Diagnosing a cerebral aneurysm is critical to saving the patient's life. Yes, you can sometimes live with this disease for years, but the situation will worsen, the aneurysm will grow, threatening to rupture at any time. Therefore, you need to be examined regularly and thoroughly, after which the doctors will decide on an operation, the price of which in Moscow for a cerebral aneurysm will be from 300 thousand rubles. Correct and timely tactics will save the patient’s health and life. Unfortunately, little attention is still paid to this serious disease, so most often it is discovered completely by accident.
What is a cerebral aneurysm
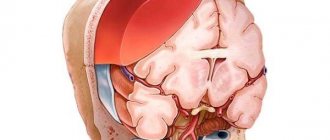
An aneurysm, most commonly a saccular aneurysm, is a spherical or similar formation on an artery in the brain. An aneurysm, as I have already noted, can be saccular and fusiform. An aneurysm consists of three parts - the neck, body and bottom or apex.
Unlike a normal vascular wall, the apex of the aneurysm is not three-layered, but single-layered and is most vulnerable to rupture, especially since a shock flow of blood rushes into this place. Most often, the aneurysm is located in the anterior sections of the circle of Willis - in descending order - an aneurysm of the anterior communicating artery of the PSA, then an aneurysm of the internal carotid artery of the ICA, and an aneurysm of the middle cerebral artery. Less common are aneurysms of the vertebrobasilar region - aneurysms of the fork of the main artery of the OA, the mouth of the posterior inferior cerebellar artery of the PICA. Aneurysms of the pericallosal artery and other distal parts of the anterior cerebral and middle cerebral arteries are also quite rare.
Causes of plaques in the carotid arteries
The formation of cholesterol plaques in the carotid arteries is one of the forms of systemic atherosclerosis, rarely occurring in isolation.
As a rule, atherosclerosis of the brachiocephalic arteries (brachio - shoulder, cephalis - head (Greek)), which includes the carotid arteries, is combined with atherosclerosis of the aorta, coronary arteries, and arteries of the lower extremities. Atherosclerosis
- a chronic disease of arteries of the elastic and muscular-elastic type, arising as a result of lipid metabolism disorders and accompanied by the deposition of cholesterol and some fractions of lipoproteins in the intima of blood vessels. Deposits form in the form of atheromatous plaques. The subsequent proliferation of connective tissue in them (sclerosis), and calcification of the vessel wall lead to deformation and narrowing of the lumen up to obliteration (blockage). It is impossible to name one single reason leading to atherosclerotic restructuring of the artery wall and the formation of atherosclerotic plaques.
Most researchers agree with the fact that atherosclerosis is based on a violation of fat metabolism (more precisely, cholesterol esters) at the level of genetic predisposition. Familial hypercholesterolemia (FH) is a known disease. This is a disease caused by a decrease in the rate of removal of low-density lipoprotein (LDL) from the bloodstream due to mutations in the specific LDL receptor gene. Familial hypercholesterolemia is the most common genetic disease due to a single gene mutation (monogenic disease). The modern medical scientific community, based on numerous studies, considers risk factors to be the main triggers for the progression of atherosclerosis (an increase in the size and number of plaques).
Cerebral aneurysm photo
I present to your attention a photo of 2 aneurysms - the main artery and the bifurcation of the middle cerebral artery, which we encountered in our clinic over the past 2 weeks.
Saccular aneurysm of the bifurcation of the basilar artery
Saccular aneurysm of the bifurcation of the left middle cerebral artery. The aneurysm and branches of M2 are outlined with a ballpoint pen.
The aneurysm of the bifurcation of the basilar artery had to be transferred to another health facility for endovascular exclusion (filling with coils), and the MCA aneurysm was operated on in our clinic.
What are the advantages of endovascular surgery?
Endovascular operations began to be practiced recently, but quickly gained great popularity among doctors and patients due to many advantages:
- The main advantage of endovascular interventions is the low risk of complications, due to the fact that during such an operation no incisions are made and general anesthesia is not used. One small puncture under local anesthesia is enough.
- After the procedure, patients recover very quickly. You can return to your normal life after a maximum of 4 weeks (often within a few days), while after open surgery on large vessels - after 3 months.
- Hospitalization time is reduced. Typically, it is enough for the patient to spend only 1–3 nights in the hospital. During and after the procedure, the patient experiences much less pain and discomfort than after classic open interventions through an incision.
- Due to the very low risk of complications, endovascular surgery is often the best choice for elderly patients and people with severe concomitant diseases.
- Excellent cosmetic result. There are practically no traces left at the puncture site.
Endovascular surgery helps to safely cope with various pathologies, even in severe cases.
Take care of yourself, make an appointment with a doctor now
Message sent!
expect a call, we will contact you shortly
Cerebral aneurysm causes of occurrence
The final genesis of the arterial aneurysm is not clear. Some argue that this is a congenital phenomenon - an undeveloped, blindly ending short vessel. Others say that this is an acquired condition - a protrusion in a weak spot of the hemangion - the structural unit of the vessel, between the circular areas of smooth muscle. As a result of the impact of the shock wave, this protrusion gradually grows. The formation of de-novo aneurysms confirms the presence of new aneurysms during control angiography in already operated patients. There is also an autoimmune inflammatory theory of the occurrence of arterial aneurysms, which is being actively developed at the University of Helsinki with the participation of Professor J. Hernisniemi. Thus, he believes that eventually a drug will be developed that can treat and prevent aneurysmal disease (he considers himself the last of the Mohicans - i.e. "aneurysmal" surgeons).
Microsurgical treatment of asymptomatic aneurysms
Until recently, asymptomatic aneurysms were detected extremely rarely. In recent years, the widespread availability and availability of noninvasive neuroimaging techniques has led to a significant increase in the number of patients with incidentally discovered aneurysms. Over the past 10 years, the institute has operated on about 400 patients with asymptomatic aneurysms. The results of surgical treatment in this category of patients should be considered satisfactory. Taking into account these data, as well as the extremely high probability of an unfavorable outcome in case of rupture of an aneurysm, it can be argued that unruptured asymptomatic aneurysms in most cases require surgery. It should be noted that the patient must be fully informed about the nature of the disease, the upcoming operation and possible complications.
Cerebral aneurysm - symptoms
Most often, an aneurysm debuts with rupture - the most serious, often fatal complication. Hemorrhage can be subarachnoid, parenchymal and ventricular , and there are also all kinds of combinations of this trinity.
Among the atypical manifestations is pseudotumor ; with a gigantic size of the aneurysm, it can behave like a tumor and compress the brain and nerves, causing focal neurological symptoms.
A migraine-like course is manifested by hemicranialgia.
Pseudoradicular simulates radiculitis - pain in the legs, which is caused by blood flowing into the terminal cistern of the spinal cord.
Meningitis-like - in this case, patients with suspected bacterial meningitis can be admitted to an infectious diseases hospital, where SAH and suspected aneurysm rupture are diagnosed only with a lumbar puncture.
Psychotic - the name speaks for itself.
Patient reviews
Mikhail Lvovich Vysotsky: I was observed and treated by Dr. Alexander Aronov at Medis for several years, for all sorts of little health issues, and at some point I was diagnosed with an aneurysm on an MRI. After consultations and “weighing” all the pros and cons, I went for an operation with Dr. Moisei Aronov, he is an endovascular surgeon, probably one of the best in Moscow. The neurosurgeon dealt with the situation and now I can continue to live in peace. Otherwise, it’s like walking around with a bomb in you. If someone has such a situation, you need to boldly go for surgery, but with one “but”, you need to go to the best specialist.
Anna Larina: Thanks to the timely operation performed by Dr. Krylov, my mother’s life was saved. The organization of everything was perfectly done.
Treatment methods for cerebral aneurysm
Surgical
Aneurysm can only be treated surgically - by direct intervention, disconnection by clipping, wrapping with various materials (rarely) or by the endovascular method. Only milliary aneurysms can be observed in patients without risk factors for rupture. Aneurysms without previous hemorrhages are also subject to surgical treatment. It is easier to prevent a rupture than to treat its fatal consequences - vasospasm and clipping the aneurysm in the acute period.
Intraoperative photo of a clipped left middle cerebral artery aneurysm.
CT angiography the next day after surgery. Aneurysm is turned off. The M2 segments of the left MCA are contrasted.
The red circle marks the intervention area where 2 clips are installed. There are signs of vasospasm.
In the area of surgery on a native CT scan of the brain along the Sylvian fissure there is a small amount of blood - impregnated surgicell.
On a CT scan in bone mode, the clip is clearly visible.
Treatment of aneurysms in pediatric patients
Cerebral aneurysms in children are rare and can be combined with various connective tissue pathologies (Marfan’s syndrome, Ehlers-Danlos’s syndrome) and various developmental anomalies of the circle of Willis. In children, aneurysms with complex anatomical characteristics are detected three times more often than in adults. Pseudotumorous and ischemic types of course in “children’s” aneurysms occur several times more often than in adults. Incidentally discovered aneurysms in children are rare. The principles of surgical treatment of aneurysms in children are generally the same as in adults. It should be noted that the compensatory capabilities of a child in the event of the development of any complications are greater than those of adults, so children can more easily tolerate the switching off of the arteries carrying the aneurysm. In this regard, deconstructive operations can be considered as the method of choice in cases of complex aneurysms when it is impossible to switch off the aneurysm while maintaining arterial patency.
Cerebral aneurysm - consequences after surgery
The consequences of the operation, as well as the natural course of the disease, very often is cerebral vasospasm, which leads to unsatisfactory treatment results - death or severe neurological deficit in the form of paresis and paralysis, aphasia, mental disorders (which is typical for aneurysms of the anterior communicating artery). Meningitis may be a complication of the operation itself, which is associated with the presence of blood - a rich nutrient medium in the subarachnoid space, in the basal cisterns, cerebral ischemia, and a rather long operation time.
Thus, the treatment of arterial aneurysms is a very urgent and difficult problem in neurosurgery, especially in the acute and acute periods of hemorrhage.
Author of the article: neurosurgeon Anton Viktorovich Vorobiev Frame around the text
Why choose us:
- we will offer the most optimal treatment method;
- we have extensive experience in treating major neurosurgical diseases;
- We have polite and attentive staff;
- Get qualified advice on your problem.
Surgical interventions for vasoconstriction. Coronary angioplasty
Today, there are several non-invasive techniques that are effectively used to narrow blood vessels.
The most popular methods in modern endovascular (vascular) surgery include angioplasty and stenting.
Minimally invasive vascular surgery is performed through a small puncture or incision in the patient's skin. The surgeon first inserts a needle with a special core - a stylet - into the hole made, and then a catheter - a thin hollow tube. The progress of the procedure is monitored using an X-ray monitor. Moving the catheter up the bed of the vessel, it is brought to the site of narrowing of the artery, localized in advance by angiography. Depending on the specific procedure, a stent or balloon is attached to the end of the catheter.
The lumen of a healthy artery is uniformly wide and the walls are smooth. Age and atherosclerosis provoke the appearance of deposits on the walls of blood vessels, consisting of fibrous tissue, calcium and cholesterol. These are so-called atherosclerotic plaques. The more such plaques on the walls of the arteries, the more the lumen of the vessel narrows and the blood flow worsens. Eventually the narrowing reaches a critical degree and normal blood flow becomes impossible. Ischemia (insufficient blood supply) develops and, as a result, pain and even necrosis (death) of tissue.
Angioplasty (balloon) is most often used to treat diseases of peripheral vessels, and sometimes to restore the functional patency of veins. In addition, it is the only medical alternative to coronary artery bypass surgery, in particular because it does not require an incision for manipulation, is performed under local anesthesia, and the recovery period after surgery is quite short.
Stenting is used when it is necessary not only to expand the lumen of a vessel, but also to reinforce it by placing a stent - a miniature wire frame.
Indications for surgery
Traditionally, vascular surgery is indicated for all patients with moderate to severe vasoconstriction.
A significant blockage of the vessel (the tip of the catheter does not pass through the narrowing site) may be a contraindication.
Complications that occur after stenting
The possibility of complications after stenting cannot be excluded:
- bleeding at the catheter insertion point;
- formation of a channel between a vein and an artery;
- high risk of blood clots forming around the stent (in the first months after surgery);
- the occurrence of restenosis;
- blockage of the lumen of the artery below the site of narrowing;
- blood clot formation in an artery;
- renal failure;
- weakening or rupture of the vessel wall;
- allergy to contrast;
- arterial wall dissection
Coronary angioplasty surgery
Preoperative preparation for coronary angioplasty (transluminal reconstruction) consists of a complete examination of the patient, during which the following must be carried out:
- X-ray examination of the chest;
- electrocardiogram;
- laboratory tests of urine and blood;
- X-ray contrast tolerance test (if an angiographic examination of the heart vessels is prescribed before surgery)
Before surgery, it is recommended to abstain from eating. Regarding taking medications (especially antidiabetic drugs), you should consult a cardiologist.
Specifics of the procedure
A catheter is inserted through the patient's femoral artery and passed to the narrowed section of the artery for intraoperative coronary angiography, during which the location and stage of narrowing of the arterial lumen is identified.
Based on the data obtained, the cardiac surgeon selects a balloon of the appropriate size and a suitable guide catheter. In order to prevent blood clots and further thin the blood, the patient is prescribed heparin.
A guide catheter is a thin wire with a radiopaque tip that is inserted into the patient's diseased coronary artery. Having received a complete picture, the cardiac surgeon directs the guidewire to the right place.
The tip is brought out beyond the narrowing of the artery lumen.
After this, a balloon catheter is inserted through the guidewire, which delivers the balloon to the site of narrowing. Once inflated, the balloon expands the lumen of the artery, flattening the plaque. If the purpose of the operation is to place a stent, then when the balloon is inflated, it is pressed into the wall of the vessel, reinforcing the affected area and preventing it from narrowing.
Effect and rehabilitation
As a rule, as a result of a successful coronary angioplasty operation, blood flow in the coronary vessels is significantly improved and the likelihood of coronary artery bypass grafting is significantly reduced.
To minimize the manifestations of the underlying disease, you should adhere to the diet prescribed by your doctor, refrain from smoking and eliminate stressful moments.
Within six hours after a successful operation, the patient is allowed to get up and walk, but he spends the first two days in the inpatient department of the cardiac center.
The rehabilitation period lasts on average a week.
Treatment of pathology
Emergency treatment for patients with a ruptured brain aneurysm includes restoring deteriorating breathing and reducing intracranial pressure.
There are 2 main treatment options.
They allow you to fasten the intracranial protrusion of cerebral vessels.
- Surgical clipping.
- Endovascular embolization.
If possible, treatment is given within the first 24 hours after bleeding to close the ruptured aneurysm and reduce the risk of recurrences that affect the blood vessels.
Let's consider the features of both methods.
Surgical clipping
The goal of the intervention is to apply a special clip to the neck of the aneurysm. This allows you to exclude it from the general bloodstream without blocking a normal vessel. If the aneurysm cannot be clipped, alternative techniques are used (wrapping, tripping, etc.).
Important! The operation to clip the cerebral vessels is performed with craniotomy. Microsurgical techniques are used to carry out the intervention. This allows you to free the aneurysm (its neck) from the feeding vessels. Complications after surgery arise from a previous rupture. Eliminating all its consequences is not so easy. When treating unruptured aneurysms, complications occur less frequently (in 4-10% of cases).
Request a call back Get a free consultation
How much do endovascular surgeries cost?
The cost depends on the type and extent of endovascular surgery. For example, sometimes, if necessary, two or even three stents can be installed in the coronary arteries during one procedure, and this will be more expensive. The amount will also be affected by factors such as pricing policy, star rating, clinics, level of doctors, length of hospitalization, additional studies, and treatment procedures.
The Medica24 International Clinic does not provide treatment for acute vascular disorders, including transient cerebrovascular accidents, as well as all types of acute cerebral circulatory disorders with persistent damage to brain tissue, incl. hemorrhagic and ischemic strokes. In case of suspicion of the occurrence of this condition, in accordance with the requirements of the legislation of the Russian Federation - The procedure for providing medical care to patients with acute cerebrovascular accidents (approved by order of the Ministry of Health of the Russian Federation dated November 15, 2012 No. 928n) -
You should contact the hotline of the Moscow Emergency and Emergency Service for subsequent hospitalization at the territorial vascular center. ONLY early provision of specialized neurological care will ensure the fastest and most complete recovery after a stroke. Above is reference medical information aimed at increasing the general awareness of citizens about cerebral vascular disorders. (NOT AN ADVERTISING)
The material was prepared by oncologist, endoscopist, chief surgeon of the international clinic Medica24, Konstantin Yuryevich Ryabov.
Sources:
- Endovascular surgery of the aorta and peripheral arteries // International Journal of Interventional Cardioangiology. 2005. No. 7.
- Shukurov B.M., Chigogidze N.A., Kozlov G.V., Pisetsky P.B., Egin E.I., Dushkina A.P. Endovascular embolization of the patent ductus arteriosus with a new type of detachable coils // International Journal of Interventional Cardioangiology. 2003. No. 1.
- Shukurov B.M., Kozlov G.V., Dushkina A.P., Nemchuk V.A. Endovascular surgery in the treatment of congenital pathology of the heart and blood vessels // International Journal of Interventional Cardioangiology. 2006. No. 11.
Progress of the aortic aneurysm resection operation
- Surgical approach
During the preoperative examination, a decision is made regarding the surgical approach. Most often, three accesses are performed. Two of them are in the groin area on the thigh, to isolate the common femoral arteries, one access is a median laparotomy (an incision in the middle of the abdomen) or an access on the left side. For tall aneurysms, the superior approach can be extended into the chest. This intervention is thoracophrenolumbotomy.
- The meaning of the operation
After isolating the aneurysmal sac, the abdominal aorta is clamped. The time for blocking blood flow must be reduced. To do this, before installing the clamp on the aorta, a good isolation of the aneurysm and all arterial branches up to the bifurcation of the aorta into the iliac arteries is performed. When vascular clamps are applied, the lumen of the aneurysm is opened, thrombotic clots are removed from the aneurysm cavity and bleeding from the branches flowing into the aneurysm is stopped.
Open intervention consists of replacing the enlarged section of the aorta with a synthetic vascular prosthesis. The latter is sewn into the upper section of the aorta (above the aneurysm), then the branches of the prosthesis are carried to the femoral arteries and sewn to them. After this, the prosthesis is covered with the walls of the aneurysmal sac. The main problem is the identification of the aneurysmal sac and the branches emanating from it. This must be done quickly enough if these branches are passable, since prolonged compression can cause disruption of the nutrition of the intestine or spinal cord.
After connecting the aorta to the femoral arteries, it is necessary to decide on the need for transplantation of the inferior mesenteric artery. This artery supplies blood to the colon, and sometimes ligating it can lead to disruption of the intestinal blood supply. To make a decision, it is necessary to evaluate the blood flow through this artery. If, after removing the clamp, there is good reverse blood flow, then the artery does not need to be sutured to the vascular prosthesis; if it is passable, but the blood flow is very weak, then the bypass paths are undeveloped and the arteries need to be replanted into the vascular prosthesis.
After completion of the vascular stage of the operation, tubular drains are installed in the retroperitoneal space and in the access area on the thighs, and the wounds are sutured layer by layer.
The average duration of surgery for an aortic aneurysm is 3 hours. The average volume of blood loss is about one liter. Blood loss is replenished with donor blood, plasma and saline solutions.
Anesthesia during surgery
The operation can be performed under general anesthesia or under epidural anesthesia (injection in the back). General anesthesia is required for large aneurysms extending to the level of the renal arteries or higher. General anesthesia is required for access using a wide midline laparotomy. With retroperitoneal access to the aorta, epidural anesthesia can be limited. During operations for an aneurysm, cardiac activity and blood pressure must be monitored using special equipment. For anesthesia and intensive care, a catheter must be installed in the central vein (most often the subclavian). Kidney function is assessed by the amount of urine, for this purpose a catheter is inserted into the bladder. During anesthesia, the level of central venous pressure is monitored and drugs are administered to regulate the volume of circulating blood and electrolytes. If necessary, blood and plasma transfusions are performed to replace those lost during surgery. Special dispensers administer drugs that regulate blood pressure levels. During a long operation, a hemofiltration device may be connected to eliminate possible intoxication. Anesthesia during aortic surgery is very important and the comfort of surgeons and the immediate results of surgical intervention depend on its course.