Cavernoma (cavernous malformations, cavernous angiomas) is a group of rare vascular formations in the central nervous system.
The formations are represented by dense or loose multi-chamber cavities (cavities) filled with blood, with varying degrees of its disintegration. The tissue around the cavernoma is usually significantly changed, but sometimes is not affected.
Localization of tumors can occur in almost any area of the central nervous system. 70% of formations are found supratentorial (above the tentorium of the cerebellum). Cavernomas are found under the tentorium of the cerebellum in 30% of cases. Of the lobes, the frontal and temporal lobes are mainly affected. Tumors in the spinal cord are rare - up to 2%. The rarest localizations: cerebellopontine angle, dura mater of the anterior and middle cranial fossae, cavernous sinus, pituitary gland region.
Sizes can vary: from a few millimeters to 9 cm.
Formations can be single or multiple. Single ones occur in 80-90% of cases.
Many studies indicate a number of causes for the occurrence of cavernous angiomas:
- Hereditary (presence of gene mutations);
- Sporadic, i.e. tumors that arise spontaneously under unknown circumstances or in isolated cases. They account for the majority of cases, approximately 80%.
- Induced by radiological radiation. A large number of reported cases in children under 10 years of age;
- Congenital (formed at 3-8 weeks of pregnancy). Very rare.
Symptoms of cavernous angioma
The patient may have no symptoms, although headaches, seizures, or other focal symptoms, such as motor or sensory disturbances, are common. Most often, the occurrence of symptoms is associated with hemorrhages, which can occur both inside the cavernous angioma and in the surrounding brain tissue. Depending on the severity of the hemorrhage, conservative treatment or surgical intervention is used, which will be discussed below.
Cavernous angioma of the right frontal lobe. A CT scan without contrast enhancement shows a large heterogeneous mass in the right frontal lobe. The formation is characterized by high X-ray density in its central part and diffusely increased density in the periphery due to the presence of calcifications and small hemorrhages in the formation.
What danger does pathology pose?
The consequences of a cavernoma depend on its location. In addition to headaches, convulsions, nausea and vomiting, the tumor may be accompanied by mental disorders (inability to normally perceive the environment, loss of practical skills, lack of self-criticism). Due to the disease, loss of speech function and the presence of auditory hallucinations are possible. In many cases, there is an inability to swallow normally, epileptic seizures, and vascular ruptures. Particularly dangerous are hemorrhages, oxygen deprivation of the brain and paralysis.
The most terrible consequences of a cavernoma, which is localized in the dominant temporal lobe. If the respiratory or vasomotor system is damaged, death occurs.
Vascular malformations of the brain
Types of vascular malformations differ based on their macroscopic and microscopic characteristics. Typically, intracranial vascular malformations are divided into the following 4 groups:
- Capillary malformations (or telangiectasias)
- Cavernous malformations (cavernous angiomas/hemangiomas)
- Venous malformations
- Malformations with arteriovenous shunts
According to the newer classification, 2 more categories have been added: arterial malformations (without the formation of an arteriovenous shunt) and mixed malformations.
Cavernomas can be found in any area of the brain because they can arise anywhere along the vascular bed. Intracranial extracerebral cavernous angiomas sometimes occur, but they are quite rare. Cavernous angiomas are also sometimes found in the spinal cord, most often in association with multiple vascular lesions of the brain.
Detection of cavernous angiomas
Despite the fact that cavernous angiomas are visualized using computed tomography (CT), this method is not the method of choice: the fact is that the identified signs in a CT study may correspond not only to cavernous angioma, but also, among other possible options, poorly differentiated tumor.
The sensitivity of magnetic resonance imaging (MRI) is much higher, due to its higher contrast resolution, as well as its greater ability to image flowing blood and its breakdown products. The combination of different MRI pulse sequences has largely solved the problem of misdiagnosis or under-detection of cavernous angiomas, since these lesions have quite specific features on MRI.
Get an MRI of the brain in St. Petersburg
CT and MRI can be used for follow-up of patients with already diagnosed cavernous angiomas, especially in cases where there is a risk of hemorrhage. Although the MR image of cavernous angiomas does not predict the occurrence of bleeding, MRI is the method of choice for long-term follow-up of patients with cavernous angiomas, as well as for the evaluation of family members of the patient who are at risk of having such malformations. In addition, MRI is extremely useful in planning surgical intervention, as it allows you to assess the size of the formation, its boundaries, and thus determine the type of operation and surgical approach.
With classical angiography, most cavernous malformations are not visualized, and even when signs are detected, they are extremely nonspecific. If the lesion develops in combination with other vascular malformations, which occurs in approximately 30% of patients with venous malformations, then its MR characteristics become much more complex and less specific. In such patients, angiography may be useful to further clarify the diagnosis.
Complex of signs of pathology
Mostly the disease occurs without pronounced symptoms. Congenital cerebellar cavernoma often manifests itself when the patient reaches the age of twenty to forty years. Clinical picture of the disease:
- epilepsy attacks;
- increasing headaches;
- uncertainty, unsteadiness of gait;
- loss of movement coordination;
- weakening of visual and auditory functions;
- noise in ears;
- nausea, vomiting;
- absent-mindedness, memory lapses;
- decreased intelligence;
- paresis and paralysis;
- loss of sensation;
- hoarseness of voice.
Cavernoma can cause numbness of the limbs, twitching and paralysis of the tongue. Often the headache that accompanies the disease indicates a rupture of the walls of the tumor.
Cavernous angioma or tumor?
Brain scanning using CT and MRI in most cases allows one to clearly distinguish a cavernoma from other brain formations, including tumors of varying degrees of malignancy. However, in some cases, differentiation of these formations represents a diagnostic problem, the solution of which requires extensive experience. In this regard, the ability to attract a highly qualified diagnostician is critical. In addition, high-quality interpretation of CT and MRI images provides a solution to other diagnostic problems: exclusion of surrounding cerebral edema, identification of the severity of hemorrhage, description of details affecting the operability of the cavernoma. If you are in doubt about the diagnosis, you should consult a radiologist from a leading center specializing in brain pathology. A second opinion from such a diagnostician can be very valuable in the differential diagnosis of angiomas and other pathological conditions.
Preventive measures
The most common type is congenital cavernoma. Modern medicine is not able to eliminate genetic abnormalities. To avoid problems with the central nervous system, it is recommended to take care of blood vessels:
- monitor blood pressure;
- eat properly and balanced;
- get rid of excess weight and bad habits;
- control cholesterol and blood sugar levels;
- avoid lifting heavy objects;
- dilute a sedentary lifestyle with physical activity and going to the gym;
- avoid stress.
If you experience any problems with your health, in particular periodic headaches and dizziness, disturbances in visual and auditory functions, you should immediately seek medical advice.
You can make an appointment at our clinic using the phone number listed on the website.
Cavernous angiomas on CT
When using visualization methods, it is useful to separate the cavity into 3 components. These include (1) a peripheral pseudocapsule, consisting of glial tissue impregnated with hemosiderin, (2) an irregularly structured intermediate connective tissue separating the cavities, and (3) a central vascular part, consisting of vascular cavities with slow blood flow.
On CT images without contrast enhancement, a cavernoma appears as a focal formation of an oval or nodular shape, characterized by slightly or moderately increased X-ray density and does not have a volumetric effect on the surrounding parenchyma. Areas of calcification and hemosiderin deposition in the walls of fibrous septa, along with stagnation of blood in the cavities, contribute to increased x-ray density on non-contrast-enhanced images. On CT images, calcifications are detected in approximately 33% of all cavernomas. If the formation is old, then it may contain central non-contrasting areas of reduced density, which corresponds to cysts from resorbed hematomas.
Contrast enhancement can be minimal or maximal, although 70-94% of cavernous malformations are weakly or moderately enhanced after intravenous contrast. In most cases, good contrast is the result of increased blood flow in the vascular component of the mass. The heterogeneous “speckled” enhancement is caused by intravascular fibrous septa, and the low-density rim along the periphery is caused by a pseudocapsule of glial tissue surrounding the formation.
Mass effect is not typical for cavernomas, unless they are associated with recent hemorrhage. On CT images without contrast enhancement, cavernomas may not be detected at all. In hemorrhages and the formation of intracerebral hematoma, cavernomas are visualized as areas of focal signal enhancement in the area adjacent to the hematoma.
Any hemorrhage detected on CT in a relatively young patient should be carefully investigated, and cavernous angioma should always be considered as a possible cause. When evaluating a patient with a seizure disorder, cavernous angioma should also be considered as a likely etiological factor, especially if the patient is between 20 and 40 years of age.
Cavernous malformations identified by CT may also include other rare vascular malformations (thrombosis of arteriovenous malformation, capillary telangiectasia), glioma (poorly differentiated astrocytoma or oligodendroglioma), and metastatic melanoma.
Methods of treating the disease
Timely treatment of cavernoma guarantees a positive prognosis. The tumor itself is non-cancerous and not life-threatening. A plan for getting rid of the pathology is developed depending on the location of the formation, the patient’s age, symptoms and the presence of other concomitant diseases. The following treatment methods are used:
- regular monitoring of the course of the disease;
- conservative therapy;
- radiosurgical method;
- surgery to remove cavernoma.
Conservative therapy is effective if the disease is detected before complications occur. Timely treatment with medications guarantees a quick restoration of the patient’s health and a return to a normal, full-fledged lifestyle. In almost 100% of cases, surgical intervention allows you to get rid of the disease forever and with a minimal percentage of postoperative risks. Surgery to remove a cavernoma is guaranteed to relieve epileptic seizures, but there is a risk of repeated hemorrhages. Conservative treatment also maintains the risk of hemorrhages, but does not eliminate epilepsy attacks, which forces the patient to take anticolvulsants throughout his life.
There are contraindications to the operation. The size, shape of the tumor, age and general health of the patient must be taken into account. If the cavernoma is located in a hard-to-reach area, radiosurgery is used to extract it. Complications are also possible after radiosurgery, but, in comparison with radiation therapy, ionizing radiation does not have a negative effect on nearby healthy areas. In addition to the listed methods, laser therapy, diathermocoagulation, sclerotherapy, hormonal therapy and cryotherapy are used to treat vascular malforation and remove cavernomas.
Cavernous angiomas on MRI
Cavernous angiomas represent about 1% of all intracranial vascular lesions and 15% of cerebrovascular malformations. With the development and introduction of MRI, cavernous angiomas have become the most commonly detected vascular malformations of the brain. In early studies on autopsy material, the frequency of their occurrence was 0.02-0.53%. Using MRI, the incidence of formations similar to cavernous hemangiomas was 0.39-0.9%, and the detection of previously unidentified asymptomatic formations using MRI increased their incidence to 0.45-0.9%.
Get an MRI of the brain in St. Petersburg
On MRI, parenchymal cavernous angiomas are represented by a characteristic “popcorn”-type formation, clearly defined, with a smooth border. The internal part is represented by multiple foci of signal of varying intensity, which correspond to hemorrhages at different stages of resolution.
MRI signs of cavernous angioma. Large cavernous angiomas of the right frontal lobe and left occipital lobe on T1-weighted axial section. These two heterogeneous space-occupying lesions have a central mesh structure with alternating areas of high and low signal intensity, surrounded by a hypointense rim of hemosiderin.
A fresh hematoma containing deoxyhemoglobin is isointense on T1-weighted images and significantly hypointense on T2-weighted images. A subacute hematoma containing extracellular methemoglobin is hyperintense on both T1- and T2-weighted images due to the paramagnetic effect exerted by methemoglobin.
Intermediate fibrous elements are characterized by a weakly hypointense signal on T1- and T2-weighted images, since they contain calcifications and hemosiderin. The heterogeneous interior of the mass is surrounded by a hemosiderin rim, which has low intensity on T1-weighted images. The hypointensity of this rim becomes more pronounced, resembling a halo, on T2-weighted and gradient-echo images due to the higher sensitivity of these sequences to changes in the magnetic field.
Axial gradient-echo MR images provide better visualization of large cavernous angiomas in the right frontal and left occipital lobes. The hemosiderin rim appears as a halo due to the increased magnetic susceptibility of hemosiderin.
Smaller cavernomas appear as low-intensity nodules on T1- and T2-weighted images.
Small lesions are better visualized on gradient echo images due to the increased sensitivity to changes in the magnetic field that is inherent in such pulse sequences. It has also been shown that in sequential gradient echo images, small punctate formations are better visualized with longer echo times; these data suggest that such formations contain paramagnetic substances.
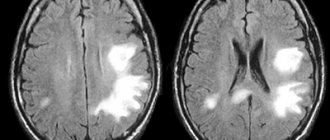
Gradient-echo MR imaging shows multiple bilateral small, punctate and round, low-intensity lesions in the periventricular and subcortical white matter. The largest lesion is visualized in the periventricular white matter of the frontal lobe anterior to the anterior (frontal) horn of the left lateral ventricle near the genu of the corpus callosum. Multiple smaller lesions are visible anterior and posterior to it.
On time-of-flight angiography images, methemoglobin in the center of a cavernous malformation may resemble moving blood. However, on a subsequent phase-contrast MR angiogram obtained with a low blood flow speed setting during encoding (10-20 cm/s), blood flow or pathological vascularization is not visualized, which makes it possible to exclude vascular lesions.
Typically, cavernous angiomas do not have a bulking effect on adjacent tissue or cause edema, and they do not have a feeding artery or draining vein unless they are associated with other similar vascular malformations. Cavernous angiomas are often associated with venous malformations, which are characterized by the presence of a draining vein. In such mixed cases, standard angiography may be useful.
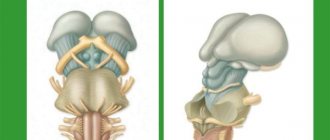
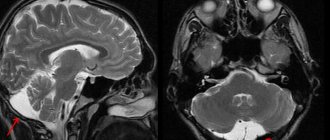
T2-weighted image of a cavernoma of the pons.
Cavernous malformations detected on MRI include other occult vascular malformations (AVM/aneurysm thrombosis, capillary telangiectasia), hemorrhage in a primary or secondary tumor (metastasis of melanoma, choriocarcinoma, thyroid or kidney cancer), amyloid angiopathy, treated or primary infection (toxoplasmosis or cysticercosis), multiple hemorrhages associated with damage to the blood system (disseminated intravascular coagulation, leukemia), as well as the consequences of diffuse axonal damage.