The internal popliteal nerve (median sciatic nerve) is the proximal part of the tibial nerve, which, in turn, is a continuation of the sciatic nerve, the largest nerve in the human body.
The sciatic nerve innervates the muscles of the dorsum of the thigh, that is, it promotes flexion of the knee and ends in two large branches in the popliteal fossa - tibial and peroneal. The proximal part of the tibial nerve performs the following functions:
- due to the presence of collateral branches, it promotes motor innervation and sensitivity of the muscles of the back of the leg, that is, extension of the ankle and flexion of the toes;
- The medial plantar and lateral plantar branches , which terminate the median popliteal nerve, provide innervation to the muscles of the soles, due to which flexion and lateral displacement of the toes are carried out.
Types of nerve damage
Damage to the median popliteal nerve is not so common due to its location, and usually occurs in pre- or retirement age (up to 60 years) in persons suffering from inflammatory processes localized in the lumbosacral region, in persons with a chronic form of recurrent sciatica, Athletes often suffer from it.
The etiology of the development of pathology in the popliteal part of the tibial nerve is primarily associated with the following factors:
- injury;
- inflammation;
- toxic effects, deformation, compression, etc.
There are three types of median nerve injury:
- neuralgia;
- neuritis;
- neuropathy.
More details about each type of damage:
- A condition in which compression (damage) of the internal popliteal nerve occurs is called neuralgia . It can be caused by both inflammatory and other processes occurring in the soft tissues adjacent to the nerve. The patient feels a burning or tingling pain, which is localized in the ankle area, spreads to the toes and intensifies when walking.
- The inflammatory process occurring in the peripheral nerves, a group of which includes the median popliteal nerve, is called neuritis . Neuritis differs from neuralgia in that inflammation affects the nerve along with its membrane, while with neuralgia, damage to the area where the nerve endings pass occurs due to irritation from many factors. Neuritis occurs with intense pain, impaired nerve function and changes in sensitivity.
- Another type of damage to the median popliteal nerve is also common - neuropathy . This condition can be of traumatic, compression, or dysmetabolic origin. The development of pathology leads to disruption of the muscle functions of the lower leg, which manifests itself in painful flexion of the foot and toes. In addition to pain, vegetative-trophic changes in the foot are observed. The risk group includes athletes and those who are forced to squat for a long time.
All processes differ from each other in etiology, course, treatment methods, and consequences.
Diagnostics
Diagnosing peripheral neuropathy can sometimes be difficult due to the variability of symptoms. A complete neurological examination is often required, including: the patient's symptoms, occupation, social habits, the presence of any toxins, the presence of chronic alcoholism, the possibility of HIV or other infectious disease, and a history of relatives with neuropathy, performing tests that can identify the cause of the neuropathy, and conducting examinations to determine the degree and type of nerve damage.
General examination tests and tests may reveal the presence of nerve damage due to systemic disease. Blood tests can diagnose diabetes, vitamin deficiencies, liver or kidney failure, other metabolic disorders, and signs of abnormal immune system activity. Examination of the cerebrospinal fluid, which circulates in the brain and spinal cord, can reveal abnormal antibodies associated with neuropathy. More highly specialized tests can detect blood diseases or cardiovascular diseases, connective tissue diseases, or malignancies. Muscle strength tests showing signs of muscle twitching or fasciculations may indicate motor neuron damage. Assessing the patient's ability to perceive vibration, soft touch, body position (proprioception), temperature and pain sensitivity helps determine damage to sensory fibers of both large and small sensory fibers. Based on the results of a neurological examination, physical examination, and a detailed medical history, additional tests and examinations may be prescribed to clarify the diagnosis.
Computed tomography is an atraumatic, painless study that makes it possible to visualize organs, bone and soft tissue. A CT scan can reveal bone or vascular changes, brain tumors, cysts, herniated discs, encephalitis, spinal stenosis (narrowing of the spinal canal), and other disorders.
Magnetic resonance imaging (NMR or MRI ) can examine the condition of the muscle and its size, reveal the replacement of muscle tissue with fatty tissue, and determine whether there has been a compressive effect on the nerve fiber. MRI machines create a strong magnetic field around the body. Radio waves pass through the body and cause resonance, which can be detected at various angles within the body. The computer processes this resonance effect and converts it into a three-dimensional image.
Electromyography (EMG ) involves inserting a thin needle into a muscle to measure the electrical activity of the muscle at rest and during contraction. EMG tests can help differentiate between damage to the muscle itself and to the nerve fibers. Nerve conduction speed can accurately determine the extent of damage in large nerve fibers, clearly indicating whether symptoms are related to myelin sheath or axon degeneration. During this study, electrical stimulation of the fiber is performed, in response to which a response impulse appears in the nerve. An electrode placed further along the nerve measures the speed of impulse transmission along the axon. Slow transmission rates and impulse blocking typically indicate damage to the myelin sheath, while decreased impulse levels are a sign of axonal degeneration.
A nerve biopsy involves removing and examining a sample of nerve tissue, most often in the lower leg. Although this test can provide valuable information about the extent of nerve damage, it is an invasive procedure that is difficult to perform and can cause nerve damage and signs of neuropathy. In most cases, this procedure is not indicated for diagnosis and may independently cause neuropathic side effects.
Skin biopsy is a test in which a small piece of skin is removed and the endings of nerve fibers are examined. This diagnostic method has advantages over EMG and nerve biopsy when it is necessary to diagnose damage in smaller sensory fibers. Additionally, unlike a conventional nerve biopsy, a skin biopsy is less invasive, has fewer side effects, and is easier to perform.
What provokes the destructive process
There can be many reasons for damage to the median popliteal nerve; in addition to the common ones - trauma, inflammation, compression, the following can be distinguished:
- slow blood circulation due to varicose veins;
- valgus flatfoot;
- rheumatoid arthritis;
- prolonged sitting cross-legged;
- wearing excessively tight shoes;
- changes in the musculoskeletal system
- reflex muscular-tonic disorders due to spinal curvature (osteochondrosis, scoliosis, spondyloarthrosis);
- surgical interventions resulting in incorrect positioning of the leg;
- diseases resulting in proliferation of connective tissue (gout, polymyositis);
- metabolic disorders (diabetes mellitus, obesity);
- intoxication (alcohol, drugs);
- local tumor processes.
general description
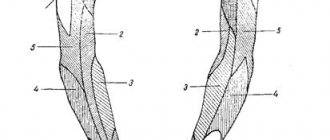
Damage to the external (lateral) popliteal nerve (G57.3) is a neuropathy of the peroneal nerve, manifested by muscle weakness and decreased sensitivity of the lateral part of the leg.
| Peroneal nerve 1 - sciatic nerve, 2 - peroneal nerve, 3 - musculocutaneous nerve, 4 - deep peroneal nerve, 5 - neck of the fibula, 6 - biceps femoris muscle, 7 - peroneus longus muscle |
More common between the ages of 40–60 years. The nature of the lesion is unilateral.
In most cases, the cause of the lesion is a lower leg injury. Less commonly, the lateral popliteal nerve is damaged by injury to the knee/ankle joint, compression of the leg during sleep, tight casting of the lower leg, or prolonged squatting.
Clinical picture
The initial stage of the pathological process is characterized by severe, persistent and long-term (from several months to several years) pain in the popliteal fossa and in the lower leg. Cramps in the calf muscles are possible, which are accompanied by a syndrome of moderate intensity.
Pain can occur both at rest and when walking. Over time, paresthesia of the lower leg and foot develops. Afterwards, paretic processes occur in the foot and muscle wasting of the affected limb.
The damaged side is characterized by a decrease in the Achilles reflex and an increase in the knee reflex; upon visual examination, swelling of the tissue in the popliteal fossa is detected. On palpation, the patient complains of dense formations in the muscles, at the point of their attachment to the tendons; the patient can feel the compaction during self-examination.
On the inside of the foot, the arterial pulse decreases, the patient is not able to fully straighten the leg due to the destruction of the muscles that are innervated by the damaged nerve. Due to the absence of the Achilles reflex, there is a change in sensitivity in the area of the sole and back of the leg.
Among the complications of phlebectomy in works devoted to this problem, damage to the trunks and branches of peripheral nerves is almost always mentioned. As a rule, the literature indicates a short-term, lasting up to 1-6 months, loss of sensitivity in small areas of the skin of the operated limb. This can be caused by nerve damage both during miniphlebectomy and during removal of the trunks of the main saphenous veins. Most often, such situations develop during interventions in the basin of the great saphenous vein and a reflection of the desire of phlebologists to avoid neurological complications is, for example, the recommendation to use a short stripping of the line. This allows us to exclude injury to the branches of the medial saphenous nerve, which are close to the trunk of the great saphenous vein on the leg. Particular attention should also be paid to miniphlebectomy, since the instruments are manipulated almost blindly. It can be stated that during interventions on the great saphenous vein and its tributaries, algorithms for preventing neurological complications have been developed and, in general, can be considered effective - the use of modern tactical approaches (short stripping) and gentle techniques practically eliminate the possibility of developing neurological complications.
As for the risk of damage to peripheral nerves during phlebectomy in the basin of the small saphenous vein, this aspect of the problem is very rarely discussed. This is largely due to the significantly smaller number of interventions performed in this venous system. Nevertheless, due to anatomical features, it is during interventions on the small saphenous vein that the risk of neurological complications is especially high. This is due to the close proximity of the tibial nerve and the ostial part of the small saphenous vein in the popliteal fossa, as well as the sural nerve with the trunk vs parva
in the lower half of the tibia and its origins at the lateral malleolus.
We would like to present to the attention of our colleagues a case of damage to nerve trunks that occurred during surgery on the small saphenous vein.
Patient K.,
63 years old, in August 2011 she applied to the Central Institute of Traumatology and Orthopedics named after. N.I. Priorov with a referral from a neurologist to conduct an ultrasound examination of the peripheral nerves of the lower extremities. She complained of decreased skin sensitivity on the dorsum and plantar surface of her right foot, and a feeling of weakness when moving the toes of her right foot. This symptomatology developed after the patient underwent phlebectomy on the right lower limb for varicose veins on October 16, 2010 in one of the Moscow hospitals. Feelings of numbness and weakness appeared the day after the operation, which she reported to the attending physician. According to the patient, numbness was regarded by the doctor as a common situation after phlebectomy, which does not require additional examination, since neurological disorders resolve on their own within several months after such an operation. Weakness when moving the toes was also regarded as a normal course of the postoperative period, when many patients, experiencing pain, involuntarily spare the operated leg. Before discharge from the hospital, an ultrasound examination of the surgical area was performed; no pathology was detected. The patient was discharged for outpatient follow-up treatment with the usual recommendations (compression bandage, phlebotonics). Subsequently, these complaints did not tend to disappear. Since January 2011, the patient was observed by a neurologist, the symptoms began to worsen—weakness in the toes increased, and sensory disturbances persisted. In July 2011, electroneuromyography was performed; when stimulating the nerves on the right lower limb, signs of gross damage to the tibial and sural nerves on the right were found. The patient was recommended to undergo neurosonography to clarify the nature of the lesion and was referred to the Central Institute of Traumatology and Orthopedics.
Local status: the right lower limb is not swollen, the skin is warm, normal color, no varicose veins; There are typical scars after phlebectomy in the basin of the great saphenous vein (along the inguinal fold, on the lower leg) and the small saphenous vein (in the popliteal fossa and behind the lateral malleolus).
The patient underwent an ultrasound examination of the venous system and peripheral nerves of the limb.
During angioscanning: deep veins - without pathological changes; the great saphenous vein has been removed along its entire length, there is no stump; the small saphenous vein is ligated in the popliteal fossa, there is no stump, it is passable distally, its diameter along the leg is 3-4 mm, it is stable.
Neurosonography of the right tibial nerve: the anatomical integrity of the nerve is preserved throughout its entire length. At the level of the popliteal fossa, the nerve is unevenly thickened to 0.77×0.78 cm; along 6.7 cm, the nerve is deformed, differentiation into fibers is preserved, and thickening of individual fibers within the nerve is noted. The contours are uneven and clear. At the level of the upper corner of the popliteal fossa (1.5 cm proximal to the level of the postoperative scar), hyperechoic linear inclusions (suture material?) are noted in the structure of the nerve in the anterior sections (see figure, a).
Figure 1. Sonograms of patient K. a - the tibial nerve was located (small arrows) in the popliteal fossa. 1 - hyperechoic inclusion in the nerve structure (suture material?). Distal to the level of the postoperative scar in the popliteal fossa, the nerve is club-shaped thickened, an oval area of hypoechoic structure measuring 1.16×0.50 cm is visualized (see figure, b)
Figure 1. Sonograms of patient K. b - intra-stem neuroma of the tibial nerve in the popliteal fossa (highlighted with markers, dimensions of the formation 1.16×0.50 cm). - intramedullary neuroma. The nerve in the lower leg is structurally unchanged.
Neurosonography of the right sural nerve: the nerve is formed at the level of the upper third of the leg, cross-sectional size 0.11×0.07 cm, accompanies the small saphenous vein. Differentiation into fibers is preserved. At the level of the outer malleolus (postoperative scar area), the nerve is pulled to the suture (see figure, c),
Figure 1. Sonograms of patient K. in - the sural nerve was located behind the lateral malleolus. Small arrows indicate its area, deformed and pulled up to the postoperative scar. its anatomical integrity is preserved, but the course of the nerve is disrupted, the nerve is thickened to 0.18×0.2 cm, differentiation into fibers is not expressed.
Thus, clinical symptoms and ultrasound data suggested iatrogenic damage to peripheral nerve trunks that occurred during phlebectomy.
Indeed, clinical practice shows that minor neurological disorders after phlebectomy are not uncommon, but in the vast majority of cases they consist of a local decrease in skin sensitivity and disappear on their own after several months after the operation. In this situation, we are talking about a serious complication that requires neurosurgical intervention and highlights a number of mistakes made by phlebologist surgeons. At first glance, it may seem that nerve damage is caused only by obvious technical errors. When searching for the small saphenous vein in the popliteal fossa, the surgeons manipulated quite roughly, which caused damage to the tibial nerve over a significant extent with the development of a neuroma. Moreover, echo-positive inclusions were found in the structure of the nerve, which could be suture material. Considering that upon completion of the operation to ligate the small saphenous vein, 2-3 nylon sutures are placed on the fascia dissected in this zone in the horizontal direction along the axis of the limb, the appearance of suture material in the structure of the nerve becomes understandable - it was stitched precisely during this stage interventions. As for the sural nerve, its entry into the suture when closing the access behind the lateral malleolus is apparently due to the capture of too large a volume of tissue when applying a Donati-type suture used in the patient.
However, crude surgical technique is not the only, and not even the main, thing that led to the development of such a complication. The leading reason, in our opinion, was the incorrect choice of treatment tactics, based on overdiagnosis during preoperative ultrasound angioscanning. It is clear that intervention on the small saphenous vein was not necessary at all. The following arguments and conclusions support this statement. Phlebectomy was performed in the basin of both main saphenous veins. Obviously, the preoperative ultrasound report described the incompetence of both the great and small saphenous veins - it is unlikely that without these data surgeons would have started the operation from the territory of the small saphenous vein. The main volume of intervention occurred in the system of the great saphenous vein, as evidenced by the marks from minifebectomy on the medial surface of the leg. Only two incisions were made in the territory of the small saphenous vein - in the popliteal fossa and behind the lateral malleolus. Thus, there were no varicose veins in the system of the small saphenous vein, and the nature of the intervention performed on the small saphenous vein - ligation of the initial and terminal sections without removal of the trunk and intervention on the tributaries - indicates that the small saphenous vein and its system at the time of the operation were intact. The surgeons probably decided not to remove the trunk of the small saphenous vein because, having exposed it, they found that the caliber indicated no changes in the vessel. By the way, the search for an unchanged small saphenous vein is often difficult and not always successful. This is precisely what can explain the injury to the tibial nerve in the popliteal fossa - surgeons have long and actively tried to detect the “incompetent”, according to ultrasound angioscanning data, the small saphenous vein. It is likely that these searches were unsuccessful, as a result of which the decision was made to make an incision at the lateral malleolus, cross the small saphenous vein and pass the probe proximally, using it to locate the ostial part of the vessel. Be that as it may, the surgeons were convinced that the small saphenous vein was not changed, and decided to simply ligate its initial and terminal sections. Of course, the course of events could have been somewhat different, but it seems to us that the version presented and described is very close to what actually happened.
This example shows how important a careful assessment of the clinical situation is when planning surgical intervention in patients with varicose veins. Simultaneous damage to both venous systems is a very rare situation. Having received the results of an ultrasound examination about the presence of reflux in the great and small saphenous veins and having made sure during examination of the limb that there were no varicose veins in the basin of the small saphenous vein, the doctors should have ordered a repeat study and, what would be optimal, be present during it in order to independently assess the situation. We are confident that having seen a vein trunk of insignificant caliber (3-5 mm) and the absence of dilated tributaries, the operating surgeon would hardly have decided to perform an intervention on such a vessel and thus would have avoided unjustified manipulations that resulted in the development of a serious complication.
Conflict of interest:
the authors declare no conflict of interest
Establishing diagnosis
Diagnosis is carried out taking into account clinical and neurological data. In order to correctly diagnose a lesion, the following sequence of methods is used:
- Survey (about the state, activity of uncomfortable sensations).
- Palpation to identify compactions.
- Examination to identify the muscle-trunk symptom of Lasègue . When walking, patients tend to limp on the side that is damaged due to its imaginary shortening. This symptom in most patients can even be detected several years after the first symptoms appear.
- Due to similar manifestations of vertebrogenic pathology, doctors practice examining the spine and knee joint using radiography .
- Additionally, the nature of the damage is revealed using ultrasound diagnostics, MRI, and electromyography .
Median nerve neuropathy
Affected nerve endings lead to disruption of the transmission of impulses from the central nervous system to muscle tissue and organs. Because of this, sensitivity, motor, and trophic functions change. Neuropathy may manifest as:
- numbness of the limb;
- tingling, burning;
- spasmodic pain when moving;
- weakness, low muscle tone, atrophy.
The patient is unable to bend the foot down or stand on his toes, the affected limb loses sensitivity, the foot takes on the appearance of a “paw” with claws, and the gait changes.
Treatment of neuropathy is aimed primarily at eliminating the consequences: in case of wounds and injuries, plastic surgery is performed, the nerve is sutured, tumor formations are also surgically removed, and at the same time pain is relieved.
In general, therapy for median nerve neuropathy is long-term, so the course of treatment is complex and includes:
- medications (B vitamins, metabolic drugs, NSAIDs);
- physiotherapeutic (electrophoresis, magnetic therapy, massage, physical therapy, etc.);
Popliteal neuralgia
The most common symptom of median nerve neuralgia is burning or tingling pain in the ankle, foot, or toes. Discomfort increases with movement and decreases when at rest.
A group of methods is used as treatment:
- medicinal method : injections of corticosteroids and other painkillers are prescribed;
- compression : bandages are applied to the foot; it is recommended to wear special insoles that help reduce pressure on the nerve.
- Surgical intervention occurs in rare cases.
Treatment
There are no treatments for hereditary peripheral neuropathies. However, there are treatments for many other forms. First, the cause of the disease is treated and symptomatic treatment is carried out. Peripheral nerves have the ability to regenerate if the nerve cell itself is preserved. Symptoms can be managed, and addressing the causes of certain forms of neuropathy can often prevent recurrence of damage.
In general, healthy lifestyle choices—such as maintaining an optimal weight, eliminating toxins from entering the body, eating well with adequate vitamins, and limiting or eliminating alcohol intake—can reduce the physical and emotional effects of peripheral neuropathy. Active and passive exercise can reduce cramps, improve muscle elasticity and strength, and prevent muscle atrophy in paralyzed limbs. Various diets may improve gastrointestinal symptoms. Prompt treatment for injuries can help prevent permanent damage. Quitting smoking is especially important because smoking spasms the blood vessels that carry nutrients to peripheral nerves and can worsen neuropathy symptoms. Good nursing skills, such as careful care, of diabetic feet and wounds are essential because these patients have decreased pain sensitivity. Good care can relieve symptoms and improve quality of life and stimulate nerve regeneration.
Systemic diseases often require more complex treatment. Strict control of blood glucose levels has been shown in studies to reduce neuropathic symptoms and help patients with diabetic neuropathy avoid further nerve damage. Inflammatory and autoimmune diseases that lead to neuropathy can be treated in several ways. Immunosuppressants such as prednisone, cyclosporine, or imuran can be very effective. Plasmapheresis, a procedure that clears the blood of immune cells and antibodies, can reduce inflammation or suppress the activity of the immune system. Large doses of immunoglobulins, which function as antibodies, can also suppress abnormal immune system activity. But neuropathic pain is difficult to treat. Moderate pain can sometimes be relieved with analgesics. Some medications (used to treat other conditions) have proven helpful for many patients suffering from severe forms of chronic neuropathic pain. They include Mexilitine, a drug designed to treat irregular heart rhythms (but sometimes causes significant side effects); some antiepileptic drugs, including gabapentin, phenytoin, and carbamazepine; and some types of antidepressants, including tricyclics such as amitriptyline. Injecting a local anesthetic such as lidocaine or using patches containing lidocaine may relieve severe pain. In the most severe cases of pain, the nerves can be surgically destroyed; however, the results are sometimes temporary and the procedure can lead to complications.
Orthotics can help reduce pain and reduce the impact of physical disability. Various arm or leg orthoses can compensate for muscle weakness or relieve nerve compression. Orthopedic shoes can improve gait disturbances and help prevent foot injuries in people with decreased pain perception.
Surgery can often provide immediate relief for mononeuropathies caused by nerve entrapment or compression. Removal of a herniated disc causes decompression of the root. Removing tumors also reduces the impact of tumor tissue on the nerves. Additionally, nerve decompression can be achieved through ligament and tendon release.
Neuritis damage
With median nerve neuritis, muscle paralysis occurs, the ability to bend and turn the foot, and move the toes is lost, and the Achilles reflex does not function.
The patient feels difficulty walking, stands on his heel, cannot stand on his toes, and feels extremely intense pain.
Treatment of neuritis is carried out in different ways, conservative ones include:
- acupuncture;
- reflexology;
- stimulation of nerve and muscle tissue (physiotherapeutic method, neurostimulation, massage, physical therapy);
- taking vitamins B (Milgamma), C, E;
- taking antiviral, anti-inflammatory medications (Voltaren, Ketoprofen);
- use of homeopathic methods.
Operative methods include:
- neurolysis;
- suturing of the nerve trunk.
Treatment of damage to the internal (median) popliteal nerve
Treatment is prescribed only after confirmation of the diagnosis by a medical specialist. Symptomatic (decongestants, analgesics, vitamins) and physiotherapy are carried out. Massage, novocaine and hydrocortisone blockades are indicated.
Essential drugs
There are contraindications. Specialist consultation is required.
- Voltaren (non-steroidal anti-inflammatory drug). Dosage regimen: IM at a dose of 75 mg (contents of 1 ampoule) 1 time/day.
- Ketoprofen (non-steroidal anti-inflammatory drug). Dosage regimen: IM - 100 mg 1-2 times a day; after pain relief, it is prescribed orally in a daily dose of 300 mg in 2-3 doses, a maintenance dose of 150-200 mg/day.
- Diacarb (diuretic). Dosage regimen: 0.25 g orally 2 times a day (morning, afternoon) for 5-7 days.
- Milgamma (B complex of vitamins). Dosage regimen: therapy begins with 2 ml intramuscularly 1 time per day for 5-10 days. Maintenance therapy - 2 ml IM two or three times a week.
Consequences and complications
The consequences of injuries to the median nerve can be very serious: all three types (neuritis, neuropathy, neuralgia) are classified as common and severe, which in advanced cases lead to complete or partial disability.
With insufficient treatment, or in the absence of it, the sick person is forced to change his profession and lifestyle.
There are frequent cases of disability due to atrophy of the muscle tissue innervated by the affected nerve. Unfortunately, at present, a significant number of errors are often made both in the diagnosis and in the treatment of this pathology.
Preventive actions
In order to prevent damage to the internal popliteal nerve in time, injury and hypothermia should be avoided.
It is worth keeping in mind that the risk group includes older people, athletes, as well as those who suffer from obesity (metabolism problems), are addicted to alcohol and drugs, and lead a sedentary lifestyle. You can avoid defeat if you follow some rules:
- do not stay in a “squatting” position for a long time (this is especially worth remembering for those who like to pick berries in the forest);
- when sitting, do not cross your legs;
- lead an active lifestyle;
- review your diet (adhere to a healthy diet);
- avoid infectious diseases (scarlet fever, HIV, tuberculosis, herpes, measles);
It is important to promptly seek qualified help at the first signs of a lesion. After all, most diseases can be treated conservatively in the early stages of detection.
Causes of peroneal nerve neuropathy
The causes of neuropathy can be judged by the names that different authors have used to call peroneal nerve tunnel syndrome: sleep paralysis, fashion model syndrome, tulip digger's paralysis. Let us list them in detail.
- Direct injury (fracture of the head of the fibula, dislocation of the knee joint) or traumatic injury when the foot is twisted, accompanied by tension on the peroneal nerve and its damage.
- Compression paralysis is compression of the nerve in the head of the fibula caused by external factors.
- by this mechanism, the nerve can be compressed during sleep or in an unconscious state (sleep paralysis) if the outer surface of the lower leg comes into contact with the hard frame of the bed;
- when sitting cross-legged for a long time - a position in which podium stars often pose in front of the camera (mannequin syndrome);
- compression of the nerve with a plaster cast or splint in the upper third of the leg;
- activities that require prolonged periods of kneeling or squatting (tulip bulb digger paralysis);
- compression of the nerve when wearing high narrow shoes (leather boots);
- a sharp decrease in body weight with loss of the protective subcutaneous fat layer can lead to compression of the peroneal nerve even with slight external compression
- Anterior tibial syndrome or anterior tibial muscle compartment syndrome. In this condition, caused by a fracture of the leg bones, arterial thrombosis or muscle strain due to prolonged walking, severe swelling of the soft tissues of the leg occurs and almost inevitable compression of the peroneal nerve
- Nerve damage during surgery (surgery for a popliteal artery aneurysm or a woman staying in a gynecological chair for a long time during surgery)
- Space-occupying formations in the knee area (Baker's cyst, knee ganglion)
- Genetic predisposition (familial cases of peroneal tunnel neuropathy have been described in the medical literature)
- Concomitant somatic diseases predisposing to the development of tunnel neuropathies (diabetes mellitus, polyarteritis nodosa)
Separately, it is necessary to highlight damage to the fibers of the peroneal nerve as part of the spinal roots or the sciatic nerve, when the traumatic factor acts at a higher level, and the clinical manifestations correspond to damage to the nerve in the upper third of the leg. Such manifestations may occur when:
- herniated intervertebral disc L4-L5 with compression of the fifth lumbar root, which is called vertebrogenic pseudoneuropathy of the peroneal nerve
- compression of the fifth lumbar root during childbirth due to compression by the fetal head
- non-compliance with the rules for intramuscular injections in the gluteal region and injury to the sciatic nerve
- traumatization of the fibers of the peroneal nerve, which are part of the sciatic nerve, when reducing a dislocated hip joint or performing total hip replacement
Any damage to the neural structures that form the peroneal nerve leads to an increased risk of injury at the level of the lower leg, even with minor external influences.