Metastasis is the migration of carcinogenic cells from the primary tumor to other organs, which is typical for most cancer tumors. This leads to the formation of secondary lesions in other tissues. Different types of cancer are characterized by different intensity of the metastatic process, which depends on the degree of malignancy and characteristics of the primary tumor. The more intense the spread, the more aggressive the cancer. For example, with skin melanoma, metastases to the brain occur frequently, unlike basal cell carcinoma. The metastatic process begins, as a rule, at the third stage of carcinogenesis, and at the fourth stage it already manifests itself quite strongly. There are two ways for cancer cells to migrate: through the blood and lymph. The appearance of metastatic tumors will be identical to the appearance of the cells of the primary tumor. When neoplasias are detected in the brain, it is important to ensure that these are secondary tumors. For this purpose, a complete examination of the body is carried out. In the presence of metastases in the brain, the prognosis worsens, life expectancy is estimated at months, in some cases weeks.
Metastasis formation
Metastases form after the development of a primary malignant neoplasm in other organs. The latter are formed as a result of mutagenesis or errors in the genetic material of somatic cells. At the initial stages, there is no metastatic process, but as it progresses, the tissues of the primary tumor grow into nearby organs. In the future, the disease worsens, cancer cells begin to break away from the primary focus and migrate through the blood or lymphatic channels (the integrity of the blood vessels is damaged). A metastatic cell attaches itself to an organ, germinates, and gives rise to a new lesion—a secondary tumor.
Important. In different individuals, the nature, timing and intensity of the formation of secondary metastatic foci are different, which is explained by the level of antitumor immunity.
Features of metastasis
The intensity of the metastatic process, the degree of malignancy, the formation of relapses, the treatment of brain metastases and the aggressiveness of cancer are influenced by the following circumstances:
- Stage of carcinogenesis. The life prognosis directly depends on the stage at which the cancer was discovered and surgically removed. The most successful will be removal of cancer at the first stage, however, this cannot guarantee a complete cure, so the patient must be constantly monitored.
- The location of the primary tumor largely determines the nature of the metastatic behavior of cancer and damage to other organs.
- The histological structure and form of cancer also influence the reasons for the spread of metastases. The most dangerous are poorly differentiated forms. Different types of carcinogenesis are characterized by different features of cancer cell migration. If the tumor is dense and slowly growing, for example, cylindroma, then metastases to the brain are rare and, as a rule, only in the terminal stages. In other cases, even with good antitumor immunity, metastases form in the brain, for example, with the development of melanoma.
- Features of anticancer therapy. If it is possible to completely remove the primary tumor in the initial stages, with the administration of radiotherapy and chemotherapy, then in this case the treatment gives the most acceptable result.
- The older the patient, the more difficult the cancer is to treat.
How can metastases be detected?
Breast cancer metastases are diagnosed using CT, MRI, and ultrasound. A chest x-ray is performed. A valuable method is positron emission tomography: during the study, a substance with a radioactive label is injected into the body, which accumulates in cancer cells and makes them “glow” in pictures taken by a special device. In a similar way, but using different radiopharmaceuticals, a bone scan is performed.
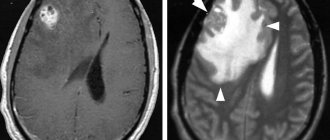
Metastases to the brain
Lead to the formation of secondary tumors in various parts of the brain. This almost always causes death. In general, any type of cancer can lead to this, but there are tumors that metastasize more often than other types of cancer:
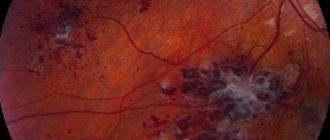
- Metastases to the brain in skin cancer (melanoma) are more common than in other types. Approximately 50-73% of patients face this problem. In 10-45% of cases (at the time of diagnosis), melanoma is at stage 4, when there are already metastatic lesions. At the same time, every third patient exhibits neurological manifestations. In this case, a condition similar to a stroke often develops, because a hemorrhage forms in the pathological neoplasm. Treatment of brain metastases in melanoma is complicated by the fact that they are poorly sensitive to radiotherapy.
- Metastases in lung cancer form in 35-60% of cases. In this case, how long people live with brain metastases is determined by many factors (age, type of cancer, intensity of carcinogenesis, presence of metastatic lesions in other organs, and so on). According to statistics, such metastases in lung cancer are the most dangerous in terms of mortality. Most often they are characteristic of the fourth stage of pathogenesis. Only in 5% of cases will the patient live 2-3 years. As a rule, at this time there are already multiple neoplasms in the lymph nodes and other organs. The patient receives palliative treatment.
- In breast cancer in women, metastases to the brain are recorded in 20-30% of cases. At later stages, metastases are diagnosed in the brain and many other organs. Treatment is carried out with radiochemotherapy and hormone therapy. The quality of life deteriorates significantly, stroke, mental disorders, vertebral fractures due to brittle bones, cough due to lung damage, and so on are possible.
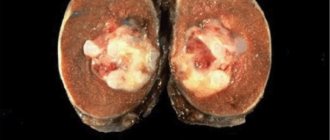
- Brain metastases in kidney cancer are characteristic of stage 4. In this case, there are secondary lesions in other organs (second kidney, lungs, other organs and multiple lymph nodes). The prognosis is unfavorable: only 8% of patients will live for about two years. Kidney cancer has a high risk of recurrence.
- Metastases from bladder cancer can be at the fourth stage. The prognosis is negative due to the presence of secondary tumors in other organs; most patients will not live more than a year. Removing the cancer is almost impossible; supportive treatment is prescribed.
- Brain metastases in intestinal and esophageal cancer are observed at stage 4. If they are present in other organs, the prognosis is negative - only 6% of patients will live more than a year.
In addition to these types of cancer, metastatic brain lesions can also form in other malignant neoplasms, for example, in the terminal stages of laryngeal or thyroid cancer, when the tumor grows into large main arteries.
Modern treatment technologies prolong the life of cancer patients.
This leads to the fact that patients “survive” until metastasis occurs in those organs and systems that are not quite typical for this pathology. The peculiarity of damage to the central nervous system is an extremely unfavorable prognosis, which forces clinicians to carry out urgent therapeutic measures because of this, even in the presence of dissemination of the process and multiple lesions of other organs and tissues. However, timely and multicomponent treatment, taking into account individual indications, can extend the life of patients for many months and even years. In this case, rapid diagnosis and choice of treatment tactics—radiation and chemotherapy, targeted agents and angiogenesis inhibitors—as well as surgical intervention if necessary are of particular importance.
At present, standards of care for this category of patients have not been developed, and treatment is carried out empirically depending on the training and individual characteristics of the doctor.
The condition of this category of patients is characterized by instability and a high risk of developing cerebral edema, especially in connection with the start of radiation therapy. This requires preventive administration of glucocorticoids, usually dexamethasone at a dose of 8-36 mg/day.
For severe symptoms, administration of 20 mg or more, followed by a decrease to 4 mg 2 times a day, is accompanied by regression of neurological pathology and pain. However, despite the positive effect in terms of relief of neurological symptoms, patient survival and response rates to antitumor therapy do not change.
With steroid therapy alone, life expectancy does not exceed 2 months, radiation therapy increases it to 5, and a combination of radiation and chemotherapy allows an average survival of about 6-9 months. The average life expectancy of patients with a high Karnofsky index, the absence of meningeal and extracranial spread, as well as with a limited extracerebral process amenable to antitumor therapy can reach a year or more. Indications for surgical intervention are infratentorial lesions with signs of ataxia and large-volume solitary metastases (especially cystic structure) located in the hemisphere. By combining radiation therapy with excision of metastases, long-term patient survival rates are improved, which is also observed in the case of high-dose precision irradiation (gamma and cyber knife). In case of multiple lesions and the need to irradiate the entire volume of the brain, fractionation modes do not play a significant role.
The main approach to conventional radiation therapy for brain metastases is irradiation of the entire volume, usually in an accelerated manner, although randomized studies in this direction are ongoing. Before the introduction of this highly effective radiation therapy technique into everyday clinical practice at the turn of the 50s of the twentieth century. The median survival of this group of patients did not exceed 1-2 months. In most situations, to prevent edema during the first few days of irradiation, it is necessary to prescribe dexamethasone 12-30 mg, followed by a sharp reduction in the dose by half.
Two lateral opposing fields are used. Particular attention is paid to the adequacy of inclusion in the scope of exposure of the base of the skull and the posterior cranial fossa. In this case, either the eyes are shielded or the fields are deployed in accordance with the projection of the base of the skull so that the lower borders are located at the level of the II cervical vertebra. A single focal dose can range from 2.5 to 4-5 Gy, the total - 20-35 Gy. The calculation is carried out on the middle plane. As a rule, a pronounced regression of metastases and relief of neurological symptoms are observed. At the same time, in accordance with IAEA recommendations, it is practiced to increase the dose rate to 4 Gy from the point of view of economic feasibility, since fractionation regimes do not significantly affect the long-term prognosis. It should be taken into account that significantly accelerated fractionation, in contrast to the traditional dose of 30 Gy in 10 sessions, may be accompanied by an increased risk of new intracerebral metastases due to a lower total physical absorbed dose. However, the standard approach in most clinics remains daily irradiation of the entire brain volume at a dose of 3 to 30-33 Gy. The fear of long-term complications of this type of treatment is often exaggerated given the life expectancy of patients. Impaired cognitive functions in patients with total brain irradiation are noted immediately after the start of radiation therapy. This persists after treatment, but is limited only to verbal memory and should not be used as a reason to refuse treatment.
The presence of single metastases implies local supplementation directly to the lesions up to doses equivalent to 50-60 Gy, usually in an accelerated fractionation mode. With a small number of metastases (1-3), local conformal hypofractionated irradiation is permissible (ROD 5-6 Gy, SOD 18-30 Gy). Particular attention should be paid to simultaneous or synchronous chemoradiotherapy. Violation of the permeability of the hematological barrier due to tumor growth and/or surgical intervention leads to rapid regression of metastases when cytostatics are prescribed during radiation treatment. At the same time, good results are achieved with the use of drugs traditionally used for these nosological forms, despite their supposedly poor penetration through the BBB. Nitrosourea drugs – lomustine, carmustine, fotemustine (mustoforan) – are actively being tested as part of synchronous chemoradiotherapy. In recent years, encouraging results have been obtained with the use of temozolomide (temodal), which was originally intended for the treatment of malignant gliomas.
In the case of stereotactic radiation exposure, a single irradiation of metastases is performed at a dose of 20-30 Gy. Indications for this method are a limited number of deposits (no more than 5-10), their maximum size is no more than 3-4 cm, the absence of a pronounced mass effect and occlusive hydrocephalus. In a certain sense, stereotactic irradiation competes with surgery when these techniques are combined with total brain irradiation. The best results with stereotactic radiosurgery are achieved in the case of small lesions whose diameter does not exceed 1.5-2 cm. However, increasing the distance from the tumor edge by more than 1 mm does not lead to an increase in the effectiveness of irradiation. Such tactics can be used even with an increase in the number of metastases and their localization in vital areas - the brain stem and cavernous sinus. The median survival rate for gamma knife radiation varies from 5-6 months for melanoma metastases to a year or more for renal cell carcinoma. Focal brain damage without a primary detected tumor is accompanied by the worst treatment results, survival does not exceed 3 months. However, in the absence of extracranial metastases and systemic chemotherapy, acceptable results are sometimes achieved. In some centers, surgical removal of metastases is accompanied by the installation of a system with radioactive iodine-125 (GliaSite) or a sponge with chemotherapy drugs (nitrosourea, anthracyclines) into the postoperative cavity. At the same time, a combination of these techniques with total brain irradiation is very promising. Supplementing irradiation of the entire brain volume with stereotactic radiosurgery and/or surgery can increase the median survival rate by 1.5-2 times. However, researchers continue to debate about the advisability of combining postoperative stereotactic irradiation with total exposure to the brain. The combination of stereotactic and total brain irradiation does not greatly affect patient survival compared to local exposure alone, but the frequency of detection of new lesions is reduced by approximately 1.5 times. Total brain irradiation is an adequate method for both independent treatment of metastatic lesions of the central nervous system and in combination with stereotactic irradiation. It is primarily indicated for multiple lesions and poor general condition of the patient. In the case of resection of single metastases or radiosurgery, total cranial irradiation is a reasonable adjunct in most clinical situations.
As the process progresses and new metastases appear in the brain, repeated total irradiation is possible. Indications are good effectiveness and tolerability of the first course, a period of at least 6 months after the previous radiation exposure and satisfactory general condition of the patient. With repeated irradiation, complete and partial response rates can reach 70%. Some authors have called for wider use of stereotactic radiosurgery in these cases.
Irradiation of patients with metastatic lesions of the spinal cord and/or spine with transition to nerve structures is carried out according to the same principles. Typically, a posterior straight vertebral field or two paravertebral ones are used at angles with the capture of the transverse processes of the vertebrae and indentations from the boundaries of the lesion in the craniocaudal direction of about 2 cm. Radiation therapy is carried out in an accelerated mode - 3 Gy × 10 times, 4-5 Gy × 4-5 times daily or (on an outpatient basis) 2-3 sessions per week. Since economically feasible fractionation regimens for bone metastases have been developed, there is a clear trend toward single irradiation of the spinal cord with a single absorbed dose of 8 Gy. Moreover, its effectiveness in terms of relieving and preventing pain and neurological (spinal cord compression) syndromes does not differ from fractionated ones. If necessary, repeated exposure is possible. A change in treatment tactics for this unfavorable contingent of patients using a combination of methods has led to an increase in average life expectancy to 1.5-2 years or more with a relatively torpid course of the underlying disease. Currently, general practitioners should consider patients with brain metastases to be treated actively rather than just symptomatic medical radiotherapy.
Symptoms and signs
As cancer progresses, it enters later stages (3 and 4). In this case, metastases form in the brain, so characteristic clinical signs begin to appear. Manifestations will depend on the area of the brain affected. In many cases, the signs are mirrored, i.e. if the tumor is in the right hemisphere, then the clinic will appear on the left side and vice versa.
Main features:
- dizziness, headache due to increased pressure inside the skull, while negative symptoms are not relieved by medications;
- dyspeptic symptoms, nausea and vomiting (vomiting does not bring relief), which is not associated with poisoning;
- various disorders of brain activity: confusion, memory impairment, speech impairment, epileptic seizures, hallucinations, etc.;
- vision, hearing, and smell suffer;
- the mental and emotional background changes, the person becomes rude, aggressive, overly irritable;
- the formation of epileptiform seizures with brain damage is more typical for the elderly;
- motor activity is impaired, coordination and fine motor skills suffer, it is difficult for the patient to maintain balance, gait is impaired, the ability to write, and so on.
How to treat breast cancer with metastases?
Surgery is usually ineffective, but some palliative interventions can help relieve symptoms and improve quality of life:
- For tumors that are accompanied by an open wound or skin ulcer. If there are single operable metastases. If the tumor spreads to the spinal cord. For liver metastases, which lead to impaired bile outflow, portal hypertension and ascites. To reduce pain and other symptoms.
The main methods of treatment for breast cancer with metastases are: radiation therapy, chemotherapy, targeted therapy, and hormonal therapy. The doctor chooses a tactic depending on the molecular genetic status of the tumor, the location of metastases, the patient’s state of health and concomitant diseases.
Diagnostics
Since the formation of secondary tumors in the brain causes the death of the patient, it is important to identify the presence of a pathological formation as early as possible. If cancer is present, the patient must be diagnosed continuously to monitor the situation and timely identify secondary tumors in the brain. If the tumor in the head is small, it usually already has a pronounced clinical picture, however, it can be diagnosed at the earliest stages using computed tomography (CT) or magnetic resonance imaging (MRI). A biopsy is important to establish the metastatic process and clarify all the nuances of pathogenesis. The presence of metastases can be suspected even with a biochemical blood test.
Modern methods of treatment
Severtsev Alexey Nikolaevich
Doctor of Medical Sciences, Professor, Surgeon-Oncologist
“For us there are no hopeless patients. It's always worth fighting for. Even if the diagnosis does not give hope for a cure, alleviating the condition and improving the patient’s quality of life is what we should strive for. Technologies are developing, new drugs are appearing, and every year our capabilities are growing.”
The choice of treatment tactics depends on several factors:
- Number of metastases (single, multiple).
- Location of metastases: along the periphery or near large blood vessels, bile ducts.
- Histological type of cancer: what tumor tissue looks like under a microscope, what cells it consists of.
Various types of treatment are used. In 5–20% of patients, it is possible to perform resection - removal of the affected part of the liver. There are also doctors in Russia who perform autotransplantation (Pilchmeier operation). In this case, metastases from the liver are removed “on the next table.” In 50% of patients, in addition to surgery, radiofrequency ablation and chemoembolization can be performed. Chemoembolization is a procedure during which an embolic drug in combination with a chemotherapy drug is injected into the vessel feeding the metastasis. The embolic drug consists of microparticles that block the lumen of the vessel, and the tumor tissue ceases to receive oxygen and nutrients. The chemotherapy destroys cancer cells. Radiofrequency ablation involves the destruction of malignant nodes with high-frequency current using a needle-electrode inserted through the skin.
The remaining 50% of patients have to be content with only palliative therapy, but they can also be helped.
- Systemic chemotherapy is usually ineffective because the liver breaks down most of the chemotherapy drugs and prevents them from reaching cancer cells. But chemotherapy drugs can be administered intraarterially, directly into the vessel feeding the tumor. Thanks to this, you can give a larger dose of drugs without fear of serious side effects. For liver cancer, the targeted drug sorafenib can be used; it is currently approved in Russia. Radiation therapy is rarely used. It does not improve patient survival, but sometimes helps relieve pain.
Treatment
What to do in case of metastases in the brain is decided by a council of doctors based on the diagnosis and medical history of the patient. Treatment of metastases in the head is very difficult, which is due to the inaccessibility of the location of secondary lesions in the brain, the presence of multiple tumors in other organs, the patient’s condition in the later stages, age and a number of other factors. Today, in the presence of secondary tumors in the head, stereotactic radiosurgical techniques are used, which stop or slow down the growth of pathological tissue. The best result is achieved when tumors are removed surgically, but at these stages treatment is always difficult. The method of treatment will depend on the location of the tumor, the intensity of damage to other organs and the general condition of the patient.
Main types of treatment
- Surgical treatment is possible only in cases where there is access to tumors in the brain. As a rule, in the terminal stages many other organs are already affected, so surgical treatment is carried out mainly for palliative purposes, to eliminate negative signs and alleviate the patient’s condition. In some cases, it is possible to remove a few tumors or metastases are removed en bloc (when they are located nearby). If there are many lesions in the brain, then surgical treatment is not advisable.
- Treatment with radiotherapy is more preferable in this case. For deep, hard-to-reach locations of secondary tumors in the brain, this type of treatment is the main one. For a few tumors, stereotactic proton therapy (irradiation of an organ from several sides) will be an effective method.
- Chemotherapy and drug treatment for brain metastases are not effective. Drugs are prescribed to relieve negative symptoms and reduce side effects. Thus, drug therapy is palliative.
Clinical manifestations of metastases
Symptoms depend on the size of intracranial tumor foci, their number and location. Basically, clinical symptoms can be divided into two groups:
- local, due to the location of the tumor in a specific part of the brain responsible for certain functions of a certain organ;
- general cerebral symptoms associated with the size of additional tumor tissue interfering with the functioning of the brain itself.
For example, a tumor near the structures that provide innervation to the eye will manifest itself as a loss of visual fields, when the eye does not perceive certain parts of the viewing sector. Many small nodes will give a picture of cerebral edema, since extra grams of tumor in a closed cranium interfere with the normal circulation of fluids and compress normal tissues.
In half of the patients, secondary brain tumors respond with headaches; very often the intensity of the pain changes along with the position of the head, when, when tilted at a certain angle, partial restoration of cerebrospinal fluid circulation temporarily leads to a decrease in pain. Unfortunately, over time, the growth of metastases will make the pain constant, and the confined space will lead to unbearable intensity. Dizziness and double vision are common when looking with both eyes.
Every fifth patient develops motor disorders up to paresis of half the body. Every sixth suffers from intellectual abilities, the same number suffers from changes in behavior, disturbances in movement and gait, seizures are slightly less common, but a completely asymptomatic course, when metastatic formations are detected only during examination, is also not uncommon. However, as the size of the tumor increases, even in such a relatively favorable situation, the functions of the body are quickly disrupted.
Swelling of the tissue around the tumor - perifocal edema, coupled with increased intracranial pressure (ICP) causes general cerebral symptoms with headache, dizziness, double vision, vomiting at the slightest movement or even when opening the eyes, constant hiccups, leading to depression of consciousness up to cerebral coma. A decrease in heart rate and breathing rate with very high “upper” systolic pressure indicates extremely high and potentially fatal intracranial pressure.
In practice, variants of the development of primary symptoms in cancer metastases to the central nervous system are distinguished according to the prevailing set of clinical signs.
- The apoplexy variant, similar to a stroke, develops acutely and is manifested by focal disorders - evidence of damage to a certain area of the brain. This option is usually associated with either blockage of the vessel or its rupture by a tumor, followed by hemorrhage into the brain.
- The relapsing-remitting variant is characterized by an undulating course, when the symptoms either decrease or progress, resembling atherosclerotic vascular damage.
In some patients, brain metastases are asymptomatic. They are discovered only during examination.
Get a treatment program
Stages of metastases
Metastasis signals the spread of tumor cells throughout the body - dissemination of cancer and generalization of the malignant process, but stage IV cancer is considered only when primary cancer with metastatic screenings is simultaneously detected.
In all situations, the stage is established once in a lifetime - after examination and initiation of treatment, the sequential detection of new tumor foci does not change the stage numbering; in the diagnosis after “stage I (II or III)” the localization of metastatic foci and the treatment performed for this purpose are indicated. For example, “stage I right breast cancer, condition after mastectomy, metastases to the left lung and skin, condition after 4 courses of chemotherapy.”
Recurrence of breast cancer. A patient’s story about treatment at the international clinic Medica24
In 2004, breast cancer was first diagnosed. After 16 years, metastasis began. Our patient talks about how she copes with cancer recurrence. Read full review
Review of the treatment of obstructive jaundice
The patient was admitted with severe signs of jaundice. During hospitalization, his condition stabilized. For this purpose, drainage of the bile ducts was carried out, as well as exposure to medications. After receiving the results of the histochemical study, further treatment tactics will be determined. Read full review
“They have golden hands”...
The patients are being treated at the international clinic Medica24. During the treatment, they managed to become friends and this time decided to record a joint review. They thank all the clinic staff for the high organization of all processes and the effectiveness of the procedures. Read full review
Chemotherapy - review by Olga Stepanovna
The patient is hospitalized for the third time. During a comprehensive examination, a puncture of the tumor was performed. Histological analysis made it possible to verify the diagnosis and determine treatment tactics. At the first stage of treatment, surgery was performed. The tumor was radically removed. Drug treatment is now being carried out to prevent the possibility of relapses. To date, the first course of chemotherapy has been completed. The patient was discharged home in satisfactory condition. Read full review
“You are the only clinical organization that brings benefits to people”...
The patient was admitted for treatment of cancer. The hospitalization lasted a week. The patient notes that they immediately responded to all his problems and provided assistance in a timely manner. He compares the international clinic Medica24 with other medical institutions. Patient about... Read full review
Review of the attending physician M.Kh. Mustafaeva
The patient was hospitalized in serious condition. Complex treatment was carried out. A positive effect has been achieved. The patient’s wife thanks her husband’s attending physician Milana Khanlarovna Mustafaeva. She says: “From the first day, from the first minute, as soon as we came to you, we immediately felt and understood each other. You understood the patient, you understood me. You have defined to the depth of the volume that we need. Although I couldn’t explain how... Read full review
Feedback on the treatment of breast disease
The patient was hospitalized with breast disease. By decision of the council, surgery was performed at the first stage of treatment. It was successful. On the third day the patient was discharged home. After histological examination, further treatment tactics will be determined. Read full review
Development of metastases
When the problem develops to the level of stage 3 cancer with metastases, the tumor becomes very active, quickly increases in size, growing into nearby tissues. In most cases, screenings are observed in distant lymph nodes. The prognosis takes into account factors such as the degree of differentiation and location of the tumor, and the general condition of the patient. These moments can both aggravate and reassure the patient’s situation. Successful treatment here is still quite possible.
How long do people live with metastases?
The life expectancy of a patient with metastases depends on the growth rate of tumor tissue and its sensitivity to therapeutic effects.
The specific location of the secondary cancer - lungs, bones, liver and other organs - matters for life expectancy only in terms of the technical capabilities of removing the metastasis. A single cancerous node can be removed, which will undoubtedly have a positive effect on the patient’s life expectancy; single and multiple neoplasms are mainly subject to drug treatment, the possibilities of which are limited. However, with high sensitivity to drugs, the patient’s life can be counted in years, and in some cases, complete regression of the tumor lesion is achieved.
The success of therapy is based on the professionalism of oncologists, who at each stage skillfully select the optimal - the most effective and individual treatment that improves the quality of life in the disease and prolongs life itself. This is the kind of help our Clinic offers.