Our clinic is engaged in examination, treatment and rehabilitation measures for pinched, inflammation and injuries of the nerves of the legs (sciatic, tibial, peroneal and their branches). You will need to be examined by a neurologist. if any studies have been previously performed, be sure to take their results for consultation, incl. the x-rays themselves . If the studies have not been performed, we will do everything necessary in our clinic or with our colleagues in other clinics.
- What are the causes of damage to the tibial and peroneal nerves?
- Symptoms of Tibial and Peroneal Nerve Suffering
- Diagnosis of neuropathies of the tibial and peroneal nerves
- Treatment of damage to the tibial and peroneal nerves at the Echinacea clinic
- When is surgery necessary?
How the treatment will be structured:
- Let's establish the location and cause of nerve damage. We perform electromyography of the peroneal, tibial and other leg nerves and ultrasound of the nerves. The potential benefit of non-surgical treatment or strict indications for surgery (risk of complete nerve loss) can be determined using needle myography.
- We will find out and discuss with you the possibility of non-surgical treatment and the prospects for restoring nerve function. Medicines can be used here, incl. administration of anti-inflammatory and absorbable drugs directly to the point of compression or damage to the nerve. For the rehabilitation treatment of the sciatic, tibial and peroneal nerves, magnetic stimulation of the nerves of the legs is very effective: improvement is noticeable immediately or several days after the procedure.
- If the chances of restoring the peroneal or tibial nerve without surgery are low, we recommend surgical treatment . We perform most of the operations on an outpatient basis. You will be able to go home on the day of surgery. The budget for surgery without hospitalization is significantly less. If hospitalization is required, we will refer you to a trusted specialist. After surgical treatment, we will offer a course of rehabilitation treatment.
What are the causes of damage to the tibial and peroneal nerves?
The tibial and peroneal nerves pass through narrow canals formed by bones, ligaments, tendons and muscles. Nerve tissue is very delicate and vulnerable. Often we detect nerve suffering even with slight narrowing or deformation of the nerve canal. Narrowing or deformation of the tibial and peroneal nerve canals occurs:
- In case of injury (bone fracture, bruise, hemorrhage, sprain or wound); Often, when injured, the nerve is pulled into scarred tissue or compressed by a bone fragment; nerve injury can also be represented by a nerve bruise, partial or complete interruption.
- If there is compression in an uncomfortable position (a tucked or compressed leg while wearing uncomfortable shoes, position, unconsciousness or intoxication, under anesthesia);
- With thickening and deformation of the knee and ankle joints and ligaments , with chronic injury and overload of the joints, often associated with the type of activity (sports, walking, forced posture, vibration, weight). Very often, such changes are facilitated by diseases and deformities of the spine. These types of neuropathy are called tunnel syndromes of the ulnar, radial and median nerves;
- For foot deformities due to flat feet (tarsal tunnel syndrome, meralgia) .
The function of nerves is to conduct electrical impulses from the brain to muscles and organs, and to the brain from sensory receptors in the body. Any damage to the nerve leads to disruption of the conduction of excitation along the nerve, which means disconnection of the affected part of the body from the brain.
Therefore, if the tibial and peroneal nerves suffer, the following are possible:
- Decreased strength and weight loss of leg muscles, twisting of the foot when walking and even fractures;
- Decreased sensitivity (numbness)
- Pain along the nerve or in the foot, fingers.
Symptoms
Clinical signs of peroneal nerve neuropathy depend on the location of its lesion (along the route) and the severity of its occurrence.
Thus, with an acute injury (for example, a fracture of the fibula with displacement of fragments and damage to nerve fibers), all symptoms arise simultaneously, although the first days may not come to the fore due to pain and immobility of the limb. If the peroneal nerve is gradually injured (when squatting, wearing uncomfortable shoes, and other similar situations), symptoms will appear gradually, over some time.
All symptoms of peroneal nerve neuropathy can be divided into motor and sensory. Their combination depends on the level of the lesion (for which the anatomical information was presented above). Let's consider the signs of neuropathy of the peroneal nerve depending on the level of damage:
- with high compression of the nerve (as part of the fibers of the sciatic nerve, in the region of the popliteal fossa, that is, before the nerve divides into superficial and deep branches), the following occur:
- disturbances in the sensitivity of the anterolateral surface of the leg, the dorsum of the foot. This may be the lack of sensation of touch, the inability to distinguish between painful irritation and just touch, heat and cold;
- pain on the lateral surface of the leg and foot, intensifying when squatting;
- impaired extension of the foot and its toes, up to the complete absence of such movements;
- weakness or inability to abduct the outer edge of the foot (lift it);
- inability to stand on your heels and walk like them;
- when walking, the patient is forced to raise his leg high so as not to catch his toes; when lowering the foot, first the toes fall to the surface, and then the entire sole; when walking, the leg bends excessively at the knee and hip joints. This gait is called “cock” (“horse”, peroneal, steppage) by analogy with the gait of the bird and animal of the same name;
- the foot takes on the appearance of a “horse”: it hangs down and seems to be turned inward with the toes bent;
- with some experience of neuropathy of the peroneal nerve, muscle loss (atrophy) develops along the anterolateral surface of the leg (assessed in comparison with a healthy limb);
- when the external cutaneous nerve of the leg is compressed, exceptionally sensitive changes (decreased sensitivity) occur along the outer surface of the leg. This may not be very noticeable, because the external cutaneous nerve of the leg connects to a branch of the tibial nerve (the fibers of the latter take on the role of innervation);
- Damage to the superficial peroneal nerve has the following symptoms:
- pain with a hint of burning in the lower part of the lateral surface of the leg, on the back of the foot and the first four toes;
- decreased sensitivity in these same areas;
- weakness in abduction and elevation of the outer edge of the foot;
- damage to the deep branch of the peroneal nerve is accompanied by:
- weakness of extension of the foot and its toes;
- slight drop of the foot;
- impaired sensitivity on the back of the foot between the first and second toes;
- with a long-term existence of the process - atrophy of the small muscles of the dorsum of the foot, which becomes noticeable in comparison with a healthy foot (the bones protrude more clearly, the interdigital spaces sink).
It turns out that the level of damage to the peroneal nerve clearly determines certain symptoms. In some cases, there may be a selective violation of the extension of the foot and its toes, in others there may be elevation of its outer edge, and sometimes only sensory disorders.
Diagnosis of neuropathies of the tibial and peroneal nerves
The most successful treatment for neuropathy is treatment directly at the point of nerve damage. For successful treatment, your treating doctor will find out:
- At what exact point is the nerve damaged (compressed); this helps us provide targeted treatment;
- What exactly led to the nerve suffering (trauma, scar, compression);
- The degree of nerve suffering (complete or partial damage, the presence of a recovery process, the presence of complete death of the nerve, etc.).
Often, to establish the cause of nerve pain, a detailed neurological examination is sufficient , during which the strength of the muscles controlled by the nerve, the possibility of certain movements, sensitivity, the presence of pain points and seals along the nerve are assessed. Auxiliary diagnostic methods are electroneuromyography, radiography and computed tomography.
Electroneuromyography allows you to assess the speed and volume of impulses along the nerve, detect the location of damage/compression, and determine the prognosis for recovery. Electromyography helps us evaluate the effect of certain types of treatment and choose the most suitable ones. The Echinacea clinic uses a modern computer electroneuromyograph.
X-ray and computed tomography of the joints and feet will provide complete information about the deformation of the joints and bone canals of the nerves, the causes and points of compression of the nerve.
Stimulation electromyography of the lower extremities
A small anatomical educational program
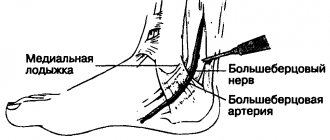
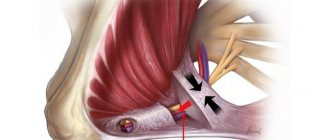
The peroneal nerve is part of the sacral plexus. The nerve fibers go as part of the sciatic nerve and are separated from it into a separate common peroneal nerve at the level of or slightly above the popliteal fossa. Here, the common trunk of the peroneal nerve is directed to the outer side of the popliteal fossa, spiraling around the head of the fibula. In this place it lies superficially, covered only by fascia and skin, which creates the preconditions for compression of the nerve from the outside. The peroneal nerve then splits into superficial and deep branches. Somewhat higher than the division of the nerve, another branch departs - the external cutaneous nerve of the leg, which in the region of the lower third of the leg connects with the branch of the tibial nerve, forming the sural nerve. The sural nerve innervates the posterolateral part of the lower third of the leg, the heel, and the outer edge of the foot.
The superficial and deep branches of the peroneal nerve are so named due to their course relative to the thickness of the lower leg muscles. The superficial peroneal nerve provides innervation to the muscles that provide elevation of the outer edge of the foot, as if rotating the foot, and also forms the sensitivity of the dorsum of the foot. The deep peroneal nerve innervates the muscles that extend the foot and toes, and provides sensations of touch and pain in the first interdigital space. Compression of one or another branch, accordingly, is accompanied by impaired abduction of the foot outward, the inability to straighten the toes and foot, and impaired sensitivity in various parts of the foot. According to the course of the nerve fibers, the places of its division and the origin of the external cutaneous nerve of the leg, the symptoms of compression or damage will be slightly different. Sometimes knowledge of the characteristics of the innervation of individual muscles and skin areas by the peroneal nerve helps to establish the level of compression of the nerve before using additional research methods.
Treatment of damage to the tibial and peroneal nerves at the Echinacea clinic
When it is clear where, how and why nerve compression occurs, local treatment in the form of physiotherapy, therapeutic blockades, massage, and manual therapy becomes much more effective. Therefore, treatment in our clinic begins with finding out the cause and location of nerve damage .
The main goals of treatment for nerve compression:
- Remove nerve compression. To do this, we use powerful resorption therapy: we use enzymes that resolve and soften scar tissue, bone and cartilage growths (Karipazim enzyme, etc.), massage, and injecting medications directly into the site of nerve compression. Sometimes, to release the nerve, manual therapy and massage of the areas of compression of the tibial and peroneal nerves (spine, leg joints, etc.) are sufficient.
- Accelerate healing and restoration of the nerve. To do this, we use modern medications that help restore the nerve that has been released from compression in the scars.
- Restore muscle function and volume. Special exercises, electrical stimulation of muscles, and physiotherapy are used here. The rehabilitator will tell you in detail and show you how to perform rehabilitation procedures at home.
Various Treatment Methods
Pharmacotherapy
To restore the myelin sheath of the nerve, alpha-lipoic acid preparations (thioctacid, berlition, espalipon) are prescribed. Among other neurometabolic drugs, a combination of B vitamins (milgamma, combilipen, neuromultivit) is traditionally used or a combination drug is prescribed - Keltican, registered in Russia as a dietary supplement.
The use of non-steroidal anti-inflammatory drugs for peroneal nerve neuropathy is ineffective, since the cause of persistent pain is not so much inflammation of the soft tissues as damage to the nerve itself. This pain is neuropathic and requires the prescription of drugs from other groups: anticonvulsants (gabapentin, Lyrica, Finlepsin); antidepressants (amitriptyline, Cymbalta, Ixel).
Peroneal nerve block
If pharmacotherapy is insufficiently effective, a nerve block in the area of the head of the fibula can be used. A local anesthetic (lidocaine solution) is administered in combination with a hormonal drug (diprospan, dexamethasone). The clinical effect occurs after a single procedure. If necessary, a series of blockades can be performed while pain persists.
Surgical intervention
Surgical intervention is performed:
- in the presence of a formation in the soft tissues of the knee area, causing compression of the peroneal nerve (Baker's cyst, ganglion of the knee joint)
- in case of injury that leads to damage to the nerve trunk
- with anterior muscle compartment syndrome of the lower leg
Orthopedic correction
To prevent ankle sprains, a special orthosis is used to fix the foot. All factors that can lead to compression of the nerve in the upper third of the leg are excluded (narrow high shoes, prolonged squatting or cross-legged)
When is surgery necessary?
In case of nerve injury, it is very important to decide in a timely manner whether conservative or surgical treatment is advisable. The answer to this question can be obtained after conducting needle myography, which will answer the question of what is the degree of damage to the nerve and whether it has a tendency to recover. If during this study it turns out that at least partially the nerve is preserved, we carry out active conservative treatment, after which we must repeat the study to make sure that the treatment had an effect . If, during needle myography, it turns out that the nerve is completely damaged and its restoration is impossible, we resort to the help of a neurosurgeon who suturing the nerve or releasing it from significantly narrowed canals. Then we perform the entire range of restoration procedures.