Infectious myelopathy
Viral damage to the spinal cord is accompanied by specific types of myelitis. In the past, the most common spinal cord infection was polio. Currently, the most common cause of viral myelitis is herpes zoster, which initially produces radicular symptoms. The pathological process in herpes zoster affects not only the gray matter of the spinal cord, as in polio. Lymphocytes are always found in the cerebrospinal fluid (CSF, cerebrospinal fluid) of patients.
MRI of the cervical spinal cord in infectious myelitis: c — axial T2-weighted image shows that the spinal cord lesion occupies its central part; d — enhancement of the pattern of the spinal cord lesion on the axial T1-weighted image after administration of a contrast agent.
Intramedullary spinal cord abscesses have been described in systemic spinal cord infections of bacterial and mycobacterial etiology. Chronic lesions of the spinal cord membranes during syphilis can lead to sluggish secondary subpial myelitis and radiculitis. Severe granulomatous, necrotizing and inflammatory myelitis is typical of Schistosoma mansoni infestation. Granulomatous, necrotizing and inflammatory myelitis is caused by a local reaction to tissue-digesting enzymes produced by parasite eggs.
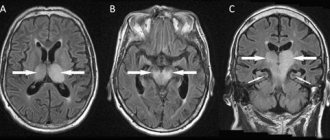
Magnetic resonance imaging (MRI) of the spinal cord for myelitis due to Zika virus infection. A - T2 MRI of the spine showing increased signal in the thoracic region T5-T8 (indicated by arrow) and enlargement of the cervical spinal cord. B, STIR MRI of the spine shows signal enhancement in the cervical spinal cord C4–C7 (arrowed).
Causes of development and classification of myelitis
Myelitis can be triggered by a variety of reasons and can occur in different scenarios. Most often, the cause of its development is infection. Pathogens include influenza, scarlet fever, typhus, polio, pneumonia, rabies, measles and other infectious diseases. The consequence of such conditions is most often transverse myelitis - inflammation in its most acute form.
The second reason why myelitis begins to develop is intoxication, leading to inflammation. In addition, injuries that affected the spinal cord, incorrect injections of drugs and punctures should be considered as the cause of myelitis.
In addition to the main reasons mentioned above, these may include factors such as hypothermia and various immunosuppressive conditions.
According to etiology, myelitis is classified into five types:
- viral;
- infectious;
- traumatic;
- toxic;
- post-vaccination myelitis.
According to the mechanism of its development, the disease is divided into primary and secondary types. In this case, secondary myelitis is a consequence of other diseases.
Based on the duration of its course, myelitis is differentiated into three main types: acute, subacute and classic. There are several types of this inflammation based on prevalence. This is diffuse, multifocal and localized myelitis. Transverse myelitis in this classification belongs to limited, as it represents a small focus of the disease.
Spinal arachnoiditis
Spinal arachnoiditis is an inflammation accompanied by scarring and fibrous thickening of the arachnoid membrane of the spinal cord. Spinal arachnoiditis can lead to compression of the nerve roots and sometimes the spinal cord. Spinal arachnoiditis can also be a postoperative complication or aftereffect from the introduction of radiocontrast agents (for myelography), antibiotics and other chemicals into the subarachnoid space.
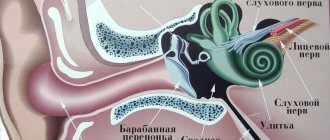
Anatomy of the membranes of the spinal cord and surrounding structures of the spinal canal.
Soon after an adverse effect, a large number of cells and a high concentration of protein can be detected in the cerebrospinal fluid (CSF, cerebrospinal fluid), but then the inflammatory process subsides. In the acute period of spinal arachnoiditis, the patient may have a slight increase in temperature. Bilateral asymmetrical radicular pain in the extremities may also be expressed. With spinal arachnoiditis, signs of compression of the roots are determined in the form of loss of tendon reflexes. Back pain and symptoms of root irritation are associated with lumbar arachnoiditis more often than should be the case. In addition, spinal arachnoiditis is not a common cause of spinal cord compression.
Approaches to the treatment of spinal arachnoiditis among neurologists and neurosurgeons are controversial. In some patients, improvement occurs after laminectomy (removal of part of the vertebral arch). Multiple meningeal arachnoid cysts located along the nerve roots may be a congenital anomaly. Increasing in volume, these arachnoid cysts cause deformation or stretching of the spinal nerve roots and ganglia, causing severe radicular pain in adult patients.
Treatment of myelitis
Treatment of myelitis depends on how much the spinal cord is affected and which segment of it is affected by inflammation. Acute myelitis is the most complex and severe form of the disease, in which the patient requires urgent surgical intervention. The operation eliminates pressure on the vertebrae and spinal canal, leading to pain. The high temperature that accompanies myelitis is relieved by a course of antibiotics and relief from inflammation.
Any myelitis requires urgent treatment, otherwise motor function may be lost forever. The course of myelitis therapy carried out with already bedridden patients includes measures to combat bedsores: treating the skin with camphor oil, regularly changing bed linen, placing rubber rings. If bedsores do appear, the damaged tissue is excised and a bandage is applied with Vishnevsky, penicillin or tetracycline ointment. Prevention of new bedsores is carried out using ultraviolet irradiation of the buttocks, sacrum and feet.
Along with bedsores, patients may experience dysfunction of the pelvic organs. The cause of these failures is an ascending urogenital infection that accompanies myelitis, which also needs monitoring and appropriate treatment. Initially, anticholinesterase drugs are used to remove urine. If they are ineffective, catheterization and rinsing of the bladder with antiseptic solutions is necessary.
To return the patient to full movement, the doctor prescribes dibazole, prozerin and vitamin B. Taking these medications is most often combined with passive gymnastics and therapeutic massage.
Myelitis in any form is an inflammatory disease that requires maximum doses of broad-spectrum antibiotics. To reduce the intensity of pain, antipyretics are used simultaneously with ACLT 40 units twice a day for 2-3 weeks and glucocorticoid hormones 50-100 mg per day. The latter can be replaced with dexamethasone or triamcinolone.
Symptoms
| Occurrence (how often a symptom occurs in a given disease) | |
| Severe pain in the lumbar region | 90% |
| Gait disturbance, difficult to specify (abasia) | 80% |
| Numbness of the lower body | 80% |
| Numbness of the foot (foot hypoesthesia) | 70% |
| Urinary retention | 60% |
| Constant pain in legs | 50% |
| Spontaneous release of urine without the urge to urinate | 40% |
| Rapidly increasing muscle weakness in the legs | 0% |
Course of the disease
Researchers talk about three options for the development of the disease. In acute transverse myelitis, neurological symptoms are observed within two weeks. After this comes the recovery stage. Later, for an indefinite period, residual effects persist or gradually disappear.
In the second option, the main symptoms remain for life.
The third type, like many other neuromuscular pathologies, is characterized by the gradual development and ascending spread of the inflammatory process with subsequent damage to the trunk. Demyelinating lesions appear in the brain.
Clinical picture
Clinical manifestations of myelitis occur acutely, less often subacutely, against the background of general intoxication (fever 38–39 °C, severe chills, general malaise). Then the appearance of moderate pain, paresthesia in the legs and lower back is noted. After a few days, paresis and sensitivity disorders, and urination disorders gradually increase.
An objective examination of the patient reveals general intoxication syndrome (60%), peripheral lower paraparesis/paraplegia with muscle atrophy (80%), absence of tendon reflexes from the legs (90%), sensory disturbances of the conductive type below the level of the lesion (70%), allodynia ( 40%), pelvic dysfunctions such as true fecal and urinary incontinence.
Prevention and prognosis of myelitis
There is no specific prevention in this case. Considering that myelitis is a consequence of other diseases, injuries and various types of interventions, it is advisable to consider prevention of diseases that will cause it as prevention in this situation. These include infectious diseases: polio, mumps, measles and the like. Experts recommend vaccination as one of the means to combat them. Preventive measures include timely treatment of other infectious diseases when their first symptoms appear.
The prognosis depends on how severely the patient's spinal cord is affected. With timely and adequate treatment, improvement occurs within six months, and full recovery occurs after 1-2 years. If no positive dynamics are observed by this time, we should talk about disability.
The area of localization also plays a significant role. Thus, upper cervical myelitis can be a direct cause of death. Thoracic and lumbar myelitis without timely diagnosis and proper treatment leads to loss of motor function of the lower extremities. The prognosis is significantly worse if myelitis is accompanied by other pathologies: cystitis, pyelonephritis, pneumonia and frequent extensive bedsores.
Complications
The consequences of myelitis include paralysis of the legs and other parts of the body. The progression of severe forms sometimes leads to damage to the nerves that innervate the respiratory system and heart.
The development of transverse myelitis is indicated by high temperature, pain in the back, increased muscle rigidity, paralysis, spasms, and loss of sensitivity. Based on the diagnostic results, treatment is prescribed aimed at combating the causes of the disease and eliminating the symptoms. The consequences of the disease are irreversible if treatment is not started in time.
To prepare the article, the following sources were used: Bakulin I. S., Vasiliev A. V., Bryukhov V. V., Stoyda N. I., Zakharova M. N. Differential diagnosis of myelitis in demyelinating diseases // Journal of Nervous Diseases - 2021.
Muradyan I. E., Martsenyuk S. K., Evtushenko S. K., Simonyan V. A., Goncharova Ya. A. Cases of acute transverse myelitis: clinical features, diagnostic difficulties // International Neurological Journal - 3 (33) 2010 .
Pathogenesis
The development of the disease begins with swelling of the spinal cord, which leads to circulatory disorders and blood clots. The processes contribute to the occurrence of even greater swelling. Thus a vicious circle arises.
Subsequently, poor blood circulation in some areas of the spinal cord stops altogether, causing necrotic processes and softening of tissue structures. Subsequently, during the recovery period, a scar forms in place of the dead tissue and these areas of the organ are not able to perform their previous functions. Therefore, some symptoms that occur during illness may persist for the rest of your life.
Our specialists
Tarasova Svetlana Vitalievna
Expert No. 1 in the treatment of headaches and migraines. Head of the Center for the Treatment of Pain and Multiple Sclerosis.
Somnologist.
Epileptologist. Botulinum therapist. The doctor is a neurologist of the highest category. Physiotherapist. Doctor of Medical Sciences.
Experience: 23 years.Derevianko Leonid Sergeevich
Head of the Center for Diagnostics and Treatment of Sleep Disorders.
The doctor is a neurologist of the highest category. Vertebrologist. Somnologist. Epileptologist. Botulinum therapist. Physiotherapist. Experience: 23 years.
Bezgina Elena Vladimirovna
The doctor is a neurologist of the highest category. Botulinum therapist. Physiotherapist. Experience: 24 years.
Volkova Svetlana Anatolevna
Head of the Center for Parkinsonism and Extrapyramidal Diseases.
The doctor is a neurologist of the highest category. Epileptologist. Ozone therapist. Physiotherapist. Experience: 26 years.
Dolgikh Tatyana Anatolevna
The doctor is a neurologist of the highest qualification category. Experience: 24 years.
Zhuravleva Nadezhda Vladimirovna
Head of the center for diagnosis and treatment of myasthenia gravis.
The doctor is a neurologist of the highest category. Physiotherapist. Experience: 16 years.