have serious consequences that impair quality of life and even lead to death.
Chain reflexes
Chain reflexes also occur in the brainstem. This happens if several pairs of cores are activated simultaneously.
Oculomotor reflexes coordinate gaze. The impulse is transmitted through the cochlear and ternary nerves to the nuclei. The direction of gaze involves the oculomotor, lateral and abducens nerves. The process is monitored by the reticular formations, the cerebellum and the cerebral cortex.
The act of chewing occurs due to contractions of the extensor muscles of the lower jaw. The impulse is transmitted along the ternary nerve. In the medulla oblongata near the pons there is a center that is responsible for the entire chewing process. Afferent signals excite the motor neurons of the masticatory muscles, which raise and lower the movable jaw.
The act of swallowing moves food that has entered the oral cavity into the digestive tract. First, the receptors of the tongue root are excited, then the palate. When food is already in the throat, receptors in the pharynx are activated, which help direct food into the esophagus. This act is ensured by the swallowing center, which is connected to the respiratory center.
Cough is a protective reaction of the human body to irritation in the trachea, larynx or bronchi. The vagus nerve carries an impulse to the cough center. The nucleus is located in the medulla oblongata and is directly connected to the respiratory center. First, take a deep breath. The glottis is closed and the expiratory muscles contract to exhale. This creates high pressure, followed by a sharp exhalation when the glottis opens. The air flow passes exclusively through the mouth.
The sneeze reflex is also protective. In the mucous membrane of the nasal cavity, irritation of the ternary nerve occurs. The sneezing center is located near the cough. The whole process happens the same way, only the air flow comes out not through the mouth, but through the nose.
to contents ^
Functions
All parts of the brain stem are equally necessary. They provide people with the opportunity to smell, hear sound, understand speech, think about any serious things. If not for them, humanity could have remained in the Stone Age forever.
The functions of the brain stem are reduced to the distribution of information between the brain and the central nervous system. They are provided by nuclei and nerve endings. In this case, the trunk is a physiological connecting step between the spinal cord and the brain. If it is damaged, then signals from the brain will not be able to reach the end point, which will completely eliminate the normal functioning of the human body.
There are several groups of functions that are characteristic of the brain stem. Among them:
- Motor. This includes all actions associated with the muscles of the eyes and eyelids. The function is also responsible for the reflexes of the eyeballs and controls the chewing muscles.
- Sensitive. Ensures the functioning of taste buds, as well as all reflexes that affect the digestive system. Helps transmit signals for swallowing and many other actions, including even vomiting. Additionally responsible for sneezing.
- Parasympathetic. Affects movement and dilation of the pupils, controls the ciliary muscles. Managed by cores, ensuring the execution of a block function.
- Upper salivary. It affects the salivary glands, ensuring timely and necessary formation of saliva.
- Vestibular. Responsible for the functioning of the vestibular apparatus, which helps control body balance and stay on your feet.
- Swallowing. Ensures the swallowing reflex works. Complements the work of the sensitive function.
- Auditory. Transmits information to the cerebellum, is responsible for hearing, as well as recognizing heard sounds.
- Sensory. Gives sensitivity to the skin on the face, analyzes taste and sound, and recognizes vestibular stimuli.
The brain stem has the most important functions. It gives every person the opportunity to hear, feel, see, move, think. All of them are necessary for a full life.
If you distribute individual functions across parts of the brain stem, you get the following:
| Brainstem region | Functions |
| Midbrain | · Functioning of visual and auditory organs; · Management of relevant bodies; · Orientation in space. |
| Medulla | · Reflexes associated with coughing, vomiting, sneezing; · Breath control; · Cardiovascular system management; · Functioning of the digestive tract. |
| Pons | · Providing blood supply to the brain; · Fast transmission of signals between the brain and the central nervous system. |
| Cerebellum | · Coordination of movements, balance; · Muscle tissue tone. |
| Diencephalon | · Function of the thyroid gland; · Control of the adrenal glands. |
The importance of such functions makes us take the condition of the brain stem more seriously. He is no exception and may be susceptible to various life-threatening diseases.
If there are disturbances in one section of the trunk, failures may occur in others, because they are all closely interconnected.
Neurokinesiology
Brain stem
Admin
09.01.2019
Uncategorized
Brain stem
(truncus encephali; synonym for brain stem)
part of the base of the brain containing the nuclei of the cranial nerves and vital centers (respiratory, vasomotor and a number of others). S. g. m. has a length of about 7 cm, consists of the midbrain, bridge (pons) and medulla oblongata and is located behind the slope of the internal base of the skull to the edge of the foramen magnum. Extends between the cerebral hemispheres and the spinal cord (Fig.).
The midbrain (mesencephalon) is formed ventrally by the left and right cerebral peduncles, dorsally by the quadrigeminal, consisting of the superior and inferior colliculi; Cranially it borders with the diencephalon, caudally passes into the pons, and through the superior cerebellar peduncles it connects with the cerebellum. The third and fourth pairs of cranial nerves emerge from the midbrain.
The pons, the middle thickened part of the brain stem, forms the middle cerebellar peduncle in the dorsolateral direction and borders caudally with the medulla oblongata. The ventral surface of the medulla oblongata is formed by the pyramids and the olives lying dorsolateral to them. On the dorsal surface of the medulla oblongata, wedge-shaped and gentle tubercles and the lower cerebellar peduncles are distinguished. The dorsal surface of the pons and medulla oblongata forms the bottom of the fourth ventricle - the rhomboid fossa. The V-VIII pairs of cranial nerves emerge from the pons, and the IX, X, XII pairs emerge from the medulla oblongata.
In transverse sections of the brainstem in the ventrodorsal direction, the base, tegmentum, parts of the ventricular system (the midbrain aqueduct and the fourth ventricle), the roof of the midbrain (quadrigeminal) and the roof of the fourth ventricle are distinguished. The base is represented by the bases of the cerebral peduncles, the ventral part of the pons and the pyramids of the medulla oblongata, formed by fibers of the motor tracts: cortical-cerebellar and pyramidal (see.
Pyramid system). The tegmentum consists of the nuclei of the cranial nerves (III-XII pairs), the reticular formation, sensitive ascending tracts (see Pathways), nuclei and conduction tracts of the extrapyramidal system (Extrapyramidal system).
The motor and parasympathetic nuclei of the cranial nerves (Cranial nerves) are located in the medial part of the tegmentum. The nuclei of the nerves of the muscles of the eyeball (III, IV, VI pairs), as well as the innervating muscle of the tongue (XII pairs) are located near the midline, ventral to the cerebral aqueduct and the bottom of the IV ventricle. The parasympathetic nuclei of the VII, IX and X cranial nerves (superior and inferior salivary, dorsal nucleus of the vagus nerve) lie lateral to the motor ones, and the accessory oculomotor nucleus (accommodation center) occupies a dorsal position in the complex of nuclei of the III pair. The motor nuclei of the nerves of the visceral arches (V, VII, IX, X pairs) lie ventral to the parasympathetic nuclei of the trunk and innervate the masticatory and facial muscles, the muscles of the pharynx and larynx.
The sensitive nuclei of the trunk occupy the side parts of the tire. The nucleus of the solitary tract (VII, IX and X pairs), located in the medulla oblongata, receives interoceptive impulses from the taste buds of the tongue, the mucous membrane of the pharynx, larynx, trachea, bronchi, esophagus and stomach, from the receptors of the lungs, carotid corpuscle, aortic arch and right atria. The pontine and spinal nuclei of the V pair receive exteroceptive impulses from the scalp and face, the conjunctiva of the eyeball, from the mucous membrane of the mouth, nose, paranasal sinuses and tympanic cavity. The midbrain nucleus of pair V receives impulses from the proprioceptors of the head muscles. The cochlear and vestibular nuclei receive impulses from the organ of Corti and the statokinetic apparatus through the VIII pair of cranial nerves.
The reticular formation, which lies between the nuclei of the cranial nerves and the pathways, passes caudally into the intermediate substance of the spinal cord and rostally reaches the subthalamic region and the intralamellar nuclei of the thalamus. The lateral (sensory and associative) and medial (effector) parts of the reticular formation, together with the nuclei of the cranial nerves, form complex functional systems (respiratory and vasomotor centers), regulate muscle tone and ensure the maintenance of posture, integrate complex reflexes (gag, swallowing), and participate in processing and modulation of primary afferent information (endogenous analgesic system), affect the cerebral cortex (activating ascending system).
The left and right parts of the medulla oblongata are supplied with blood by branches of the vertebral arteries: from the ventral surface - the medial and lateral cerebral and anterior spinal arteries, from the dorsolateral - the inferior posterior cerebellar arteries. Branches of the basilar artery supply blood to the bridge (pontine arteries, cerebral peduncles (midcerebral arteries) and the roof of the midbrain (superior cerebellar and posterior cerebral arteries).
Research methods. To diagnose S.'s lesions, clinical and instrumental laboratory methods are used. The first group includes neurological studies of the functions of cranial nerves, voluntary movements of the limbs and the coordination of these movements, sensitivity, and autonomic-visceral functions.
Instrumental and laboratory methods include spinal puncture (Spinal puncture), suboccipital puncture (Suboccipital puncture) followed by laboratory examination of cerebrospinal fluid (Cerebrospinal fluid), radiography of the skull (see Skull), pneumoencephalography, ventriculography, rheoencephalography (Rheoencephalography), Doppler ultrasound, echoencephalography Iyu (Echoencephalography), electroencephalography (Electroencephalography) (with evoked potential), which allows recording the bioelectrical activity of certain areas of the brain stem; radionuclide studies (see Radionuclide diagnostics), computed tomography (Tomography) and nuclear magnetic resonance imaging, which make it possible to visualize the pathological focus, clarify its nature and prevalence.
Pathology. The variety of clinical manifestations of S.'s lesions depends on the location and size of the focus of the pathological process. The most common topical diagnostic signs of midbrain damage are alternating syndromes, various oculomotor disorders, disorders of consciousness and sleep, and decerebrate rigidity. When the lesion is localized at the base of the midbrain, conduction disorders predominate. Alternating Weber syndrome develops, characterized by damage to the oculomotor nerve on the side of the lesion and hemiplegia with central paresis of the muscles of the face and tongue on the opposite side.
Sometimes, with vascular lesions of the midbrain, a syndrome occurs due to simultaneous damage to the superior cerebellar peduncle, spinothalamic tract and quadrigeminal tract, with choreiform hemiathetoid hyperkinesis observed on the side of the lesion and a disorder of pain and temperature sensitivity on the opposite side.
Lesions of the nuclei of the oculomotor nerve cause drooping of the upper eyelid, limitation of movements of the eyeball up, down, inward, divergent strabismus, double vision, pupil dilation, impaired convergence and accommodation.
When the tegmentum of the midbrain is damaged, upward or downward gaze paralysis develops (impaired function of the posterior longitudinal fasciculus) or vertical pendulum-like movements of the eyeballs, sometimes developing in a state of coma. If the posterior longitudinal fasciculus is damaged, conjugal eye movement may be impaired.
Pathological processes in the midbrain lead to impaired muscle tone. Damage to the substantia nigra causes Akinetic-rigid syndrome. When the diameter of the midbrain is damaged at the level of the red nuclei, decerebrate rigidity syndrome may develop. With extensive, often vascular, processes in the midbrain involving the nuclei of the reticular formation, disturbances in wakefulness and sleep often occur. Sometimes “peduncular hallucinosis” is observed, accompanied mainly by visual hallucinations of the hypnagogic type: the patient sees figures of people and animals and maintains a critical attitude towards them.
Unilateral lesions in the pontine region also cause alternating syndromes. When the middle and upper part of the base of the bridge is affected, contralateral hemiparesis or hemiplegia develops; with bilateral damage, tetraparesis or tetraplegia develops. Pseudobulbar syndrome occurs quite often. Millard-Hübler syndrome is characteristic of lesions of the caudal part of the base of the bridge.
A lesion in the caudal third of the pontine tegmentum is accompanied by the development of Foville syndrome: homolateral damage to the VI and VII cranial nerves (in combination with gaze paresis towards the lesion). When the caudal part of the tegmentum is affected, Gasperini syndrome is described, which is characterized by homolateral damage to the V, VI, VII cranial nerves and contralateral hemianesthesia.
With extensive, often vascular, processes in the area of the tegmentum of the brain, occurring with damage to the activating part of the reticular formation, disturbances of consciousness of varying degrees often develop: Coma, stupor, Stupefaction, akinetic mutism.
With pathology of the medulla oblongata, the most characteristic is Bulbar palsy. Often, lesions of the pyramidal tract at the level of the medulla oblongata cause hemi- or tetraplegia (see Paralysis). Often, lesions of the pyramidal tract involve the nuclei and roots of the IX, X, XII cranial nerves, and bulbar alternating syndromes develop.
Damage to the ventral part of the lower half of the medulla oblongata is characterized by the appearance on the side of the lesion of segmental dissociated anesthesia in the caudal dermatomes of Zelder on the face, a decrease in deep sensitivity in the leg and arm, the development of hemiataxia and Bernard-Horner syndrome; on the side opposite to the lesion, conduction hemianesthesia is noted with an upper border at the level of the upper cervical segments.
Damage to the nuclei of the reticular formation is accompanied by respiratory distress (it becomes frequent and irregular), cardiovascular activity (tachycardia, cyanotic spots on the limbs and torso), thermal and vasomotor asymmetry in the acute phase.
Of the pathological processes in the brainstem area, ischemic lesions due to transient cerebrovascular accidents and infarctions as a result of occlusive, usually atherosclerotic, damage to the vessels of the vertebrobasilar system at various levels are more common (see Cerebral circulation), hemorrhages developing as a result of arterial hypertension are less often observed. Ischemic lesions of the brain stem (see Stroke) are characterized by a scattering of several, usually small, foci of necrosis, which determines the polymorphism of clinical manifestations. With the development of an ischemic focus in the area of the brain stem, along with paresis of the extremities, nuclear damage to the cranial nerves develops (oculomotor disorders, nystagmus, dizziness, dysarthria, swallowing disorders, impaired statics, coordination, etc.), sometimes these symptoms manifest themselves in the form of alternating syndromes.
Infarctions in the midbrain region can be primary or secondary, caused by dislocation of the brain with transtentorial herniation during various supratentorial space-occupying processes. The most characteristic of midbrain infarction is the inferior red nucleus syndrome: paralysis of the oculomotor nerve on the side of the lesion, ataxia and intention tremor in the contralateral limbs, sometimes choreiform hyperkinesis is observed. If the oral parts of the red nucleus are damaged, the oculomotor nerve may not be affected.
With a heart attack in the medulla oblongata, there are two main options. When the lateral and medial cerebral branches of the vertebral and basilar arteries are blocked, medial medulla oblongata syndrome develops: paralysis of the hypoglossal nerve on the side of the lesion and paralysis of the opposite limbs (Jackson syndrome). When the vertebral and inferior posterior cerebellar arteries are blocked, Wallenberg-Zakharchenko syndrome occurs, which is characterized by paralysis of the muscles of the soft palate, larynx, tongue and vocal muscles on the side of the lesion; on the same side, dissociated segmental anesthesia of the facial skin, impaired deep sensitivity with selective ataxia are observed in them, cerebellar hemiataxia, Bernard-Horner syndrome. Due to damage to the spinothalamic tract on the opposite side, conduction hemianesthesia is detected.
Clinically, hemorrhages in the brainstem are characterized by disturbances of consciousness and vital functions, symptoms of damage to the nuclei of the cranial nerves, and bilateral paresis of the limbs (alternating syndromes are sometimes observed). Strobism (strabismus), anisocoria, mydriasis, fixed gaze, “floating” movements of the eyeballs, nystagmus, swallowing disorders, bilateral pyramidal reflexes, cerebellar symptoms are often observed (see Cerebellum). With hemorrhages in the bridge, miosis and paresis of gaze towards the lesion are noted. An early increase in muscle tone (Hormetonia, decerebrate rigidity) occurs with hemorrhages in the oral parts of the brain stem. Lesions in the lower parts of the trunk are accompanied by early muscle hypotonia or atony.
The diagnosis is made based on medical history, clinical manifestations, and additional examination methods. Differential diagnosis must be made with apoplectiform syndrome during myocardial infarction, acute development of a tumor or edema of the brain, traumatic brain injury, hemorrhagic meningoencephalitis, disorders of consciousness of various etiologies.
Therapeutic measures are carried out immediately and differentiated, taking into account the patient’s condition and the nature of the pathological process. Early hospitalization of patients is necessary. Patients in a state of deep coma and with severe impairment of vital functions cannot be transported. Emergency care is aimed at correcting the vital functions of the body: treatment of cardiovascular disorders, respiratory failure (changing the patient’s position, suctioning secretions from the trachea and bronchi; if these measures are ineffective, intubation and tracheostomy), maintaining homeostasis, combating cerebral edema.
The prognosis depends on the nature of the vascular process, its topic, size, and rate of development of complications. The most favorable prognosis is for limited brain stem infarctions in young people.
Rehabilitation includes exercise therapy, massage, classes with a speech therapist, drug therapy using drugs that improve metabolic processes in brain tissue (aminalon, Cerebrolysin, piracetam, etc.).
Infectious lesions of S. g. m. are primary and secondary. Among the primary ones, neuroviral lesions are more common than others: poliomyelitis, poliomyelitis-like diseases. In this case, paralysis of the muscles of the face, tongue, pharynx, and larynx is observed. In infectious-allergic processes, for example, the bulbar form of Guillain-Barré polyradiculoneuritis, against the background of a severe general condition and meningeal symptoms, signs of damage to the IX-XII cranial nerves on one or both sides and changes in the cerebrospinal fluid (cerebrospinal fluid) (protein-cell dissociation) appear. The bulbar form of neuroviral diseases is the most dangerous, because often leads to cessation of breathing and cardiovascular activity. Treatment: drugs with antiviral activity (deoxyribonuclease, ribonuclease, interferon), glucocorticoids, detoxification agents (gemodez, neocompensan) and symptomatic, with increasing respiratory failure, artificial ventilation of the lungs is carried out, in the recovery period - drugs that improve metabolism, anticholinesterase drugs, massage, Exercise therapy.
Secondary inflammatory lesions of the brain stem can occur with syphilis, tuberculosis, influenza, etc. In these cases, the nuclear formations of the brain stem, pyramidal tract, sensory conductors, and coordination system are affected.
Inflammatory processes of various nature - Encephalitis can cause oculomotor disorders, sleep disturbances, muscle tone, akinetic-rigid syndrome, and occasionally bulbar palsy. Often there is damage to the brain stem in multiple sclerosis, which is expressed by oculomotor disorders, nystagmus and dysfunction of conductive structures, especially the pyramidal tracts.
The medulla oblongata is affected by syringobulbia (see Syringomyelia). In the clinical picture of syringobulbia, the most typical symptom is dissociated sensitivity disorders on the face of a segmental type (decreased sensitivity in the lateral parts of the face). Dizziness, nystagmus, and static ataxia are observed due to damage to the vestibular nuclei in the trunk. Often the nuclei of the bulbar group of cranial nerves are involved in the process; sometimes autonomic crises are observed in the form of tachycardia, respiratory failure, and vomiting. The danger is respiratory distress due to Stridor, caused by paralysis of the larynx. Treatment is symptomatic.
Amyotrophic lateral sclerosis (Amyotrophic lateral sclerosis) is characterized by damage to the IX, X, XII pairs of cranial nerves in the S. g. m. Disorders of swallowing, articulation, phonation, restriction of tongue movement, atrophy and fibrillary twitching in it appear and increase.
Isolated brainstem injuries are rare and are more common with severe traumatic brain injury (traumatic brain injury). In this case, loss of consciousness develops, there may be a deep coma, respiratory and cardiac problems. Symptoms of cerebral ischemia and hypoxia appear with the development of cerebral edema (cerebral edema). In some cases, tonic convulsions are possible. With less severe injuries, nystagmus, decreased corneal and pharyngeal reflexes, changes in tendon reflexes and the appearance of pathological reflexes are observed. Emergency care is aimed at correcting respiratory and cardiac disorders. The prognosis depends on the severity of the damage and the completeness of treatment measures.
Brain stem pathology is often caused by intracranial tumors. The clinical picture and symptoms of brain stem lesions due to tumors depend on their location and damage to certain nuclei and pathways.
In the midbrain, the most common are gliomas and teratomas (see Brain, tumors), which first cause internal hydrocephalus due to compression of the cerebral aqueduct, then headache, vomiting, and swelling of the optic discs (see Occlusive syndrome). Damage to the upper part of the midbrain causes upward gaze paresis, combined with convergence paresis (Parinaud's syndrome). Anisocoria and a tendency to dilate pupils are noted. The reaction of the pupils to light, convergence, and accommodation are absent. Weakness and spasticity in the muscles progress. Sensory and cerebellar disturbances are possible.
In the area of the cerebral pons, gliomas are most common; in the medulla oblongata - epindymomas, astrocytomas, oligodendrogliomas, and less commonly, glioblastomas and medulloblastomas. Most often these tumors occur in childhood. The initial signs are focal symptoms caused by damage to the cranial nerves and pathways. Pain in the occipital region appears early, and dizziness often occurs. Diplopia is often the first focal symptom. Early signs may indicate damage to half the trunk (see Alternating syndromes).
The diagnosis of a tumor is based on progressive damage to the brain stem and increased intracranial pressure, taking into account these additional research methods. Differential diagnosis is carried out with stroke, multiple sclerosis, encephalitis. Treatment of a brain stem tumor is surgical; if this is not possible, treatment is conservative. The prognosis for intrastem tumors, regardless of their histological structure, is usually unfavorable.
Bibliography: Human Anatomy, ed. M.R. Sapina, vol. 2, p. 348, M., 1986; Gusev E.I., Grechko V.E., Burd G.S. Nervous diseases, p. 186, M., 1988; Krol M.B. and Fedorova E.A. Basic neuropathological syndromes, M., 1966; Sandrigailo L.I. Anatomical and clinical atlas of neuropathology, vol. 125, 150, Minsk, 1988; Sinelnikov R.D. Atlas of Human Anatomy, vol. 3, p. 31, M., 1981.
Brain stem (on a sagittal section): 1 - medulla oblongata; 2 - bridge; 3 - cerebral peduncles; 4 -
Brain stem (on a sagittal section): 1 - medulla oblongata; 2 - bridge; 3 - cerebral peduncles; 4 - thalamus; 5 - pituitary gland; 6 — projection of the nuclei of the subtubercular region; 7 - corpus callosum; 8 - pineal body; 9 - tubercles of the quadrigeminal; 10 - cerebellum.
1. Small medical encyclopedia. — M.: Medical encyclopedia. 1991–96 2. First aid. - M.: Great Russian Encyclopedia. 1994 3. Encyclopedic Dictionary of Medical Terms. - M.: Soviet Encyclopedia. — 1982—1984
Source: https://dic.academic.ru/dic.nsf/enc_medicine/29975
You can sign up online or get the schedule of the nearest master classes at the link: https://qviz.matomba.ru/1c06710015fbab389df6
Diseases
Like any other organ, the brain can fail. The same applies to its trunk. Most problems become the consequences of injuries or other diseases, and sometimes simply manifestations of age. There are several diseases:
- Stroke;
- Tumor;
- Cysts;
- Chordomas;
- Ischemia;
- Malformation;
- Aneurysms;
- Epidermoids;
- Meningiomas.
Most of them appear extremely rarely. The bulk of reported cases of brainstem lesions are stroke and various tumors. They are the most dangerous and require the highest quality and fastest treatment. But why do they arise?
Causes
A particular disease can develop for many reasons. Those most at risk are those who already have serious brain diseases, lead an unhealthy lifestyle, or suffer from regular stress. But even healthy people can get problems with the brain stem. Violations occur for the following reasons:
- Diseases associated with blood vessels, as well as their damage;
- Traumatic brain injuries;
- Poor circulation;
- Nervous breakdowns, severe stressful situations;
- Extreme sports, as well as extreme sports in everyday life;
- Eating junk food or untreated water;
- Alcohol abuse, smoking;
- Congenital diseases associated with the brain stem.
When any diseases appear, they must be treated immediately. Lack of necessary medical intervention can lead to severe irreversible consequences or death.
Diffuse headaches and types of complications
Diffuse tumors of the brain stem can cause headaches. Diffuse headache at the very beginning of tumor formation rarely has a permanent nature and increasing effect.
Most often, the pain appears in attacks and lasts only a few minutes, in the intervals between which the patient feels completely healthy. If the increase in intracranial pressure is associated with stagnation of cerebrospinal fluid, then this occurs with brain tumors.
Unfortunately, malignant brainstem tumors affect areas of the brain. They are mainly of glial origin, from glial cells. These cells are responsible for creating normal working conditions for the nervous system. A diffuse brain tumor does not have a clear separation from the normal brain matter. The growth of these cells affects the important nerve centers of the trunk, which are responsible for breathing and heartbeat. By consulting a doctor in time, you can avoid the pathological development of the disease.
The brain stem is primarily responsible for vital activities such as heart rate, hyperventilation, temperature and appetite. A disorder of the brain stem structures can occur as a result of a traumatic brain injury, after a concussion, or trauma during childbirth. There are cases where there was no injury, but the person experienced intermittent loss of consciousness, seizures, or other signs of dysfunction.
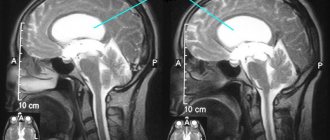
This diagnosis is made by neurologists or osteopaths, based on tests and studies, for example, you need to do an EEG, which should show irritation of the brain stem. The doctor must accurately determine the cause of the irritation, so an additional study of computed tomography and magnetic resonance imaging is prescribed.
Dysfunction means a disruption in the functioning of the brain stem, a tumor that compresses the brain stem structures; the result of dysfunction can be quite disastrous. To identify abnormalities in the functioning of the trunk in the early stages, you should see an osteopath immediately after the birth of a child or after a head injury. The doctor will determine whether there are any problems and offer individual treatment for you.
Dysfunction of the brain stem structures is curable, everything can be corrected in a fairly short time, you just need to restore full blood flow, as well as full mobility of the brain structures.
Brain stem metastases most often occur in early childhood, causing damage to nuclear formations. Alternating syndromes of motor and sensory disorders on the side of the tumor and the opposite side are often detected.
But on the side of the tumor the damage is more pronounced. A tumor of the brain stem can sometimes lead to disruption of the outflow of cerebrospinal fluid, resulting in hydrocephalus and hypertension. These diseases are late symptoms of a tumor of the trunk.
Benign tumors grow slowly, it can last for years and a person does not even suspect that he is developing a disease, sometimes the disease lasts up to 15 years. Malignant tumors, unfortunately, make up the majority of tumors and develop very quickly from several months to two years. Most often the tumor affects the pons of the brain, but sometimes it can choose another location.
R. Virchow believed that tumors on the brain stem cannot be operated on, but modern doctors believe that each case should be considered separately and sometimes a person has a chance. There are diffusely growing tumors, the majority of them, and there are nodular tumors containing cysts.
The following tumors of the trunk exist:
- stem inside;
- primary and secondary stem;
- pair of stem neoplasms.
Stroke
The most common disease affecting the brain stem is stroke. It is always associated with disturbances in the functioning of blood vessels. As the body ages or certain diseases occur, their walls become thinner and more inelastic, and may become covered with plaques or become completely clogged. Then a stroke occurs, which can lead to death.
There are two types of stroke: ischemic and hemorrhagic. The first is an infarction of the brain stem and is considered extremely dangerous due to blockage of blood vessels and subsequent oxygen starvation of nerve cells. The second manifests itself in the form of hemorrhage in the brain tissue. There is a risk of death in both cases.
Mechanism of action
In most cases, a hemorrhagic stroke occurs like this: first, a blockage of a vessel occurs, and then, under increased pressure, it bursts. When thinning, the vessels can immediately burst or become damaged without the formation of blood clots or any plaques. Immediately after the rupture, severe bleeding occurs in the brain, after which a hematoma appears, limiting the access of oxygen to the neurons. This becomes a failure, the consequence of which is a disruption of the functioning of all body systems.
With an ischemic stroke, severe damage to brain tissue also occurs, which greatly complicates the survival of the patient. After damage, the tissue gradually begins to die. Therefore, it is important to provide medical assistance to the victim as quickly as possible.
Causes
You can prevent a stroke if you try to exclude from your life all the moments that lead to this dangerous phenomenon. Doctors have been able to identify several main factors that increase the risk of cerebral infarction. Among them:
- Diabetes;
- Rheumatism;
- Hypertension;
- Atherosclerosis.
Everyone who is affected by at least one point needs to be as attentive to their health as possible and consult a doctor at the first alarming sensation.
Symptoms
A stroke is always sudden. A person can feel great throughout the day, and at one point hemorrhage occurs. Occasionally, shortly before a stroke, discomfort or pain may appear in the head. Symptoms indicating a cerebral hemorrhage are as follows:
- Dizziness;
- Increased sweating;
- Pale skin color;
- High body temperature;
- Pressure interruptions;
- Cardiopalmus;
- Breathing problems;
- Muscle paralysis.
The brain stem may be significantly damaged, making full recovery impossible. In this case, the development of severe complications associated with other diseases or characteristics of the body cannot be ruled out.
Treatment
Providing prompt assistance is the most important condition for preserving the life of the patient. But even she does not give any guarantees. Approximately 60% of victims die in the first days after a major stroke. In some cases, a person may die within two weeks. Only 20% of stroke survivors survive. If help is provided in the first hour after an attack, there is a chance of successful therapy. However, all consequences can be treated with great difficulty.
Transfer to a hospital is a prerequisite. It will not be possible to treat the victim at home; refusal to hospitalize will lead to death. Treatment involves constant monitoring by doctors and taking medications aimed at:
- Elimination of the formation of blood clots in blood vessels;
- Thinning of blood and existing blood clots;
- Reduced pressure;
- Normalization of cholesterol levels.
Additionally, physiotherapy is prescribed. In severe cases, emergency surgery may be performed. It is required to stop hemorrhage when conventional means do not have the desired effect.
Rehabilitation after successful treatment can take several years. Its duration depends on many factors and is individual in each individual case.
Tumor
The second most common tumor is the brain stem tumor. Some of them can be very dangerous, but most do not require any medical intervention. There are several types of tumors:
- Primary. Appear when brain tissue is damaged.
- Secondary. They are a consequence of other diseases.
- Deforming. They negatively affect the shape of the brain stem, deforming it. They may be located on the stem or some other parts.
- Diffuse. They merge with the brain matter, which creates serious difficulties in treatment. Cases of successful therapy are very rare.
- Parastem. They grow to the trunk, causing deformation.
- Diamond-shaped. Appear in the occipital part of the skull.
- Cerebellar. The cerebellum is affected along with the trunk.
- Exophytic. They form on the cerebellum, then reach the trunk.
Neoplasms develop gradually, increasing in size. Sometimes their growth may slow down or stop completely, eliminating the need for treatment. The reasons for their appearance are various injuries and complications after serious illnesses.
Symptoms
Identifying neoplasms that affect the brain stem is not so easy. If they are small in size, they may not cause any symptoms at all, which creates certain difficulties in diagnosis. By the time a tumor is discovered, as a rule, it has already grown to a large size.
Symptoms that may indicate the growth of a tumor are as follows:
- Headache;
- Dizziness;
- Coordination problems;
- Problems with vision or hearing;
- Disorientation in space;
- Tremor of the hands or head;
- Unstable mood.
If such symptoms occur, you should consult a doctor. The patient will be scheduled for an MRI, which will determine the presence of a tumor.
Treatment
The prognosis always depends on what kind of tumor the patient has. Its growth rate, size and exact location are of great importance. Benign neoplasms are easily removed surgically, for which an incision is made through which the tumor itself is excised. Malignant tumors cannot be removed using this method, so you will have to give preference to radiation therapy or other methods.
Methods for treating tumors:
- Surgical removal. Excision of the tumor using physical pressure with a knife; it requires making an incision. Suitable only for benign tumors.
- Radiation therapy. X-ray exposure to the tumor through all other structures of the head. Effectively slows down the growth of tumors.
- Stereotactic. A combination of several types of exposure is used, including radiation. It is characterized by the absence of any painful sensations for the patient.
If necessary, doctors can combine several treatment methods at once. This will increase the chances of successful tumor removal.
Drug treatment for tumor development is almost impossible. Cytostatics are the only drugs that can produce the desired effect. They are classified as chemotherapy drugs.
Midbrain
It is located between the diencephalon and the pons. The midbrain is the youngest stem section of the human brain.
Appearance
On the anterior surface of the midbrain, thick bundles of fibers are visible - the cerebral peduncles. At the top, the optic tracts go around them from the sides. The nerves of the 3rd pair of cranial nerves, the oculomotor ones, emerge between them.
The posterior surface of the midbrain is called the tegmentum . This is where the quadrigemina and its plate are located. In the upper colliculi, part of the visual information is processed, in the lower ones - part of the auditory information that does not need awareness. From under the inferior colliculi, a pair of trochlear nerves emerge from the posterior surface, which are the only pair of cranial nerves that generally emerge from the posterior surface of the brain.
conclusions
The brainstem is the most important part of the brain, as well as the entire body. The general condition of a person depends on his health. The slightest damage can cause serious consequences: loss of hearing or vision, inability to taste food, or maintain balance. The most dangerous is damage to the respiratory center, which leads to respiratory arrest. Prevention of brain stem diseases consists of maintaining a healthy lifestyle, avoiding head injuries and timely elimination of factors that can trigger the pathological process.