Diffuse brain stem tumor (DSBT) is a neoplasm that represents about 6-8% of cases of known cancers. OSGM accounts for a quarter of a percent of total brain oncology. Unfortunately, the younger generation is also susceptible to this pathology. The real cause of the disease has not been fully determined, and therefore the only chance not to worsen the disease is to recognize the signs that have appeared and begin timely therapy.
What is a brain stem tumor
The structure of the brain stem includes: the base, where the head trunk itself is located, consisting of two substances: gray and white. The trunk itself is small - only 7 centimeters in length. The spinal cord is on one side, and the diencephalon is on the other. Its components: medulla oblongata, pons, midbrain. All nerve nuclei are located in it. There are also centers responsible for: breathing, cardiac function, nerve endings, swallowing, coughing, chewing, salivation, gag reflex. The pons is responsible for the functioning of the eyes, facial muscles, tongue, neck, limbs and torso. Thanks to the work of the nerve nuclei of the medulla oblongata, the work of the muscles of the larynx and pharynx, gastrointestinal tract, hearing and speech of a person is regulated.
Given the importance of the brain stem, any damage or formation entails symptoms that affect health and sometimes life.
2. Symptoms of the disease
Among the main symptoms of tumors of this type are the following:
- astigmatism, nystagmus, violation of facial symmetry;
- headache, dizziness;
- impaired muscle tone on one side of the body;
- unsure gait;
- hand trembling;
- hearing impairment;
- emotional instability.
In severe cases, breathing and heart rhythm disturbances may occur.
Visit our Neurosurgery page
Types of tumors
There are two types of tumors: primary and secondary. Disruptions in brain activity caused by harmful factors will ultimately lead to the chaotic division of damaged cells until they are completely replaced by healthy ones. This is how a primary tumor of the brain stem appears in children and older people. It is based on glial cells. Brain stem cancer can start and develop in one part of the organ. A common place for oncology to appear is the bridge (about 60%). Slightly less - in the midbrain and medulla oblongata. Brain stem tumors occur in the plural.
Secondary are those that appear in one place and continue to grow on the brain stem. Moreover, in only 5% of cases, metastases occur in the trunk, penetrating from other organs. A brain stem tumor is a parastem formation (para – about).
Common types of tumors are gliomas, which develop from glial cells.
- Astrocytomas account for about 60% of diseases. There are multiforme, pilocytic, anaplastic and fibrillary. Benign ones include pilocytic and fibrillary. Pilocytic forms occur in children. Glioblastoma (multiforme) is considered aggressive, which occurs most often in men under 50 years of age.
- Ependymomas account for 5% of all tumors. Most often it is benign.
- Oligodendrogliomas occur in 8% of diseases. Large tumor sizes. There are 4 degrees of malignancy.
Causes and symptoms of gliomas
The nature of the appearance of the neoplasm remains unknown. Experts have only assumptions regarding the reasons for the growth of this type of formation. They may be associated with the influence of unfavorable internal and external factors, and hereditary predisposition.
Glioma is predominantly a primary intracerebral tumor of the hemispheres. It has fuzzy outlines. Experts disagree and cannot say for sure from which cells these neoplasms primarily appear. Many believe that tumor activity is provoked by genetic disorders. The trigger can be unfavorable external and internal factors, including intoxication of the body and radiation exposure.
Symptoms of gliomas
The clinical picture of the disease depends on the severity of the pathological process. Signs of pathology increase gradually. They can be mistaken for a general deterioration in well-being due to overwork and stress.
Symptoms of brain glioma in adults can be focal and cerebral. Dislocation manifestations also occur remotely, which appear as a result of displacement of brain structures and the appearance of local edema.
General cerebral symptoms are characterized by the appearance of headache, nausea and vomiting, seizures, and visual disturbances. They are the first signs of growth of a brain tumor. A headache appears after stress, physical exertion, or a sudden change in body position. At first, the pain syndrome occurs periodically, but as the tumor grows it becomes permanent. Nausea and vomiting are usually not associated with food intake.
Convulsions and visual disturbances occur much later. They appear when the tumor is large enough. Patients note the presence of a constant veil before their eyes. In this case, ophthalmological treatment does not give the expected effect.
Symptoms
When gliomas appear, the destruction of brain stem tissue begins. Depending on the affected area, focal symptoms of the disease appear. Unfortunately, with the appearance of a tumor, other organs also suffer - the tumor, increasing in size, impairs blood circulation and increases intracranial pressure.
Brain stem tumor symptoms to look out for include:
- Headache. 90% of patients complain about it. The tumor puts pressure on the nerve endings, membranes, and blood vessels of the brain. It can appear both locally and be felt throughout the head. The intensity varies - from strong to dull. It occurs suddenly, most often in the morning.
- Nausea, sometimes with vomiting. Appears in the morning.
- Incorrect position. The patient prefers to hold the head in a manner that does not irritate the nerves in the neck and skull.
- Mental disorders. This symptom can be observed both locally and generally. Such disorders include deafness, irritability, and changes in consciousness. The patient feels lethargic, apathetic, does not want to talk, and does not react to anything.
- Epilepsy.
- Decreased visual acuity, which appears due to intracranial pressure. The fundus of the eye changes - the discs swell, their color changes.
- Bulbar syndrome.
- The structure of the skull changes - the seams diverge, its walls become thinner.
Focal symptoms include:
- Damage to motor functions, loss of orientation, tactile and visual perception disappears, gait changes.
- Hearing and sensitivity decrease.
- Paresis and tremors appear.
- Blood pressure surges.
- A facial disorder (distorted smile) appears.
- The clinical picture of brainstem tumors includes delayed onset of intracranial pressure and accumulation of cerebrospinal fluid in the brain (hydrocephalus).
There are many structures in the brain stem that can be affected. When central paresis is affected, tremor appears, dizziness occurs, problems with hearing and vision appear, strabismus may develop, and difficulty swallowing appears. Paresis in the limbs may occur. With the progression of tumor growth, these symptoms increase, and new ones appear - nausea, headache, vomiting. The patient dies due to malfunctions of the cardiac, vascular centers and respiratory organs.
Symptoms of the clinical picture of the disease
The nuclei of the cranial nerves, nerve pathways, centers - all components of the brain stem influence the development of many symptoms of its damage. The compensatory properties of children's nervous tissue provoke a long-term course of the disease in children. The occurrence of a tumor process affects the initial symptoms of the disease; further manifestations depend entirely on the type of tumor.
Probably, the development of main paresis of the facial nerve with a violation of facial symmetry, nystagmus, strabismus, as well as the occurrence of motor coordination disorders, unsteadiness of gait. Symptoms include dizziness, hand tremors, hearing loss, difficulty swallowing and a sore throat. Decreased muscle activity, paresis of the arms, legs or half of the body are added to the main symptoms. In a later period of the disease, symptoms of hydrocephalus appear - headache, nausea, vomiting. The death of the patient occurs due to disorders of cardiovascular functioning and the respiratory center of the brain stem.
Stages of the disease
In medicine, there is a classification of oncological diseases. It is expressed in degrees:
- The first degree is benign. They grow slowly, up to ten years.
- The second degree is borderline.
- The third and fourth are the highest, having an indicator of malignancy. The growth of tumors is rapid - a person with similar degrees can live from a couple of months to several years.
Unfortunately, benign tumors can eventually develop into malignant tumors.
Surgical interventions: technique and results
Planning of access and surgical intervention for removal of cerebral cavernomas generally correspond to the general principles used in surgery of space-occupying brain lesions. In the case of superficial subcortical localization, the search for malformation is greatly facilitated by the presence of post-hemorrhagic changes in the superficial cortex and meninges. The cavernoma, as a rule, is clearly demarcated from the medulla, which simplifies its isolation. If the cavernoma is localized outside functionally important areas, identifying the malformation in the area of perifocal changes and removing it in one block significantly facilitates and speeds up the operation. To improve the outcome of treatment of epilepsy, in some cases, a technique is also used to excise the macroscopically altered brain matter around the cavernoma by blood breakdown products, although information about the effectiveness of this technique is contradictory. Surgeries to remove cavernomas located in functionally significant cortical and subcortical parts of the brain, as well as in deep structures cerebral hemispheres, have a number of features. In case of hemorrhage from a cavernoma of this localization, the patient should be monitored for 2–3 weeks. The absence of regression of focal symptoms during this period provides additional justification for surgical intervention. When making a decision about surgery, you should not wait for the hematoma to resolve, since due to the processes of organization and gliosis, the operation becomes more traumatic. Internal decompression of a cavernoma by evacuation of the hematoma is a necessary step when removing cavernomas from functionally significant areas, as it allows to reduce surgical trauma. Resection of perifocal posthemorrhagic changes is impractical.
| Removal of a small cavernoma using neuronavigation |
To improve the outcomes of cavity removal, various instrumental intraoperative auxiliary techniques are used. In the absence of clear anatomical landmarks, it is advisable to use intraoperative navigation methods. Ultrasound scanning in most cases allows you to visualize the cavity and plan the access trajectory. A significant advantage of the method is the provision of information in real time. Ultrasound imaging of cavernomas can be difficult for small lesions. Frameless neuronavigation based on preoperative MRI data allows for the most accurate planning of access and craniotomy of the required (minimum possible for a given situation) size. It is advisable to use the technique to search for small caverns. Stimulation of the motor area with assessment of the motor response and M-responses should be used in all cases of possible intraoperative damage to the motor cortex or pyramidal tracts. The technique allows you to plan the most gentle access to the cavernoma and evaluate the possibility of excision of the zone of perifocal changes in the medulla. Intraoperative use of ECoG to assess the need for excision of distant foci of epileptiform activity is advisable in patients with a long history of epilepsy and drug-resistant seizures. In the case of epileptic lesions of the medial temporal structures, the technique of amygdalohippocampectomy under ECoG control has shown high effectiveness. For any location of the cavernoma, one should strive for complete removal of the malformation due to the high frequency of repeated hemorrhages from partially removed cavernomas. It is necessary to preserve venous angiomas found in the immediate vicinity of cavernomas, since their excision is associated with the development of disturbances in the venous outflow from the medulla adjacent to the cavernoma. In most cases, cavernomas, even very large ones, can be completely removed, and the outcomes of operations are usually favorable: most patients do not experience neurological disorders. In patients with epileptic seizures, improvement is noted in 75% of cases, and in 62% of cases, seizures do not recur after removal of the cavernoma. The risk of developing postoperative neurological complications depends largely on the location of the formation. The incidence of defects in cavernomas located in functionally insignificant parts of the cerebral hemispheres is 3%. With cortical and subcortical cavernomas of functionally significant areas, this figure increases to 11%. The risk of the appearance or worsening of a neurological deficit in the case of removal of a deep-seated cavity reaches 50%. It should be noted that the neurological defect that occurs after surgery is often reversible. Postoperative mortality is 0.5%.
Causes of pathology
Oncology can occur for various reasons. Doctors call the most common heredity, genetic predisposition, exposure to chemicals, and radiation.
Deviations in genetics include the following syndromes: Turco, Li-Fraumeni, Gorlin, tuberous sclerosis, Von Recklinghausen's disease, Burkitt's tumor.
Unfortunately, medicine has not yet found the exact causes of cancer in humans. Therefore, to date, no remedy has yet been found to help prevent cancer.
Cavernous malformations of the deep parts of the cerebral hemispheres
Removal of a giant cavernous malformation and hematoma of the basal-medial parts of the left frontal lobe, the head of the caudate nucleus and the anterior horn of the left lateral ventricle
Cavernomas of the deep parts of the cerebral hemispheres usually include formations located in the corpus callosum, basal ganglia, thalamus optic, and hypothalamic region. The so-called cavernomas of the lateral ventricles and, in particular, the third ventricle should also be classified as deep. Many deep cavernomas extend to several structures at once. The most characteristic is the spread of cavernomas of the basal ganglia to the internal capsule and insula, cavernomas of the posterior parts of the thalamus opticum into the cerebral peduncle and oral parts of the trunk. Cavernomas of the head of the caudate nucleus and posteromedial parts of the frontal lobe can spread to the hypothalamic region, optic tract and chiasm. Cavernomas of the corpus callosum often protrude into the cingulate gyrus.
Unlike the neocortex, where functionally more or less significant zones can be identified, all deep formations are classified as functionally significant. In this regard, the clinical manifestations of deep CMs and approaches to their surgical treatment differ from those for superficial malformations.
Common to the clinical manifestations of deep cavernomas is the acute or subacute development of focal neurological symptoms due to hemorrhages from these formations. The most characteristic is the subacute development of symptoms with an increase over several days. Depending on the amount of hemorrhage, symptoms may be more or less severe. Often preceded by a period of persistent headache. Typical focal symptoms are contralateral hemiparesis and sensory disturbances, including hypoesthesia, hyperpathy and pain in the extremities. If the dominant hemisphere is damaged, speech disorders may occur. Some patients with cavernomas located near the insula, cingulate gyrus, and mediobasal cortex of the frontal lobe may have epileptic seizures. Cavernomas of the hypothalamic region are often manifested by various endocrine-metabolic disorders. A characteristic symptom of cavernomas of the posterior parts of the visual thalamus, spreading into the midbrain, are oculomotor disorders in the form of dysfunction of the 3rd nerve, and other mesencephalic symptoms. Rare neurological disorders include various extrapyramidal symptoms.
Hemorrhages from deep cavernomas of a medial location, as well as cavernomas of the corpus callosum, can occur with the spread of blood into the ventricular system and subarachnoid space, which is manifested by the development of cerebral and meningeal symptoms. Quite often, hemorrhages from deep cavernomas lead to occlusion of the cerebrospinal fluid pathways. In these cases, intracranial hypertension may be the leading manifestation of the disease.
The dynamics of symptoms after the onset of the disease are varied - from a relatively benign relapsing course with unpredictable intervals, to cases of fairly frequent repeated hemorrhages and a rapid increase in neurological defect as a result of significant damage to brain structures and occlusion of the cerebrospinal fluid pathways. The clinical picture of the disease often depends on the period after hemorrhage. In the acute period of the disease, the condition can be quite severe.
Removal of deep cavernomas, as well as other space-occupying formations of such localization, is a complex task and is associated with a high risk of developing or increasing a neurological defect. In this regard, the indications for surgery differ from the indications for operations for neocortical localization of cavernomas. The general consensus is that surgical intervention is only possible in patients with severe neurological symptoms and frequent recurrent hemorrhages leading to deterioration of the condition. There is no consensus regarding the timing of surgical intervention after hemorrhages that occur with the development of pronounced focal symptoms. Many surgeons indicate that the presence of a hematoma in the acute and subacute period of hemorrhage makes the operation easier. In case of delayed surgery, the latter becomes more traumatic due to the development of adhesions. At the same time, some authors believe that at least one month is necessary to adequately assess the possibilities of neurological recovery.
The peculiarities of operations for cavernomas of this localization include the particular importance of choosing an adequate access, the use of “internal decompression” of the cavernoma in formations containing fairly large hematomas, and the preferable removal of the cavernoma by lumping.
Approaches to deep-lying cavernomas are similar to those that are routinely used to remove tumors of the optic thalamus, subcortical ganglia and other midline structures. Transcallosal access is often used, which makes it possible to remove various neoplasms located in the head of the caudate nucleus, the medial and middle parts of the optic thalamus, and the hypothalamus. Depending on the location of the formation, the transcallosal approach can be homolateral (on the side where the tumor is located) or contralateral. The latter has the advantage that it makes the lateral parts of the thalamus more accessible. With the transcallosal approach, a direct approach to the hypothalamic region, posteromedial parts of the thalamus optica and the midbrain can be carried out through the foramen of Monro, which can be significantly expanded with concomitant hydrocephalus, or through the vascular fissure between the fornix and the optic thalamus. Often a combination of these approaches is necessary. For cavernomas of the posterior parts of the visual thalamus (cushion area) and when the formation spreads into the midbrain, the occipital interhemispheric approach with dissection of the tentorial tentorium lateral to the straight sinus is preferable. For malformations located simultaneously in the midbrain and thalamus optic, subtentorial approaches can also be used - median and lateral, or a combination of different approaches. When the cavernoma is located in the subcortical ganglia, insula, or near the internal capsule, access is used through the Sylvian fissure with dissection of the insular cortex. With such localization of cavernomas, as well as with their location in the basal-medial parts of the frontal lobe (near the chiasmal region), the use of navigation and ultrasound scanning is necessary.
At the initial stages of removal, it is important to empty the accompanying hematomas, which creates additional space that simplifies further removal of the malformation. Cavernoma should be removed by biting, cutting it with scissors or dividing it into fragments using bipolar coagulation. When removing a malformation located near large arteries—the bifurcation of the ICA, MCA, and ACA—special care must be taken not to damage the perforating arteries, which may be included in the structure of the malformation and take part in its blood supply.
The most favorable outcomes are for cavernomas located in the head of the caudate nucleus and in the optic thalamus without spreading to the hypothalamic region and midbrain structures. The least favorable outcomes are the removal of cavernomas of the basal ganglia located under the insula and operated on through the transsylvian-transinsular approach, and malformations of the thalamus opticus extending into the midbrain and hypothalamic region. Removal of the corpus callosum cavernoma is generally not associated with the risk of developing neurological deficits. Taking into account the clinical course and outcomes of the operation, surgical interventions in this localization should be considered justified.
Diagnosis of a brain tumor
In order for the doctor to make a diagnosis, he must first collect an anamnesis. It is very important to answer all questions about symptoms as accurately as possible. If neurological abnormalities are observed, the patient must be sent to a neurologist.
At his appointment, he undergoes an examination and various tests that reveal motor dysfunctions. The doctor will definitely check whether all reflexes are present and whether there is tactile and pain sensitivity. An examination by an ophthalmologist is required, where the patient's fundus is measured. If necessary, the patient is referred to an otoneurologist for a hearing test. After collecting anamnesis, the neurologist will be able to make a diagnosis. If necessary, a neurologist can prescribe CT and MRI, which help detect tumors of minimal size, determine the location of the tumor, and the type.
Additional studies include craniography (x-ray of the skull), which can show whether there is a change in the bones of the skull, encephalography (determining changes in the brain), echoencephaloscopy (ultrasound diagnostics), radioisotope scanning, angiography.
A biopsy is not performed for brain stem cancer. Histology is carried out solely on the basis of data on location, symptoms, and the age of the patient.
Diagnostics
Based on the medical history information obtained by the neurologist and the results of detailed neurological diagnostics, a preliminary diagnosis is established. For confirmation, neuroimaging examinations are used - computed tomography, magnetic resonance imaging, MSCT.
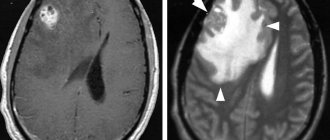
MRI using a contrast solution provides particularly complete and accurate information about the tumor. High-resolution imaging can detect small tumors that are not visible on CT scans.
MRI results suggest determining the histological structure of the tumor, determining in advance the growth pattern, the extent of exophytic growth of the tumor element and the level of infiltration of the medulla. It is necessary to conduct a detailed collection of all data to determine the likelihood and rationality of surgical treatment of the tumor.
Interpretation of MRI examination data reveals the concentration of the tumor, the forms of accumulation of the contrast agent - uniform, uneven, ring-shaped. If the tumor has a diffuse or infiltrative structure, the outlines of the staining do not correspond to the actual size of the pathogenesis.
In T2 mode, the MR signal changes its propagation to areas where the contrast agent has not accumulated. These areas may be an area of swelling of brain tissue, a space for its growth, or both. The simplest neuroectodermal formations are determined by the presence on MRI images of implantation metastases in the ventricular system of the brain, in the subarachnoid spaces.
It is important to differentiate tumor processes in the brain stem from multiple sclerosis, brain stem inflammation, demyelinating encephalomyelitis, ischemic stroke, intracerebral hematoma, and lymphoma.
Treatment
The most effective methods include operations that are aimed at removing tumors.
During the operation, the doctor cuts off the largest part of the formation. To perform the operation, the patient needs to open the skull. In some cases, surgery is not performed on the brain stem, since there is a high probability that vital centers may be affected. The decision on the need for surgery is made based on the size of the tumor and location. The tumor is cut off using endoscopic or laser removal. The laser option cauterizes the edges of the tissue and stops bleeding. The operation is performed using a robotic system, minimizing all kinds of complications.
Radiosurgery is radiation therapy that is based on the use of a single exposure to a high dose of radiation. Used for relapses and metastases.
HIFU therapy, which uses high-intensity ultrasound.
Cryodestruction – freezing with liquid nitrogen. To perform this you need a cryoprobe. The photo below describes the mechanism of action of cryotherapy. The mechanism in the brain is similar.
Treatment of neoplasms
Previously, there was a widespread belief that stem tumors are not subject to surgical treatment due to the fact that they have an infiltrative nature and are capable of diffusely growing into stem elements.
Despite the fact that among all stem structures, most tumors have diffuse germination, sometimes there are delimited nodular formations that are easily removed. Before choosing treatment tactics and deciding on the possibility of surgical intervention, the patient needs to consult a neurosurgeon.
The preferred method of eliminating a brain stem tumor is the maximum possible resection of the tumor with minimal damage to brain structures. Microneurosurgical surgical techniques are developing and provide a chance for a higher level of treatment.
Almost 80% of brain stem tumors are considered inoperable forms. Chemotherapy and radiation treatment are used for inoperable forms, in the preoperative and postoperative period. Cytostatic agents are used in combination form for chemotherapy. 75% of patients receive symptom relief from radiation therapy. The vast majority of cases of the disease end in the death of the patient. Radioisotope treatment can prolong the life of children with similar tumors. The life expectancy of 30% of children who underwent radiotherapy increased by 2 years.
Stereotactic radiosurgery is the newest method for treating brainstem tumors. Two types of radiosurgery can be performed:
- gamma knife - a special helmet is placed on the patient’s head for irradiation from multiple points. The rays converge at one point where the tumor focus is localized. Healthy tissues are practically not affected by this effect. Each beam has a small amount of gamma energy, but the total effect of all beams contributes to achieving maximum effect.
- cyber knife - performed using a robot and is an automated procedure. The device independently concentrates radiation into the area where the tumor is located. The patient's movements and breathing prevent any confusion in aiming the beam of rays.
Studies prove the validity of these methods in the treatment of benign neoplasms up to 3.5 cm in size.
Radiation and chemotherapy
After the operation, radiation therapy is prescribed 14-21 days later. Doctors use radiotherapy (external beam radiation). The course ranges from ten to thirty procedures. Radiation dose – up to 70 Gy. If there are many metastases and malignant astrocytomas, it is necessary to irradiate the head. Radiation dose – up to 50 Gy. This treatment is suitable for inoperable patients who have a diffuse type of oncology.
Chemotherapy is carried out along with education. Treatment for diffuse brainstem tumor is a course of several drugs. The duration of treatment with chemotherapy should be from 1 to 3 weeks. After a break, repeat. During treatment, tests are taken that will show whether chemotherapy needs to be continued or whether it will be cancelled.
Glioblastoma
Chemotherapy for glioblastoma
Drugs for the treatment of glioblastoma and their dose should be selected taking into account the stage of development of the disease, the patient’s age and state of health.
The action of chemotherapy drugs is aimed at the death of malignant tumor cells. For this purpose, temozolimide derivatives are used, which are given the name “Temodal”. International treatment standards include chemotherapy. Chemotherapy is carried out simultaneously with radiation therapy. Usually these are 6-8 cycles, lasting less than 5 days. The effect of chemotherapy occurs only in 20 cases out of 100. In the case of childhood illness, chemotherapy is prescribed instead of radiation treatment, because the latter has a negative effect on the development of the brain at a young age. This type of treatment should be used only after carefully weighing all the pros and cons, taking into account the health status, age of the person, shape and degree of malignancy of the tumor.
The patient will also need supportive care. For this purpose, doctors mainly prescribe Temodal. It should be taken 4 weeks after the end of the course of radiation therapy. Temodal is taken in 6 short courses, each lasting 5 days, with a break between them of at least 23 days. Doctors call this regimen 5/28,” that is, the drug is taken for 5 days of every 28-day cycle.
Avastin is considered a new drug to fight tumors; it has a specific mechanism of action. Avastin was developed by genetic engineers; it is an antibody to a growth factor produced by the vascular endothelium of a malignant neoplasm. This factor is a protein substance that glioblastoma secretes. Therefore, a vascular network is formed in the tumor for its favorable blood supply and development. The larger and more vessels there are, the faster the malignant focus will grow. Avastin is able to block this process of formation of the vascular network, thereby suppressing the development of the tumor. The drug Avastin appeared on the market quite recently. In 2005, publications appeared on the results of its effect on patients with glioblastoma.
Radiation therapy for glioblastoma
This method is used in most cases after surgery to completely remove the malignant tumor. Surgery does not always result in 100% removal of the tumor, because cancer cells can continue to multiply in the lesion. Radiation therapy in a small proportion of cases can replace surgical treatment - when the tumor is inoperable.
Radiation therapy has side effects that occur to a lesser or greater extent. These are fatigue, nausea, hair loss, weakness. Brain tissue may swell, leading to headaches. Necrotic processes are also likely to occur under the influence of radiation. Radiation therapy for the treatment of glioblastoma is aimed at selectively destroying malignant cells without affecting healthy areas of the brain.
Radiation therapy is carried out in several sessions. The irradiation area should cover areas of the brain located on the periphery of the lesion for more effective treatment. You should know that each session destroys not only pathological cells, but also healthy ones. Subsequent treatment stimulates the restoration of healthy tissues, while cancerous ones die.
Glioblastoma can manifest itself in several forms, so the entire irradiation process can include from 10 to 30 treatments, depending on the extent of the process. Radiation therapy increases the likelihood of increasing the life expectancy of every cancer patient.
Radiation therapy is given in fractions of 2 g per day for 5 days. The entire course lasts 6 weeks. The total radiation dose is 60-65 Gy. Such indicators correspond to the norms, while weaker radiation does not give the desired results, and a higher dosage causes undesirable complications. In parallel with radiation therapy, the person is given the drug Temodal - throughout the entire course.
Glioblastoma removal
In some cases, doctors consider glioblastoma not amenable to surgery. But, having a specific location, it can be removed surgically. This prolongs the patient’s life if an integrated approach is taken. It follows from this that chemotherapy and radiation therapy give more desirable results if a person’s glioblastoma is removed first.
As mentioned above, the edges of glioblastoma in some cases are difficult to determine. Therefore, even under a microscope, swollen brain tissue and cancerous tumors cannot always be distinguished. Therefore, a modern method of fluorescent detection of altered cells is used, using 5-aminolevulinic acid.
Preparation begins 4 hours before the start of the operation. The patient is given a special solution with this drug to drink. Then protoporphyrin begins to accumulate in tumor cells. This is necessary so that the contours of glioblastoma become clearer under special lighting. This will allow the neurosurgeon to see the tumor better. Thanks to the wavelength of 375-400 nanometers and the blue light emitted, malignant cells begin to glow.
Not so long ago, it was believed that it was impossible to completely remove glioblastoma, so the cancer cells were partially removed. Nowadays, thanks to the latest developments and modern technologies, glioblastoma can be completely removed.
Treatment of glioblastoma with folk remedies
Glioblastoma, as we have already noted, develops rapidly, with a high percentage of fatal cases due to the disease. But some people still rely on folk remedies for treatment.
One of the recipes is this... Take small radishes and grate them without peeling. Then add salt, mix and leave for 20 minutes to release the juice. The resulting mixture is rubbed into the head, then the head is covered with a warm scarf. A person will feel the heat for about half an hour, then instead of the heat there will be a feeling of warmth. The procedure should be carried out in the evening. In the morning, rinse your head with water (not too hot and not too cold). The next sessions of the procedure should be carried out 3 weeks 1 month after the previous one.
To treat glioblastoma with folk remedies, tinctures and decoctions are used. To prepare a decoction of Siberian cones, take 30-40 g of foliage and flowers and pour 200 ml of boiling water. Then the mixture is infused in a water bath for 30 minutes. The course of treatment includes taking the tincture up to 5 times a day, a third of a glass, for several months.
You can prepare a vinca tincture from fresh herbs, which is filled with alcohol (70%) and infused for 1-2 weeks. The resulting solution is taken 15 drops (strictly!) up to 3 times a day for 2-3 months.
Treatment of glioblastoma in Germany
Treatment of glioblastoma should be comprehensive. In Germany, several methods are used at once. There are known successful cases of treatment at the University Hospital Heidelberg, the RINECKER proton therapy center in Munich and at the university clinics in Düsseldorf and Freiburg.
Radiosurgery, namely cyber-knife and gamma knife, is used in the absence of the possibility of conventional surgery or as an addition to it. Protein therapy, which is used only in German clinics, has proven effective. This type of treatment is considered safer than chemotherapy.
Treatment of glioblastoma in Israel
In Israel, glioblastoma is treated at the Tel Aviv Medical Center, Rabin Clinic and Ishilov Hospital. As in German clinics, these use an integrated approach to treatment. In cases where complete removal is impossible, then partial resection is performed with intraoperative high-dose irradiation of the lesion. To reduce the risk of relapse, Gliadel capsules are widely used, which act as chemotherapy during surgery, acting locally. Systemic chemotherapy is used only for the purpose of relapses and metastases.
New treatments for glioblastoma
German professor Huber determined how to reduce the possibility of regenerative processes and increase the effect of radiation therapy. To do this, you need to block the TGF-β signaling pathways. The latter is considered a growth factor that is produced by the tumor and makes it more aggressive. The drug LY2109761 was developed to block it.
Israeli scientists have also developed new treatment methods. They invented a device with an adjustable electromagnetic field, the spectrum of which selectively kills cancer cells. So far, approval has been received only for the treatment of people with the most common and aggressive forms of brain tumors, including glioblastoma.
Cyber Knife in the treatment of glioblastoma tumors
The duration of therapy for treatment with this new method ranges from 1 to 3 days, one session lasts 30-90 minutes. There is no need to use anesthesia or make incisions, as with standard surgical methods for treating glioblastoma. It is possible to influence several tumors at once. In this case, the person is not hospitalized; immediately after treatment, the patient can live as usual.
CyberKnife is even used to treat those patients for whom the classic version of radiation therapy is contraindicated. If therapy is suspended due to excess
Neurosurgical treatment of glioblastoma tumor
Surgery is indicated to completely remove glioblastoma multiforme, which is the most common and most aggressive form of brain tumor. It accounts for up to 52% of primary brain tumors and up to 20% of all intracranial tumors. The operation significantly prolongs the patient's life. In addition, in the case of tumor removal, the use of radiation therapy and Temodal (an imidazotetrazine alkylating drug with antitumor activity) significantly increases the effectiveness of treatment.
Since the growth of glioblastoma is infiltrative (fast and characteristic of immature, malignant tumors), it is difficult to achieve complete resection. Some areas of the tumor completely merge with healthy edematous tissue. Therefore, even under a microscope it is difficult for a neurosurgeon to accurately determine its boundaries. In order to improve the visualization of a glioblastoma tumor during surgery, a method is used to determine the affected cells using 5-aminolevulinic acid. 4 hours before the start of the operation, the patient needs to drink a solution of the specified drug. In the human body, 5-aminolevulinic acid is converted to protoporphyrin. It, in turn, accumulates in glioblastoma multiforme cells.
Under illumination by a microscope generating blue light waves with a length of 375-400 nanometers, protoporphyrin provokes a fluorescent glow in malignant tumor cells. Thanks to this, the surgeon is able to perform the resection as accurately and efficiently as possible. Using this method, you can completely get rid of the disease glioblastoma multiforme. In the recent past, this was not possible, especially in cases where the tumor was localized in functional areas of the brain. Previously, neurosurgeons left a certain part of the tumor, fearing the risk of complications. Especially such as paralysis, impaired motor function, speech. But using the latest neuronavigation systems, the surgeon in most cases is able to remove glioblastoma multiforme completely.
For example, using a Zeiss Pentero operating microscope, which has fluorescent lighting and is equipped with an integrated module for angiography and resection of glioblastoma multiforme, as well as other hard-to-reach tumors. Only a few clinics around the world have such equipment. This system made it possible to operate on more than forty patients who were diagnosed with glioblastoma at the oncology center. In the case where tumor particles remain in the body after surgery, carmustine or another cytostatic antitumor chemotherapeutic drug is applied to its surface. They gradually spread throughout the remains of glioblastoma, slowly destroying malignant cells.
Maintenance chemotherapy with Temodal
Temodal is prescribed to patients in combination with radiation therapy. It is taken daily throughout the course of radiotherapy. Maintenance therapy with Temodal begins 4 weeks after completion of the course of radiotherapy necessary for the treatment of glioblastoma of the brain. Usually the doctor prescribes 6 short courses of Temodal. The duration of each course is 5 days. Between courses a break of 23 days is required. Thus, the patient receives a dose of the drug in the first 5 days of each 28-day cycle. That is why the Temodal maintenance therapy regimen is called “5/28”.
Maintenance chemotherapy with Avastin
Avastin is a drug that is essentially an antibody to tumor vascular endothelial growth factor. These antibodies are created through the use of genetic engineering. Endothelial growth factor is a protein compound that can be secreted by tumors. Glioblastoma of the brain develops due to the fact that its vessels begin continuous uncontrolled growth. Avastin has the ability to block vascular endothelial growth factor. Thus, it stops the growth of the tumor. Patients gained access to the drug Avastin (Bevacizumab) not so long ago.
Clinical trials in glioblastoma brain
Scientists at Duke University Medical Center (USA, New Carolina) have created a new vaccine. Based on the results of clinical trials, it can be argued that this drug can prolong the life of patients diagnosed with glioblastoma up to 33 months, and in some cases, more.
The studies involved 23 patients who had previously received conventional treatment (surgery, chemotherapy and radiotherapy). Each patient received a monthly injection of the newly created vaccine along with temozolomide (a drug used in chemotherapy). Temozolomide is believed to enhance the effect of the vaccine. And this despite the fact that chemotherapy drugs usually have a suppressive effect on the immune system. The leader of the study, neurosurgeon John Sampson, thus describes the mechanism for treating glioblastoma of the brain. “During the period when the patient’s body is recovering from a course of chemotherapy, immune mechanisms are at their highest activity. This provides the best prerequisites for curing glioblastoma of the brain with the introduction of a vaccine.” The new drug has no side effects, except for swelling of the skin at the injection site. In all patients who took part in clinical trials, the tumor did not increase over 16.6 months. The life of some patients was extended by 4 to 6 years, although this tumor was not treated. American scientists announced the effective result of clinical trials of a new vaccine, with the help of which it became possible to cure a disease such as glioblastoma multiforme of the brain.
The prognosis for patients with glioblastoma of the brain is disappointing. The average survival for patients treated only with surgery is 14 to 26 weeks. Additional radiation extends this period to 40 weeks. Chemotherapy with nitrosourea derivatives (such as procarbazine or carmustine) prolongs life for patients by up to 50 weeks and sometimes up to 18 months. But even in the case of the most favorable prognostic factors, most patients live less than 1 year. Only 15% of patients have a life expectancy of two years.
Death from glioblastoma
Glioblastoma is a terrible cancer that manifests itself with many symptoms. The more the cancer grows and the longer it goes untreated, the worse the symptoms become. Therefore, the last months of a person’s life with a diagnosis of glioblastoma can be extremely difficult.
In the last months of life, there is a constant headache, epileptic seizures and paralysis occur regularly, and mental activity is impaired. A person loses certain functions. Which ones exactly depend on which area of the brain is affected. The patient is constantly weak and feels a lack of strength.
Forecast
Unfortunately, the prognosis is disappointing. Even after a complex of treatment, the survival rate is 60%. If a patient is contraindicated for surgical intervention or has an advanced disease, he or she is less likely to live 5 years (the patient is one of 30-40% of people).
People with the most aggressive forms of cancer live no more than one year. Unfortunately, some survive only a few months. Children, due to their growing bodies, have a better chance of surviving than adults or older people.
People with certain diseases: non-Hodgkin's lymphoma, brain stem cavernoma, sarcoma tumor, HPV, lymphoma tumor, unfortunately, will not be able to live long.
3.Diagnosis of the disease and treatment
Diagnosis of such neoplasms is traditionally made using magnetic resonance imaging (MRI) and computed tomography (CT)
.
In addition, it is also necessary to conduct a histological examination of the tumor
in order to determine its exact type.
When choosing a treatment method
neoplasms, a number of circumstances are taken into account, among which the most significant are the degree of malignancy of the tumor and its size, the degree of proximity of the tumor to vital centers, the age and physical condition of the patient, etc.
The main method of treating trunk tumors is radical surgery.
, however, in some cases it may not be possible if access to the tumor is too risky or difficult for one reason or another.
In addition to surgery, radiation therapy may also be used.
In case of inoperability of the tumor, stereotactic radiosurgery
, which allows the neoplasm to be irradiated with a high dose of ionizing radiation with extreme precision, without causing damage to surrounding healthy tissues.
About our clinic Chistye Prudy metro station Medintercom page!
Cavernous malformations of the cerebellum
Removal of multiple cerebellar cavernomas
Cerebellar cavernomas account for 4–8% of all cavernomas and, as a rule, are localized in the cerebellar hemispheres. Cavernomas of the vermis and cerebellar peduncles are less common.
Clinical symptoms in cavernous malformations of the cerebellum, as in cavernomas of other locations, are caused by hemorrhages from the malformations. Acute or subacute development of the disease in the form of headache, nausea, vomiting in combination with brainstem-cerebellar symptoms is quite typical. General cerebral symptoms are especially characteristic of hemorrhages with blood spreading into the fourth ventricle or with the formation of large hematomas. Focal symptoms of cerebellar cavernomas are most often represented by dizziness, unsteadiness when walking, and loss of coordination in the limbs. Sometimes patients complain of double vision, but it can be quite vague, since, as a rule, it is associated not with damage to the oculomotor nerve system, but with vestibular disorders, which is manifested by the appearance of nystagmus. Symptoms that develop after hemorrhage from the cerebellar cavernoma can completely regress, but often persist for a long time.
Indications for removal of a cerebellar cavernoma should include hemorrhages manifested by severe cerebral and/or focal symptoms, especially repeated ones, as well as a progradient increase in focal symptoms. The formation of large hematomas causing occlusion of the cerebrospinal fluid pathways is an indication for urgent intervention. For large malformations with clinically compensated or subcompensated occlusion of the cerebrospinal fluid pathways, removal of the formation is also preferable.
You should refrain from surgery if the clinical picture is blurred, complete regression of symptoms after a single hemorrhage, especially in patients with cavernomas of the middle peduncle and medial parts of the cerebellar hemisphere, as well as in patients of an older age group and with a burdened somatic history.
The technique for removing cerebellar cavernomas does not have any significant differences from removing cavernomas of other locations. As with the removal of other space-occupying lesions of the cerebellum, performed with the patient in a sitting position, special attention should be paid to the prevention of air embolism. The risk of developing cerebral edema and rapidly developing occlusion of the cerebrospinal fluid pathways, which may be caused by impaired venous outflow, should also be taken into account. In the postoperative period, if necessary, external ventricular drainage should be installed. With cavernomas of a paratrunk location, there is a risk of damage to the vessels supplying the trunk with the development of corresponding complications.
The story of Nadezhda Nikolaevna
Nadezhda Nikolaevna says: “Before the operation, I felt very bad.
There came a time when I couldn’t walk, I stumbled and fell, I was constantly dizzy, my memory was impaired. This state no longer gave me confidence in the future.” The tomogram showed a tumor actively accumulating contrast - most likely a meningioma of the wing of the main bone. By the time the first problems arose, it had grown to impressive proportions. Then neurosurgeon Vladislav Svetlitsky suggested surgical intervention to the woman. Surgery is the main, generally accepted method of treating meningiomas, which gives every chance to be cured once and for all and never have to return to this issue.
This operation was performed jointly by Vladislav Petrovich and Andrey Anatolyevich Oblyvach , a Kiev neurosurgeon, candidate of medical sciences with extensive experience in performing similar interventions.
A little about terms and erroneous conclusions
Patients or their relatives who do not have a medical education sometimes have doubts about the need to remove a tumor node using a radiosurgical unit. This is due to the fact that the medical report does not (and cannot write) “inoperable brain cancer,” but refers to a tumor, neoplasm, area of neoplastic growth, etc. The validity of irradiation of a benign tumor raises especially many questions.
In this case, people are misled by the peculiarities of medical terminology. It must be borne in mind that in the brain tissue there are no epithelial cells that can degenerate and give rise to a true cancerous tumor - carcinoma. That is, brain cancer as such does not exist. But this circumstance does not mean that the detected outbreak is harmless. On the contrary, highly malignant brain tumors are distinguished by extremely aggressive “behavior”, although they are not cancerous.
Moreover, in some cases, benign nodes can cause no less serious problems. For example, if they disrupt blood circulation, they compress the centers of nervous and neurohumoral regulation.
In the neurosurgeon's operating room: work at the microscope
However, the tumor is clearly visible on the screen of a neurosurgical microscope: it was carefully separated from the vessels and removal began. The lining of the meningioma and its cystic part were opened to release the fluid. And then the tumor was removed from the surface of the brain layer by layer using vacuum suction.
From the moment Dr. Svetlitsky cut the skin until the moment the tumor was removed, only two hours passed. Another 1.5 hours were spent on thorough, hermetically sealed suturing of the wound.
Even after completing an operation, surgeons cannot know one hundred percent whether a tumor is malignant or not. Here, modern medicine is still limited, and one has to wait hours and days until a histological examination confirms the diagnosis of “benign meningioma” and it becomes clear that the tumor is over and there is no need for further treatment.