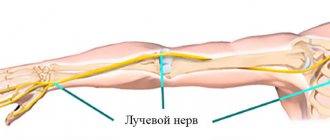
The scalene muscles are 3 large muscles that are located on both sides of the neck. With their upper edge they are attached to the lateral protrusions of the vertebrae (C2, C3, C4) of the cervical spine. With their lower edge they are attached to the 1st and 2nd ribs of the chest. Between the anterior and middle scalene muscles pass large blood vessels (subclavian artery and vein) and a bundle of nerve fibers (brachial nerve plexus).
Rice. 1. Anatomy of the neck - localization of the scalene muscles
Normally, muscles have elasticity, extensibility, are covered with “slippery” fascia and do not compress nerves and blood vessels. With pathological changes in the bone and muscle-tendon system, compression of these important organs of innervation and blood supply occurs, which causes the appearance of scalene muscle syndrome.
Depending on which muscle undergoes changes, a distinction is made between anterior scalene syndrome and posterior scalene syndrome. When nerves and blood vessels are compressed, neurovascular disorders are observed, accompanied by characteristic symptoms.
Symptoms of scalene muscle syndrome
Scalenus syndrome (SMS) may develop first as a myofascial pain syndrome. Due to overexertion or injury, the muscles spasm, structural changes occur in them, inflammation of the neck muscles develops, and trigger points (increased pain sensitivity) are formed. In this case, the main symptom of the pathology is pain. It radiates to the upper limb from the affected side, spreading from the shoulder joint to the tip of the phalanx of the ring or little finger. Often the soft tissues of the occipital part of the head and chest are involved in the pain process. The pain usually gets worse at night or when moving the head, upper limb, or taking a deep breath. The neck muscles hurt in different ways - from a mild nagging pain to a shooting, constant, burning pain.
Rice. 2. Map of the distribution of pain in scalene muscle syndrome
When a nerve bundle is compressed by a spasmodic muscle, the following manifestations are observed:
- a feeling of numbness, tingling, loss of sensitivity in the fourth and fifth fingers, as well as along the inner surface of the hand and forearm;
- swelling above the metacarpophalangeal joints of the II–V fingers and on the dorsum of the hand;
- stiffness of movements in the fingers, worsening in the morning.
When the great vessels are compressed, vascular disorders are observed:
- coldness of the extremity;
- cyanosis;
- numbness;
- swelling;
- disappearance of the pulse in the radial artery when raising the arm up and tilting the head to the affected side (Adson's test).
If lymphatic drainage is impaired, patients develop a swelling in the neck (Kovtunovich's pseudotumor) in the area of the supraclavicular fossa.
With prolonged disruption of innervation and blood supply, an imbalance of trophic processes occurs, which is accompanied by the following symptoms:
- damage to the nail plate – brittleness, unevenness;
- hair loss on the affected limb.
Long-term compression of nerve endings can lead to:
- hypertonicity of the neck muscles;
- heaviness, weakness in the hand;
- incomplete paralysis of a limb;
- atrophy of the muscles of the distal part of the arm.
As a rule, SLM is observed only on one side, much less often on both. The most dangerous complications occur when there is pain in the left neck.
Diagnostics
The set of diagnostic measures includes:
- clinical examination
- collection of complaints and clarification of neurological history
- functional radiography of the spine
- MRI
- electroneuromyography (study of bioelectric potentials of muscles, allowing to diagnose muscular-tonic syndrome of the lumbar region with symptoms of radiculopathy)
Magnetic resonance imaging is recognized as the most informative, safe and painless method of neuroimaging. It gives the most accurate assessment of the condition of the spine and spinal cord, allows you to identify protrusions and intervertebral hernias, determine their size and location.
Complications of scalene muscle syndrome
The most dangerous complications of SLM are:
- thrombosis of the subclavian artery;
- paresis and/or atrophy of the arm muscles;
- violation of the biomechanics of the neck and the whole body.
Large blood vessels pass between the anterior and middle scalene muscles - the subclavian artery and subclavian vein. Spinal vessels and arteries that supply blood to the brain depart from them. Therefore, thrombosis threatens to disrupt the blood supply to the spine, brain and body as a whole. Complaints that the neck is swollen on one side and there is a feeling of heaviness, pain, burning, and stiffness of movement are a signal for immediate hospitalization, surgical care and treatment.
A pinched nerve in the neck area leads to disruption of the innervation of the soft tissues of the hands, paresis and atrophy. If the consequences of atrophy and paralysis of the muscles of the limb are quite clear, then violations of the biomechanics of the neck need to be considered in more detail. When muscles are under prolonged tension, structural changes occur in the fibers - they compress, the muscles shorten and begin to “pull” the head forward. The curvature of the spinal column (lordosis) increases and a violation of the architectonics of the skeleton occurs. In this case, the muscles of the back of the neck and shoulder girdle are tense, and myofascial pain syndrome develops with the corresponding characteristics - trigger points and referred pain.
If the patient does not pay attention to the pain in the neck muscles and ignores treatment, then as a result of the action of compensatory mechanisms, curvature of the spinal column occurs in the lumbar and thoracic region. Changes in vector loads on the vertebrae cause deformation and protrusion of the intervertebral discs, the formation of hernias not only in the cervical region, but also in other areas of the spinal column.
Causes of this disease
Numbness and pain are caused by damage to the fibers that make up the nerves, as well as the vessels between the ribs and the collarbone. In addition, the cause may be excessive muscle density or pressure on the artery passing below the collarbone. All these factors can lead to impaired blood flow in the shoulder area and pathology of muscle innervation. If compression of the artery occurs, then a severe headache is added to the other symptoms of the disease.
Natzfinger syndrome in the vast majority of cases is one of the complications of osteochondrosis of the cervical spine.
Diagnostics of SLM
Due to the variety of manifestations of the syndrome, variability in severity, and lack of characteristic signs, its diagnosis presents some difficulties.
An important diagnostic sign is the condition of the skin, muscles, hair and nail plate. Feeling the neck reveals hypertonicity of the anterior scalene muscle and pain when pressed. A test for spasm is carried out - with maximum rotation in the direction of the lesion and strong pressing of the chin to the collarbone, the spasmed muscle is tensioned and trigger points are activated.
Another indicative test is the Adson test. On the affected side, the patient should raise the limb upward and tilt the head towards this shoulder. With SLM, the pulse in the arm will not be palpable. Specialists at the Manual Medicine Clinic “Galia Ignatieva MD” conduct physical examinations - examination, palpation, skin sensitivity tests of individual parts on the hand. During physical examinations, the doctor may measure temperature and pulse pressure in different arms and in different positions.
In addition to visual examination and physical examinations, the Manual Medicine Clinic “Galia Ignatieva MD” prescribes instrumental methods:
- electromyography (EMG), which allows you to assess the anatomical and functional characteristics of nerves and muscles;
- radiography - to identify anatomical abnormalities, the presence of an additional rib in the upper part of the chest;
- MRI – to visualize the condition of soft tissues, localization of compression of nerves and blood vessels;
- CT – for layer-by-layer visualization of changes in bone tissue;
- Ultrasound, Doppler mapping, angiography - to determine the presence of arterial stenosis and the speed of blood flow in them.
Specialists can also prescribe laboratory tests to identify inflammatory processes, assess blood sugar and hormone levels, which help in the differential diagnosis of SLM.
In the initial stage of SLM, instrumental diagnostic methods are uninformative and can give a false answer. Therefore, the most reliable method for diagnosing the syndrome is manual muscle testing. It allows you to conduct a comprehensive assessment of the condition and physiology, dynamics of movements, and identify the causes of disorders more quickly and informatively than other diagnostic methods.
Diagnosis and treatment of scalenus syndrome in
Medline-Service clinics employ experienced neurologists who will carry out all the necessary diagnostic measures to determine the causes of pain or other unpleasant symptoms that bother you. Our medical centers have advanced equipment to perform various instrumental studies, including ultrasound and radiography. Our doctors provide qualified assistance in the treatment of identified neurological pathologies, prescribing only the necessary procedures and medications.
To make an appointment with a neurologist at any of the clinics in the Medline-Service network, use the form on the website or call the contact number.
Treatment of scalene syndrome
After conducting research and establishing an accurate diagnosis, the doctor at the Manual Medicine Clinic “Galia Ignatieva MD” develops an individual SLM therapy plan. Treatment of scalene muscle syndrome is most often carried out using conservative methods:
- medicinal;
- physiotherapy;
- reflexology;
- exercise therapy;
- manual therapy.
Scalenus syndrome, the treatment of which requires symptomatic therapy, involves the use of the following groups of drugs:
- NSAIDs – medications eliminate inflammation and relieve pain;
- muscle relaxants – relax muscles, eliminate hypertonicity, spasm and, as a result, pain;
- opioid analgesics – to eliminate severe pain that is unresponsive to other types of painkillers;
- drugs for neuropathic pain and restoration of nerve structure.
After the severity of the symptoms of SLM has been reduced, physiotherapy methods can be added to the complex effect:
- shock wave therapy;
- magnetic therapy;
- laser therapy;
- DDT – diadynamic therapy;
- electrotherapy;
- vibration impact;
- myostimulation;
- phonophoresis;
- massage.
Physiotherapy eliminates inflammation, pain, activates blood circulation in soft tissues and normalizes trophic processes. In combination with medication, the effectiveness of treatment increases.
Exercise therapy is one of the important elements of the treatment program. Individually selected exercises allow you to:
- improve posture;
- eliminate muscle hypertonicity;
- correctly distribute the load;
- strengthen the muscle corset;
- restore range of motion in the neck and upper limbs.
Drug blockades are prescribed for the purpose of differential diagnosis and treatment of SLM, but due to the proximity of the nerve plexus, the procedure must be performed by a specialist with extensive experience.
Rice. 3. Manual treatment of SLM.
If a nerve in the neck is pinched, a vertebrologist can tell you what to do. The effectiveness of manual therapy at the Clinic of Manual Medicine “Galia Ignatieva MD” in relieving pain, restoring the anatomical and physiological characteristics of structures, eliminating muscle blocks and clamps has been proven by numerous clinical studies.
The specialist not only eliminates the signs and consequences of the pathology, but also acts on the root cause of SLM, since manual therapy has virtually no contraindications, it can be prescribed to patients with drug allergies, children and the elderly. Gentle manual techniques will restore mobility to the arm and neck, activate blood circulation, eliminate congestion, normalize metabolic processes and help remove metabolic products.
The use of surgical treatment is indicated only in exceptional cases - when there is a threat of arterial thrombosis, damage to nerve endings, the presence of an additional rib, etc. When the left neck hurts, the surgeon decides how to treat the anomaly.
Treatment
Conservative. As part of drug treatment, non-steroidal anti-inflammatory drugs, vasodilators, and vitamins are used. The choice of specific agents depends on the severity of pain and the nature of the dysfunction of the limb. Patients with this syndrome are also recommended physical therapy (electrophoresis, UHF and other procedures), massage, exercise therapy, and acupuncture.
Radical. The surgical method for treating this syndrome is called scalenotomy. During the operation, the doctor cuts through the muscle tissue. Due to this, optimal conditions are created for the functioning of nerves and blood vessels, and their injury is prevented.
Prevention of SLM
Specific methods for preventing SLM have not been developed. To prevent the occurrence of pathology, it is necessary to eliminate the causes of SLM:
- avoid hypothermia;
- eat rationally and control body weight;
- lead an active lifestyle - physical inactivity is one of the factors in the development of pathology;
- promptly identify and treat pathologies of the spinal column and musculotendinous system;
- avoid overstraining the muscles of the neck and shoulder girdle;
- train correctly;
- avoid prolonged fixed posture;
- the workplace must be ergonomic.
Anyone who has to spend a long time at a computer, desk, or operator console should know how to relieve neck muscle spasms with the help of special exercises. Examples of exercises can be found in specialized literature or shown by a specialist at the Manual Medicine Clinic “Galia Ignatieva MD”.
Manual therapy plays a great role in preventing relapse of SLM. A vertebrologist will show you how to relax your neck muscles. The patient can perform simple exercises and self-massage at home. In difficult cases, the help of a professional with extensive experience is necessary.
Tunnel syndromes as a cause of pain in the neck and arm
Reflex muscular-tonic syndromes are dominant among all manifestations of osteochondrosis of the cervical spine. Among reflex muscular-tonic syndromes at the cervical level, tunnel syndromes occupy a special place. Due to the fact that these syndromes manifest themselves with similar clinical symptoms, most authors of English-language scientific works use the term “the thoracic outlet syndrome” [2]. This term combines: – anterior scalene muscle syndrome (ASMS); – cervical rib syndrome; – costoclavicular syndrome; – pectoralis minor muscle syndrome (PMMS); – hyperabduction syndrome. With all of these syndromes, a combination of compression of the subclavian artery and brachial plexus is possible, which makes it possible to designate them as neurovascular syndromes. The most common are SPLM and SMGM [3]. The occurrence of SPLM, or scalenus syndrome, or Naffziger syndrome (named after the author who described it) is due to certain anatomical and topographical features. The anterior scalene muscle originates from the transverse processes of the III–VI cervical vertebrae, ending at the anterior edge of the first rib (Fig. 1). The subclavian artery and the lower trunk of the brachial plexus pass between the anterior scalene muscle and the first rib; the subclavian vein is located in front of the muscle. Tonic tension of the anterior scalene muscle causes the appearance of this syndrome. SPLM is often a symptom of cervical osteochondrosis, but this is often ignored by clinicians, because other, more striking clinical symptoms are the focus of medical attention. However, patients with subclinical forms of scalenus syndrome suffer longer, and the course of exacerbations of cervicalgia is more severe. Timely detection of scalenus syndrome has not only therapeutic and social significance, since it improves the patient’s quality of life, but also economic significance, since it reduces the number of days of disability and improves the quality of work performed by the patient. SPLM debuts predominantly (in more than 2/3 of patients) between the ages of 30 and 60 years, during the most active period. The main provoking factor in the development of SPLM is long-term static exposure of the head and upper limbs. When moving, the nerves are subjected to various loads (compression, stretching, bending), which are usually tolerated without pain or any functional impairment. As a result, in order to function adequately, the nerve must have freedom to glide through surrounding tissues and structures. Under physiological conditions, during limb movements, the nerve is capable of sliding in the longitudinal direction within a few millimeters, which provides nerve protection [4]. Even a slight decrease in the mobility of the nerve during limb movement can lead to microdamage and the formation of adhesions, further limiting the movement of the nerve. This creates a vicious circle, since adhesions, in turn, contribute to disruption of the outflow of blood and lymph, the development of swelling of the connective tissue sheaths of the nerve and compression of nerve fibers [5].
Clinically, SPLM is manifested by pain (in more than 85% of cases), which spreads along the inner surface of the shoulder, forearm and hand to the ring finger and little finger. Pain and sensory disorders increase with movements in the cervical spine. Sometimes pain radiates to the occipital region, especially when turning the head, sometimes to the chest, which requires the exclusion of angina. The pain intensifies during a deep breath, when turning the head in the healthy direction, at night. The pain increases significantly when moving the arm, especially when abducting it. Characterized by feelings of heaviness, weakness in the arm, and tension in the neck muscles. Vascular-trophic disorders gradually develop: coldness of the limb, cyanosis, numbness, swelling, brittle nails, decreased hair growth, weakening of the pulse, and sometimes the disappearance of the pulse when raising the arm and tilting the head in the same direction or with a maximum turn of the head in the opposite direction.
It should be noted that the neurovascular bundle can be subject to compression not only by the scalene muscle, but also by the accessory cervical rib. Cervical ribs can be 1- or 2-sided, have different sizes and degrees of clinical manifestations. The average incidence of cervical rib in the population is 6%. Cervical ribs are 3 times more common in the female population. There are 4 degrees of development of the cervical rib: 1) the cervical rib is limited by the transverse process of the 7th cervical vertebra; 2) the cervical rib extends beyond these limits, but does not reach the first rib; 3) the cervical rib is connected to the first rib through a ligament; 4) the formed cervical rib is connected to the sternum. SPLM clinically develops in every tenth owner of a cervical rib due to provoking factors. A vicious vicious circle develops, which is maintained by the tension of the anterior scalene muscle. In addition to the cervical rib, compression of the neurovascular bundle can be caused by a fracture or deformation of various origins of the clavicle and the first rib. According to B. Judovich and W. Bates, intraspinal tumors, C4–C7 radiculopathy, irritation of the phrenic nerve, myocardial infarction, etc. can lead to reflex tension of the anterior scalene muscle. The clinical picture of cervical rib syndrome is not much different from SPLM. The classic appearance of a patient with cervical rib syndrome is characterized by low shoulders and a seal-like appearance. Often in the supraclavicular region it is possible to palpate the cervical rib of one size or another. When pressing on the cervical rib or the large transverse process of the 7th cervical vertebra, pain and paresthesia in the arm arise or intensify. Less commonly, a systolic murmur can be heard during auscultation. The diagnosis of cervical rib syndrome is based on a typical clinical picture, a positive arm abduction test, as well as radiographic findings (elongated transverse processes of the 7th cervical vertebra or cervical rib).
An objective examination of scalenus syndrome in most cases reveals swelling in the supraclavicular fossa, which is explained by compression of the lymphatic vessels of this area due to changes in the anterior scalene muscle. The anterior scalene muscle itself is sharply tense. Percussion in the area of the projection of the scalene muscles provokes increased pain in the neck with possible irradiation to the arm. Neurological symptoms are manifested by a complex of sensory, motor and vegetotrophic disorders. The latter can manifest themselves in a range from swelling of the hand and mild acrocyanosis to severe trophic disorders.
Significant compression of the subclavian artery leads to a weakening of the pulse in the radial artery of the arm of the affected side. Patients in certain professions, such as plasterers, cannot work with their arms raised. During provocative tests: turning the head to the healthy side and taking deep breaths, the pulse may disappear completely, which is associated with additional tension in the scalene muscles, which are also auxiliary muscles of inhalation. When performing Dopplerography of neck vessels, it is also necessary to use a test with turning the head in the healthy direction, which significantly increases the diagnostic value of this method [6]. Objective diagnostic methods are especially necessary if SPLM manifests with symptoms of vertebrobasilar insufficiency with gradual development or acute, simulating the picture of compressive radiculopathy [7]. A possible deterioration in cerebral circulation is due to the fact that the vertebral artery, which is of cardinal importance in the blood supply to the brain, departs from the subclavian artery, which is subject to compression.
Early detection and adequate treatment of SPLM will help to avoid such an urgent and dangerous complication as thrombosis in the subclavio-vertebral-basilar system, which requires urgent surgical intervention. In case of SPLM, radiography is required to exclude cervical ribs or hypertrophied transverse processes, deformities of the clavicle, and the first rib. Electroneuromyography is considered a generally accepted method for diagnosing tunnel syndromes. However, at the initial stages of compression, the insufficient information content of this study can lead to erroneous conclusions [8]. When the brachial plexus nerves are compressed, the thick myelin fibers that carry information from proprioceptors are primarily damaged, which leads to functional muscle weakness. Detection of afferent paresis by manual muscle testing is currently considered as a more promising method for early diagnosis of SPLM [9]. Since there are more similarities than differences between the clinical manifestations of various tunnel syndromes in this area, angiographic methods of radiodiagnosis are sometimes of decisive importance. It is advisable to conduct a hagiographic study in a position with the arm abducted and the head turned to the healthy side.
Differential diagnosis Differential diagnosis of SPLM should be made with Paget-Schroetter syndrome, compression of the cervical spinal root, Raynaud's disease, obliterating endarteritis. Paget–Schroetter syndrome is an acute thrombosis of the proximal subclavian vein with possible extension to the axillary and brachial veins, resulting in obstruction of venous drainage in the arm. The core of the clinical picture of Paget–Schroetter syndrome is swelling and cyanosis of the arm on the affected side. The development of the disease is facilitated by a number of features of the subclavian vein, located surrounded by bone and tendon-muscular formations. Men (4:1) with well-developed muscles and those involved in sports or heavy physical labor are more often affected. As mentioned above, aggravation of clinical disorders when turning the head in the healthy direction is typical for scalenus syndrome. If pain increases when turning the head to the painful side, it is necessary to eliminate compression of the cervical spinal root.
SPLM differs from Raynaud's disease by affecting only one limb, trophic changes and lack of response to cold; from obliterating endarteritis of the upper extremities - increased pain when pulling the arm down while simultaneously turning the head to the healthy side. A pathognomonic sign of SPLM is a noticeable improvement in the condition with novocainization of the muscle. If the clinical picture is associated only with pathological muscle tension, then after its novocainization almost all symptoms should regress. In the case of “secondary” muscle damage, for example against the background of radicular syndrome, after novocainization the situation will not change significantly [10]. SMGM and Wright–Mendlovich hyperabduction syndrome are caused by muscular-tonic, trophic disorders in the pectoralis minor muscle, provoking compression of the neurovascular bundle passing under it (subclavian artery and vein, trunk of the brachial plexus). The pectoralis minor muscle originates from the II–IV ribs, rises diagonally upward and attaches to the coracoid process of the scapula (Fig. 2). The designation “hyperabduction syndrome” is legitimate in cases where the provoking factor of the tunnel syndrome is a strong, prolonged abduction of the arm (hyperabduction during anesthesia, during sleep with the head thrown back, frequently repeated jerking movements with abduction of the arm and raising it up).
The main clinical manifestations of VMS: pain in the area of this muscle, more at the level of the III-V ribs, possible irradiation to the neck, paresthesia in the anterior chest wall, weakness in the arm, more in the distal parts, autonomic disorders. The Wright test is of great diagnostic importance for SMGM - the hand is raised and placed behind the head. With such a movement, the neurovascular bundle is subjected to even greater compression under the pectoralis minor muscle. The test is considered positive if after 30 s a pain syndrome in the corresponding localization appears or intensifies, autonomic disorders increase (pallor and swelling of the fingers), and the pulse in the radial artery weakens [11].
During palpation examination (the patient's arm is retracted posteriorly and downward), the pectoralis minor muscle can be felt through the relaxed pectoralis major muscle during a deep inspiration. Muscle infiltration with procaine can be carried out both through the axillary region and through the pectoralis major muscle [12]. The difference in the clinical manifestations of SMGM and SPLM is that for lesions of the anterior scalene muscle, a violation of the venous outflow and, as a consequence, swelling of the hand and “stiffness” of the fingers are more typical. SMHM should be differentiated from Steinbrocker syndrome (shoulder-hand syndrome), which at its onset is characterized by excruciating pain in the shoulder and hand, reflex contracture in the shoulder joint with further formation of ankylosis.
Treatment For effective treatment of tunnel syndromes, it is necessary to understand the cause and mechanisms of compression and apply an integrated approach to therapy [13]. One of the important conditions for recovery or achieving long-term remission is the elimination of stereotypic movements that contribute to compression of the neurovascular bundle. Therapy for tunnel syndromes should begin with conservative measures, such as novocaine blockades (hydrocortisone can be administered additionally), physiotherapy (diadynamic currents, ultra-high frequency therapy, procaine electrophoresis), physical therapy, massage. The decision to initiate therapy and the choice of medications in most cases is dictated by the duration of pain, the severity of symptoms, and the degree of dysfunction caused by the pain. Traditionally, initial therapy for carpal tunnel syndrome includes: non-steroidal anti-inflammatory drugs (NSAIDs), B vitamins and vasodilators. One of the well-known and time-tested drugs is the combination drug Neurodiclovit, developed and produced by the Austrian company (in Russia the holder of the registration certificate is). It contains the NSAID diclofenac and vitamins B1, B6, B12.
Diclofenac has pronounced anti-inflammatory activity and powerful analgesic potential. The mechanism of action of diclofenac is associated with inhibition of the activity of the enzyme cyclooxygenase (COX), which is involved in the formation of prostaglandins from arachidonic acid and the activity of the enzyme lipoxygenase. In the early 90s of the last century, two isoforms of the COX enzyme were discovered - COX-1 and COX-2. Diclofenac inhibits both COX isoenzymes, due to which the analgesic effect of diclofenac occurs earlier than in the case of selective NSAIDs. Providing both central and peripheral antinociceptive effects, diclofenac provides effective suppression of pain of various etiologies. A pronounced analgesic effect, rapid regression of inflammatory processes, including inflammatory edema, have made this drug one of the most necessary for the treatment of compression-ischemic syndromes.
Thiamine (vitamin B1) as a result of phosphorylation is converted in the human body into cocarboxylase, which is actively involved in the processes of nerve excitation at synapses. Pyridoxine (vitamin B6) acts as a coenzyme for the most important enzymes acting in nerve tissues, ensures synaptic transmission, and normalizes the ratio of excitation and inhibition processes in the central nervous system. Cyanocobalamin (vitamin B12) has a beneficial effect on processes in the nervous system, is involved in the synthesis of the myelin sheath, helps reduce pain associated with damage to the peripheral nervous system, and is necessary for normal hematopoiesis and maturation of red blood cells, cell replication and growth. The advisability of combining NSAIDs with B vitamins is to potentiate the analgesic effect, reduce the risk of side effects of NSAID therapy, increase adherence to treatment, and also reduce the cost of a course of therapy when using Neurodiclovit compared to the separate use of NSAIDs + vitamin complexes. According to a number of independent studies [14], B vitamins potentiate the analgesic effect of NSAIDs and promote faster regression of pain than NSAID monotherapy.
Indications for the use of Neurodiclovit are: inflammatory and degenerative rheumatic diseases, many pain syndromes in neurological practice (in particular, acute back pain, tunnel syndromes), disorders of the musculoskeletal system, in addition, the drug is widely used in gynecology for dysmenorrhea, adnexitis; for inflammatory diseases of the ENT organs. The drug Neurodiclovit is enteric granules of diclofenac with delayed release and separate granules of vitamins B1, B6, B12 with immediate release. Neurodiclovit is prescribed orally, during meals, with the recommendation not to chew and drink plenty of liquid. For adults, Neurodiclovit is prescribed 1 capsule - at the beginning of treatment 3 times / day, as a maintenance dose - 1-2 times / day. The average duration of therapy is 7–14 days.
Vasodilators are an addition to the complex therapy of tunnel syndromes; the most commonly used are xanthinol nicotinate, drotaverine, and pentoxifylline (vasonite). It is advisable to continue therapy with neurotropic B vitamins (for example, Neuromultivit) to increase the effectiveness of therapy and reduce the risk of disease chronicity and relapses. Indications for the surgical treatment of tunnel syndromes: the failure of the complex of treatment measures, the presence of gross impairments of motor and sensory functions, the rapid increase in symptoms with the development of contractures, the development of secondary complications (in particular, thrombosis) [15, 16].
A radical method of treating tunnel syndromes is dissection of the tissues compressing the nerve, removal, if necessary, of the cervical rib and the creation of optimal conditions for the nerve trunk and blood vessels, preventing their injury. In case of SPLM, the preference of neurosurgeons is currently given to resection of the anterior scalene muscle over as much of its extent as possible. This reduces the risk of relapse of the disease due to fibrotic changes in the specified area, and also eliminates the focus of pathological irritation. The prognosis for tunnel neuropathies depends on timely diagnosis and initiation of therapy. In the case of the development of irreversible metabolic processes in the neurovascular bundle, as well as atrophy and contractures in the innervated muscles, the prognosis is unfavorable. Timely use of NSAIDs and B vitamins allows in some cases to prevent or at least delay the onset of irreversible changes.
References 1. Guez M., Hildingsson C., Nilsson M. et al. The prevalence of neck pain // ActavOrthop.Scand. 2002. Vol. 73. P. 455–459. 2. McKenzie K., Lin G., Tamir S. Thoracic outlet syndrome. Part I: a clinical review // J Am Chiropr Assoc. 2004. Vol. 41(l). R. 17–24. 3. Popelyansky Ya.Yu. Orthopedic neurology. Guide for doctors. M., 2008. pp. 19–24. 4. Kipervas I.P. Tunnel syndromes. 3rd ed., revised. and additional M.: Newdiamed, 2010. 520 p. 5. Luchetti R., Amadio P. Carpal Tunnel Syndrome. Springer-Verlag, Berlin, Heidelberg. NY, 2007. R. 70. 6. Skoromets A.A., Skoromets A.P., Skoromets T.A. Topical diagnosis of diseases of the nervous system. M.: Politekhnika, 2007. 400 p. 7. Rasstrigin S.N. New approaches to the clinical assessment, diagnosis and treatment of anterior scalene syndrome: Abstract of thesis. diss. ...cand. honey. Sci. M., 2005. pp. 3–6. 8. Gekht B.M. Electromyography in the diagnosis of neuromuscular diseases. Taganrog: TRTU Publishing House, 1997. 370 p. 9. Novak CB Thoracic outlet syndrome // Clin Plast Surg. 2003. Vol. 30. R.175–188. 10. Kalmin O.V. Morphological factors of biomechanical reliability of peripheral nerves: Author's abstract. diss. ... doc. honey. Sci. Saransk, 1998. 38 p. 11. Golubev V.PI. Merkulova D.M., Orlova O.R., Danilov A.B. Tunnel syndromes of the hand // BC. 2009. T. 17. pp. 7–12. 12. Moskvitin A.V. Tunnel syndromes of the scalene and pectoralis minor muscles (frequency, diagnosis, treatment): Abstract. diss. ...cand. honey. Sci. Irkutsk, 2011. pp. 2–4. 13. Solovyova E.Yu. Therapy of back pain // Neurology, neuropsychiatry, psychosomatics. 2012. No. 2. 14. Graham RG, Hudson DA, Solomons M., Singer M. A prospective study to assess the outcome of steroid injections and wrist splinting for the treatment of carpal tunnel syndrome // Plast Reconstr Surg. 2004. Vol. 113(2). R. 550-556. 15. Jarvik JG, Comstock BA, Kliot M et al. Surgery versus non-surgical therapy for carpal tunnel syndrome: a randomized parallel-group trial // Lancet. 2009. Vol. 374 (9695). R. 1074–1081.
Physical therapy
Conservative treatment should be the first treatment strategy for SVA as it is effective in reducing symptoms and improving function. Conservative treatment includes physical therapy, which focuses primarily on patient education, pain control, increasing range of motion, improving nerve gliding, and strengthening muscles.
First stage
The goal of the initial phase is to reduce the patient's symptoms. This can be achieved through patient education, which explains what SVA and poor posture are. In addition, the patient is explained his prognosis and the importance of following the doctor's recommendations. People who sleep with their arms up need to be aware of their posture to avoid waking up during the night. These patients should sleep on their unaffected side or in a supine position, possibly with the sleeves secured. If the patient has a "release phenomenon", then Cyriax release may be used. This method completely unloads the neurovascular structures in the area of the superior aperture before bedtime.
Kyriax Release Maneuver
- Elbows bent 90°.
- Towels create a passive lift of the shoulder girdle.
- Support the spine and head in a neutral position.
- The position is maintained until peripheral symptoms appear.
The patient's breathing technique must be assessed because the scalene and other accessory muscles often compensate for the primary respiratory muscles during inspiration. Encouraging diaphragmatic breathing will reduce the stress on already overworked or tense muscles and possibly reduce symptoms.
Working with a spatula
This is important to ensure normal scapular muscle recruitment and control in the resting position. Once this has been achieved, the next step is to improve scapular control during movement and under load. Training begins with lower ranges of abduction and gradually progresses further into the ranges of abduction and flexion until the muscles are retrained to operate within higher amplitudes.
Control of the position of the humeral head
It is also important to control the position of the humeral head. The most common abnormality is the anterior position of the humeral head. A useful strategy to promote stabilization and centralization of the humeral head is a moderate-intensity isometric contraction of the rotator cuff muscles by applying resistance to the humeral head.
This can be integrated into movement patterns later in treatment. First in exercises with slow controlled concentric/eccentric movement, then in isolated exercises to strengthen the muscles.
Recruitment and control of the serratus anterior muscle
The external rotation and abduction strategies described above are often sufficient to recruit and control the serratus anterior muscle without the risk of overactivating the pectoralis minor muscle.
Second phase
Once the patient has reduced their symptoms, they can move on to this stage of treatment. The goal of this step is to directly target the tissues that are creating the structural restrictions. How this should be done is one of the most debated topics. Here are some options that are discussed in the literature.
- Massage.
- Strengthening the levator scapulae, sternocleidomastoid, and upper trapezius muscles (this group of muscles “opens” the superior opening, elevating the shoulder girdle and increasing the costoclavicular space).
- Stretches the pectoral muscles, lower trapezius, and scalene muscles (these muscles “close” the superior opening).
- Exercises to correct posture.
- Relaxation of shortened muscles.
- Aerobic exercise in your daily home workout program. Exercises for the shoulder girdle and restore range of motion and increase space for neurovascular structures. Lift your shoulders back and forth, flex your upper thoracic spine, and move your shoulders forward and down. Then straighten your back and repeat the exercise 5-10 times.
- Amplitude of movement of the cervical spine. Standing with your back to the wall (touching the back of your head), lower your chin to your chest (5-10 repetitions). The effectiveness of this exercise can be increased by pressing your hands down on your head.
- Activation of the scalene muscles is the most important point. The exercises are performed in isometric mode for 5 seconds. Anterior scalene muscle - press your forehead into your palm; middle scalene muscle - press on your palm with the side of your head; posterior scalene muscle - press the back of your head into your palm.
- Stretching exercises.
Other events
- Mobilization of the shoulder girdle: cervicothoracic, sternoclavicular, acromioclavicular and costotransverse joints.
- Mobilization of the glenohumeral joint at the end of the amplitude of shoulder elevation with support of the elbow in extension.
- Taping: Some patients with severe symptoms respond favorably to taping and orthoses that elevate or retract the shoulder girdle.
Manual therapy and mobilization of the first rib
Mobilization of the first rib should be done with caution and only after careful evaluation because this may cause irritation and painful symptoms in some patients.
- Posterior glide of the humeral head with flexion of the arm. The patient lies on his back. The mobilizing hand touches the proximal humerus, avoiding the coracoid process. The force is directed posteriorly (thumb direction).
- Anterior sliding of the humeral head with hand grip. The patient is positioned in a prone position. The mobilizing hand touches the proximal humerus, avoiding the acromion. The force is directed anteromedial.
- Inferior sliding of the humeral head. The patient is positioned in a prone position. The stabilizing arm holds the humerus proximally (distal to the acromion). The mobilizing hand touches the axillary edge of the scapula. Mobilize the scapula in a craniomedial direction along the rib cage.
- Mobilization of the first rib. The patient is sitting. A thin belt is placed over the first rib. Pull the strap towards the opposite thigh. The neck is in a position of retraction, contralateral lateral flexion and ipsilateral rotation. Ipsilateral head rotation increases stretching of the scalene muscles. Contralateral rotation enhances mobilization of the first rib.
Epidemiology/Etiology
SVA affects approximately 8% of the population and is 3 to 4 times more common in women than men aged 20 to 50 years. Women have less developed muscles, a greater tendency to droop the shoulder girdle due to extra breast tissue, and have a narrowed superior opening. These factors change the angle between the scalene muscles and therefore cause a higher prevalence in women. The average age of people suffering from SVA is 30-40 years. This condition is rarely seen in children. Almost all cases of SVA (95-98%) involve the brachial plexus; in remaining cases (2-5%), vascular structures such as the subclavian artery and vein are affected.
There are several factors that can cause SVA. Cervical ribs are present in approximately 0.5-0.6% of the population, 50-80% of which are bilateral, and 10-20% cause symptoms; the ratio of women to men is 2:1. Cervical ribs and associated fibromuscular structures are responsible for most cases of SVA. Fibromuscular lesions are a more common cause of SVA than rib abnormalities.
Congenital factors
- Cervical ribs.
- Elongated transverse process of the vertebra.
- Muscle abnormalities.
- Fibromuscular formations (transverse costal, costocostal).
- Abnormalities of attachment of the scalene muscles.
- Exostosis of the first rib.
- Scoliosis.
- High scapula position.
- The location of the subclavian artery or vein in relation to the anterior scalene muscle.
Acquired fortunes
- Postural changes.
- Dropping of the shoulder girdle.
- Heavy mammary glands.
- Injury.
- Clavicle fracture.
- Rib fracture.
- Whiplash, neck injury during hyperextension.
- Repetitive injuries (most often caused by sitting at a keyboard for long hours).
Muscular causes
- Hypertrophy of the scalene muscles.
- Decreased tone of the trapezius, levator scapulae and rhomboid muscles.
- Shortening of the scalenes, trapezius, levator scapulae, and pectoral muscles.