Diencephalic syndrome (hypothalamic) is a complex of endocrine, metabolic, and autonomic disorders.
During these disorders, damage to the hypothalamic region of the diencephalon is observed. In most cases, these disorders occur due to dysfunction of the hypothalamus.
Diencephalic syndrome is characterized by:
- change in body weight, in most cases it increases;
- the appearance of headaches;
- mood problems, frequent changes;
- the appearance of hypertension;
- problems with the menstrual cycle;
- increased appetite;
- a feeling of increased thirst;
- Sometimes sex drive increases and decreases.
This disorder often occurs in endocrinological, gynecological, and neuralgic practice, and during diagnosis difficulties arise that are associated with the variety of symptoms and varieties of the syndrome.
Diencephalic syndrome in most cases occurs in adolescents aged 13 to 15 years, as well as during reproductive age from 31 to 40 years. During reproductive age, it mainly predominates in women - from 12.5% to 17.5%.
The disease leads to serious reproductive health problems for many women. The development of endocrine infertility, the appearance of polycystic ovary syndrome, as well as various obstetric and perinatal pathologies are observed.
Causes and provoking factors
Disturbances in the functioning of the hypothalamus can occur due to a number of reasons and factors:
- the presence of tumors in the brain , which lead to compression of the hypothalamic region;
- traumatic brain injuries , during which direct damage to the hypothalamus occurs;
- state of neurointoxication - substance abuse, drug addiction, alcoholism, harm from industrial activities, the influence of environmental harmful components;
- various disorders of a vascular nature - stroke, osteochondrosis;
- neuroinfections of viral and bacterial types - influenza, malaria, chronic tonsillitis;
- factors with a psychogenic nature - the manifestation of stressful and shock situations, excessive mental stress;
- the period of pregnancy and hormonal changes that are associated with this period;
- chronic diseases that manifest themselves together with elements of the vegetative type - bronchial asthma, hypertension, ulcerative lesions of the stomach and duodenum, obesity.
Treatment
Treatment of both diencephalic crisis and the syndrome itself depends on the identified causes:
- if the cause of the disease is a neuroinfection, then therapy is carried out to cure this infection;
- if the cause is a tumor, then an operation is performed to remove the tumor;
- For this disease, the patient is prescribed a special diet.
As for drug treatment, it is aimed at restoring the normal menstrual cycle when it comes to women, as well as normalizing metabolism.
If the patient consults doctors on time, the likelihood of a complete cure is very high.
Classification and clinical picture
There are a large number of research programs on the study of diencephalic syndrome, according to which a classification of the disorder was created.
Dysfunction of diencephalic structures can be of several types, each of which has its own symptoms and manifestations:
- Diencephalic syndrome with hypothalamic (diencephalic) epilepsy .
- A disorder of a vegetative-visceral-vascular nature . There are disturbances in the cardiovascular and respiratory systems.
- Thermoregulation disorder . There is an increase in body temperature from subfebrile to febrile. With this form, a state of chills, muscle yeast appears, and sometimes hypothermia may appear.
- Neuromuscular type disorders . This form is accompanied by increased weakness in the form of physical asthenia.
- Neurotrophic disorders . This disorder is characterized by the manifestation of increased edema against a background of general weakness, thirst, headaches, chill-like tremor and hypothermia.
- Neuroendocrine form . This disorder manifests itself in the form of hypo- and hyperfunction of the pituitary gland and other endocrine glands.
- Neuropsychiatric disorders . Vegetative-vascular, neuroendocrine, metabolic and trophic disorders are observed.
- Neuroendocrine metabolic disorders . These are endocrine disorders that cause obesity, early puberty, headaches, rapid physical and mental fatigue, menstrual irregularities and other disruptions.
Diencephalic epilepsy
Diencephalic epilepsy is a kind of vegetative paroxysms, similar to attacks of ordinary epilepsy, but caused by disturbances in the functioning of the hypothalamus. They can appear from several hours to days.
This form of the syndrome combines the following symptoms:
- a day before the onset of an attack, a person’s mood may change;
- increased feeling of hunger;
- feeling of thirst;
- manifestation of unreasonable fear;
- After about two hours, a feeling of chills may appear;
- increased body temperature;
- manifestation of heavy sweating;
- skin color may change;
- the occurrence of frequent urination and bowel movements.
Seizures usually occur in conjunction with convulsions and fainting.
NSICU.RU neurosurgical intensive care unit website of the intensive care unit of the N.N. Research Institute Burdenko
Research Institute of Neurosurgery named after N.N. Burdenko, RAMS, Moscow
Introduction
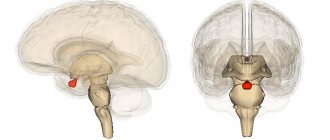
Diencephalic structures (DS) include the thalamus, hypothalamus, epithalamus, subthalamus and pituitary gland [1]. The thalamus, located below the lateral ventricles, is a cluster of nuclei, has an oval shape, forms the lateral wall of the third ventricle and occupies 4/5 of the space of the diencephalic region. The main function of the thalamus is the primary analysis and transmission of information to the cerebral cortex from all sense organs with the exception of the olfactory analyzer. The hypothalamus is a complex of nuclei that form the bottom and side walls of the third ventricle.
There are paraventricular, supraoptic, preoptic, suprachiasmatic, ventromedial, arcuate, mammillary, posterior and other nuclei. The nuclei of the hypothalamus have extensive intracranial connections. The hypothalamus synthesizes peptides - liberins and statins. The hypothalamus is the highest center of endocrine regulation, ensures the constancy of the internal environment of the body, regulates the functioning of organs and systems of the body, coordinates the work of the nervous, endocrine and immune systems. The epithalamus - the pineal body, the leash, its nuclei and commissures, the posterior commissure - form the roof of the third ventricle, to which the choroid plexus is adjacent.
Melatonin is synthesized in the pineal gland. The epithalamus regulates the sleep-wake cycle, takes part in the regulation of emotions and the functioning of the autonomic nervous system. The subthalamus includes the subthalamic nucleus, the rostral parts of the red nucleus and the substantia nigra, is located between the thalamus and the midbrain tegmentum and is involved in the extrapyramidal regulation of movements. The pituitary gland is located in the sella turcica of the sphenoid bone and has two lobes - the anterior (adenohypophysis) and posterior (neurohypophysis). The neurohypophysis is connected to the hypothalamus by the pituitary stalk, which is the axons of the neurons of the nuclei of the hypothalamus and epithalamus and through which vasopressin, oxytocin and melatonin are transported. The anterior lobe of the pituitary gland synthesizes tropic hormones (adrenocorticotropic, thyroid-stimulating, gonadotropic, somatotropic hormones and prolactin), the release of which is regulated by hypothalamic peptides. Liberins and statins enter the adenohypophysis from the hypothalamus through a branched system of arterioles, capillaries and venules. Endocrine regulation is the main function of the pituitary gland.
Syndromes that develop as a result of damage to the DS are described: diencephalic dysthermia (hyperthermia, hypothermia, poikilothermia), hypothalamic obesity, diencephalic syndrome in children, hypothalamic cachexia in adults, anorexia, bulimia, diencephalic glycosuria, acromegaly, Cushing's disease, hypothalamic hypogonadism, pituitary dwarfism, gigantism, syndrome Pradera-Willi and others [2,3]. In neurocritical care patients with traumatic brain injury, signs of damage to the DS are detected in 15-33% of cases [4 – 6]. The range of clinical manifestations that these authors consider to be a consequence of damage to the DS in patients with traumatic brain injury is wide and includes impaired consciousness, dilated pupils, increased intracranial pressure, arterial hypertension, tachycardia, bradycardia or other cardiac arrhythmias, fever, increased muscle tone, opisthotonus, hyperhidrosis, tachypnea. Considering the mechanisms of brain damage during traumatic brain injury, it is difficult to talk about isolated damage to the DS in this category of patients. A number of the above symptoms are a consequence of primary damage to brainstem and subcortical structures or dislocation of the brainstem.
In patients with tumors of the chiasmal-sellar region (CSR) and a complicated course of the postoperative period, the critical condition is caused by isolated damage to the DS. In this case, a characteristic syndrome is formed - diencephalic dysfunction syndrome (DDS).
Purpose of the study
Description of DDS in intensive care patients. In connection with this goal, it was necessary to solve the following tasks: determine the structure of the DDS; identify SDD options; to draw a correlation between the variant of DDS and the outcome of the disease.
Materials and research methods
The study included patients who underwent surgery at the Institute from 2006 to 2009, inclusive. Inclusion criteria were: Age over 18 years; XSO tumor; complicated course of the early (7 days) postoperative period; the patient's stay in the intensive care unit for more than 48 hours. Exclusion criteria were: patient stay in the intensive care unit for less than 48 hours; intracranial complications not associated with damage to diencephalic structures (meningeal hematomas, intracerebral hematomas at a distance from the bed of the removed tumor, ischemic brain damage in the basin of the great vessels of the brain); atonic coma that developed within 7 days after surgery; pulmonary embolism and acute myocardial infarction that developed within 7 days after surgery; sepsis that developed within 7 days after surgery. Manifestations of multiple organ dysfunction were recorded. For this purpose, the criteria of the SOFA scale were used [7]. The exceptions were the classification of altered consciousness (AC) and dysfunction of the respiratory system. Consciousness was assessed using the RASS scale (Table 1).
The RASS scale was chosen because the patient population studied develops both depression of consciousness and psychomotor agitation. Under these conditions, the use of other generally accepted scales assessing the level of consciousness, including the Glasgow Coma Scale, did not cover all changes in consciousness characteristic of patients with CSO tumors during a complicated postoperative period. The absence of IS corresponded to a RASS score of 0; with any other RASS score, consciousness was considered altered.
The criteria for dysfunction of the respiratory system were a decrease in the pO2/FiO2 index below 400, as in the SOFA scale, and the need for prolonged mechanical ventilation (more than 24 hours after surgery). This is due to the fact that the cause of respiratory dysfunction in neurocritical care patients is not only parenchymal damage to the lungs, which reflects the pO2/FiO2 index, but also other mechanisms, for example, disruption of the central mechanisms of respiratory regulation or depression of consciousness [8]. Other somatic organ dysfunctions (SOD) were classified strictly according to the SOFA scale. Cardiovascular system dysfunction was defined as the development of arterial hypotension (a decrease in mean blood pressure below 70 mmHg) or the need to use sympathomimetic drugs. Renal dysfunction was defined as an increase in creatinine levels above 110 μmol/L or a decrease in urine output less than 500 ml/day. Hepatic dysfunction was defined as an increase in bilirubin levels above 20 μmol/L. Hematological dysfunction was defined as thrombocytopenia (less than 150 thousand/μl).
Fluid-electrolyte disturbances (WED) and intestinal dysfunction often develop in patients with CSO tumors and a complicated course of the postoperative period. The SOFA scale does not include assessment of these disorders, so the following criteria were introduced to qualify them. VEN was defined as dysnatremia (increase above 145 mmol/L or decrease below 135 mmol/L) due to diabetes insipidus, syndrome of inappropriate vasopressin secretion, or salt-wasting syndrome. Intestinal dysfunction was defined as gastrointestinal paresis. Fever was defined as an increase in body temperature above 38.5ºC, hypothermia - a decrease in body temperature below 36ºC. To prevent the development of hormonal deficiency, all patients after surgery received hormone replacement therapy at a dose that is used in patients with hormonal deficiency who are in a state of severe stress: hydrocortisone 2.5 - 3 mg/kg/day, L-thyroxine 2-2.5 mcg/kg/day Data are presented as medians with 25th and 75th percentiles indicated. The Mann-Whitney test and risk ratio were used in data analysis. Differences were considered significant at p<0.05, and the risk was considered significant if the lower limit of the confidence interval exceeded one. Statistical analysis was carried out using the Statistica 7.0 program.
Research results and discussion
According to the inclusion criteria, 83 patients were included in the study. 7 patients were excluded from the analysis in accordance with the above criteria: 2 patients with epidural hematoma, 3 patients with the formation of atonic coma within 48 hours, 1 patient with acute myocardial infarction and 1 with PE. Thus, 76 patients with a complicated course of the early postoperative period aged from 19 to 77 years (median 49 years) were analyzed.
There were 43 (56.6%) women, 33 (43.4%) men. 46 patients had a pituitary adenoma, 17 had a craniopharyngioma, 8 cases had meningioma in the CSR, and one observation each included patients with glioma and ependymoma of the third ventricle, hemangiopericytoma, epidermoid cyst, and cancer metastasis in the CSR.
All 76 patients (100%) had IS and dysnatremia, developing, respectively, on the first and second days after surgery (Table No. 2).
Taking into account the anatomy and physiology of the DS, this is logical. Since vasopressin is synthesized in the paraventricular and supraoptic nuclei, deposited in the neurohypophysis, and transported there along the pituitary stalk, there is a high probability of perioperative damage to any one or more of these anatomical structures. This immediately leads to dysnatremia. IP is also easy to explain. The thalamus, which occupies 4/5 of the DS, isolates important information coming from all sensory analyzers and transmits only it to the cerebral cortex. When this limiting mechanism is damaged, the cortex receives a huge amount of unnecessary information, which it is not able to analyze, and an obvious overload occurs, leading to a change in consciousness [9]. The epithalamus synthesizes melatonin, which is then deposited in the neurohypophysis. Melatonin is of paramount importance for the adequate functioning of the circadian sleep-wake rhythm. When the epithalamus, pituitary stalk or pituitary gland are damaged, sleep disturbances develop, which lead to changes in consciousness [10]. In addition, various DS are associated with stem structures, the limbic system, and the cerebral cortex. Morphological damage to these connections can also cause IS [11].
Dysfunction of the respiratory and cardiovascular systems and water and electrolyte disturbances developed on the second day after surgery, and paresis of the gastrointestinal tract - on the third. The most common SODs were cardiovascular dysfunction, intestinal dysfunction, and respiratory dysfunction. Dysfunction of the cardiovascular and respiratory systems developed on the second day, respectively, in 52 (68%) and 50 (66%) patients. Intestinal failure developed on the third day in 51 (67%) patients. The cardiovascular, respiratory systems and gastrointestinal tract are those structures on which DS have a pronounced and direct effect. Based on this, the frequent development of these SODs in patients with a complicated course of the postoperative period is logical. Thrombocytopenia developed much less frequently and later – in 21 (28%) patients from 4 days after surgery. This is because platelet levels are regulated by other mechanisms. Renal and hepatic dysfunction developed in the early stages after surgery, but were detected very rarely - in three (4%) and one (1%) cases, respectively. DS do not directly regulate glomerular filtration, so they cannot have a direct effect on creatinine clearance [12]. In diabetes insipidus, renal failure develops only with the development of decompensated hypovolemia, which can be easily avoided with adequate infusion and hormone replacement therapy with vasopressin preparations. In addition, renal failure can develop as a result of resistant arterial hypotension, which occurs extremely rarely in the studied group of patients [13]. DS probably also lack a direct regulatory effect on liver function, which, however, may suffer due to hypoperfusion due to resistant arterial hypotension. Another possible cause of the development of renal and liver failure may be abdominal compartment syndrome, which develops as a result of paresis of the gastrointestinal tract [14]. However, resistant arterial hypotension and compartment syndrome develop quite rarely [13], which is reflected in the frequency of these dysfunctions in the studied category of patients.
Fever developed in 18 (23.7%) patients; hypothermia was not detected in any of the observations. Thus, dysthermia, previously described as a symptom characteristic of damage to the DS, rarely developed in our patients.
When the DS is damaged, dysfunction of the adrenal glands and thyroid gland is inevitable. Clinical manifestations of adrenal and thyroid insufficiency are arterial hypotension, brady- or tachycardia, hypothermia or fever, paresis of the gastrointestinal tract, increased membrane permeability, leading to polyserositis and interstitial edema [2,15]. In accordance with accepted intensive care protocols, all patients included in the study received glucocorticosteroid and thyroid hormones in doses that completely replaced their production by the adrenal glands and thyroid gland under conditions of severe stress. It follows from this that we could exclude adrenal and thyroid insufficiency from among the causes of the development of the above organ disorders.
It is obvious that if the posterior lobe of the pituitary gland or its stalk is damaged, VEN will inevitably appear [2]. In which type of damage to the DS the patient will obligately develop IS and SOD still remains unknown. The analysis also failed to answer this question. This means that accurate preoperative and intraoperative predictors of the development of IS and SOD are still lacking.
It should be emphasized that before the operation, all patients included in the study were in a compensated state, and they had no manifestations of somatic organ dysfunction, and VEN were less pronounced or completely absent. Thus, when describing the structure of postoperative DDS, dysnatremia, IS and SOD that developed after surgery should be taken into account. To determine the variants of DDD, patients were divided into groups depending on the combination of identified dysfunctions. There were 6 groups (Table No. 3).
Note. Gr – group; IS – altered consciousness; VEN – water and electrolyte disturbances; SD – somatic dysfunction; ICU – intensive care unit; GOS – Glasgow Outcome Scale; DS – diencephalic structures; SS – stem structures; PE – pulmonary embolism.
Group 1 consisted of 12 patients. They showed an isolated combination of IS and VEN without SOD. The median age of these patients was 42.5 years, the median length of stay in the ICU was 8.5 days. In 11 (91.7%) patients, according to the Glasgow Outcome Scale (GOS), a favorable outcome was recorded (GOS=4), one patient (8.3%) had an unfavorable outcome (GOS=3), there were no deaths.
Group 2 consisted of 11 patients. They had one SOD in addition to IS and dysnatremia. Most often, 6 (54.5%) patients developed dysfunction of the cardiovascular system. Intestinal paresis developed in two patients, and respiratory failure developed in two cases. In one observation, thrombocytopenia was detected. The median age was 51 years, and the median length of stay in the ICU was 13 days. A favorable outcome (GOS=4) was in 5 (45.5%) patients, an unfavorable outcome (GOS=3) was in 6 patients (54.5%).
Group 3 consisted of 12 patients. They had two SODs against the background of IS and dysnatremia. Intestinal failure developed in 9 (75%) patients, respiratory failure - in 8 (66.7%) patients, cardiovascular failure - in 7 (58.3%) cases. The median age in this group was 47 years, and the median length of stay of patients in the ICU was 23.5 days. 3 (25%) patients had a favorable outcome: GOS = 4 in two observations; GIS=5 in one observation. 9 patients (75%) had an unfavorable outcome. Of these, 5 patients developed severe disability (GOS = 3), and in 4 cases (33%) a fatal outcome was recorded (GOS = 1). The cause of death in 3 cases was sepsis, in one case it was PE.
Group 4 consisted of 25 patients. They had three SODs in addition to IS and dysnatremia. Respiratory failure developed in 24 (96%) cases, cardiovascular failure - in 23 (92%) patients, intestinal failure - in 24 (96%) patients. Thrombocytopenia was noted in 4 (16%) patients. The median age in this group was 53 years, the median length of stay in the ICU was 22 days. A favorable outcome was observed in 6 (24%) patients: GOS = 5 in two patients, GOS = 4 in four patients, unfavorable outcome in 19 patients (76%), of which 8 developed profound disability (GOS = 3). Death occurred in 11 patients (44%). In 4 patients who died, the cause of death was sepsis, in 2 – meningoencephalitis, in another 2 – hemotamponade of the ventricular system, dislocation and herniation, 2 patients died due to confirmed morphological damage to diencephalic structures, and 1 – due to PE.
Group 5 consisted of 12 patients. They were simultaneously diagnosed with four SODs with IS and dysnatremia. All patients developed respiratory, cardiovascular, intestinal failure and thrombocytopenia. The median age in this group was 57.5 years, the median length of stay in the ICU was 40.5 days. A favorable outcome (GOS=4) was recorded in 4 (33.3%) patients in this group. An unfavorable outcome developed in 8 (66.7) cases. However, only one of the 8 patients with an unfavorable outcome survived (ORG=3). The remaining 7 (58.3%) patients had a fatal outcome (GOS=1). In 5 observations, the cause of death was sepsis, in 2 observations – damage to diencephalic structures.
Group 6 consisted of 4 patients. They simultaneously developed 5 SOD with IS and dysnatremia. All patients developed respiratory, cardiovascular, intestinal failure and thrombocytopenia. In 3 patients, renal dysfunction was detected, and in one observation, hepatic dysfunction. The median age in this group was 52 years, the median length of stay in the ICU was 7.5 days. There were no patients in this group with a favorable outcome; in all observations, death occurred. The cause of death in one patient was sepsis, in three – morphologically confirmed damage to diencephalic and structures.
The outcomes of patients in the first group with an isolated combination of IS and dysnatremia were better than in all other groups. Their duration of stay in the ICU was the shortest. The differences between the first and second groups were not significant (p=0.5). However, significant differences were obtained in the length of stay of patients in the ICU between the first and third, first and fourth groups (p = 0.04 and p = 0.01, respectively). The analysis did not take into account the length of stay in the ICU of patients in group 5, since these were the most severe patients in whom death occurred early after surgery. Favorable outcomes in group 1 developed more often than in other groups, and unfavorable ones - less often (Table No. 3). The risks of developing unfavorable and fatal outcomes in groups 2 – 6, compared with the first group, are shown in Table No. 4.
There were no deaths in groups 2 and 3, and in group 6 all patients had a death, so it was impossible to calculate risks in these groups.
It is known that a number of patients with isolated dysnatremia, isolated IS, or even a combination of IS and dysnatremia do not require ICU stay in the postoperative period [16]. In some patients, these disorders may persist for a long time after they are discharged from the hospital, and adequately selected therapy allows patients to return to their daily activities.
Obviously, patients in group 1 had more severe forms of IS and dysnatremia than patients with similar disorders, but who did not require a stay in the ICU. Compared with the latter, the distinguishing feature of patients in group 1 was their instability. This was manifested by the need to change the intensive therapy during the day. However, the fact that the same manifestations can occur both in intensive care patients and in those who have already returned to their daily activities does not allow us to distinguish the isolated combination of IS and dysnatremia into one of the forms of DDS.
In group 2, the number of unfavorable outcomes significantly exceeded the number of favorable ones (Table No. 3). This gives grounds to consider patients in group 2 as patients of the first stage of DDS. Therefore, DDS is a syndrome that includes altered consciousness, dysnatremia, and at least one somatic organ dysfunction. The outcomes of patients in each subsequent group were more severe than the outcomes of patients in the previous group (Table No. 4). The risk of developing an unfavorable outcome compared to the first group was higher in each subsequent group: 13.2; 33; 34.8, respectively (Table No. 4). The lower limit of the confidence interval exceeded one in all groups, which indicates the reliability of the identified risk. It is not clear why the risk of developing an unfavorable outcome in group 5 compared to group 1 was 22, while in groups 3 and 4 it was 33 and 34.8, respectively. However, in this group the risk of developing a lethal outcome compared to the first group was significantly higher, and for group 4 the risk of developing a lethal outcome compared to the first group did not reach a significant level (Table No. 4). It follows from this that SDD has 5 degrees of severity. Stage 1 DDS has IS, dysnatremia and one SOD. At each subsequent degree, one SOD is added.
DDS is essentially a variant of multiple organ dysfunction syndrome (MODS). However, unlike SOD, which develops against the background of systemic inflammatory response syndrome, SDS has a number of fundamental differences. First, DDS necessarily includes IS and dysnatremia, which do not always develop in SPOD [17]. Secondly, renal and hepatic dysfunction, typical of DSOD, is not typical for DDS [18]. Thirdly, a significant difference is the timing and order of development of SOD. With DDD, early and virtually simultaneous development of respiratory, cardiovascular and intestinal dysfunction occurs within 1–3 days. Even renal dysfunction, which is not typical for DDD, developed within a day and a half after the operation. SOD is characterized by a slower and gradual emergence of SOD [19]. Fourth, thrombocytopenia has different prognostic significance for DDS and SPOD. In our study, it was detected in 21 patients, which is significantly more common than renal or hepatic failure, but significantly less common than cardiovascular, respiratory or intestinal dysfunction. This does not provide a basis for judging whether thrombocytopenia is a typical or atypical phenomenon in patients with DDS. While thrombocytopenia is typical for SPOD [17,18]. We found no differences in the frequency of its occurrence in different groups. In other words, if the appearance of any other organ dysfunction means a worsening of the patient's condition and a worsening of his prognosis, then the detection of thrombocytopenia meant little to the outcome. However, the most important fact is that in none of our observations did thrombocytopenia reach a level of 50 thousand per µl, and almost always the platelet count exceeded 100 thousand per µl. This meant that thrombocytopenia in DDS does not require correction, unlike SPOD.
conclusions
- In patients with neurosurgical pathology CSO, diencephalic dysfunction syndrome in the postoperative period is manifested by a combination of altered consciousness, water and electrolyte disturbances in the form of dysnatremia and at least one somatic organ dysfunction.
- The presence of altered consciousness and dysnatremia in a patient is not sufficient to diagnose diencephalic dysfunction syndrome.
- The severity of diencephalic dysfunction syndrome and outcome are determined by the number of somatic organ dysfunctions that have developed.
Literature
- Beer M, Frotscher M. Topical diagnosis in neurology according to Peter Duus. Anatomy, physiology, clinic. Per. from English edited by BEHIND. Suslina. 4th ed. M: Practical Medicine, 2009. 478 pp.
- Endocrinology. DeGroot LJ, Jameson JL Elsevier Saunders, Philadelphia, 2006. p. 3336.
- Russell A. Diencephalic syndrome of emaciation in infancy and childhood. // Arch Dis Child, 1951. V.26 p274.
- Baguley IJ, Heriseanu RE, Cameron ID, et al. A critical review of the pathophysiology of dysautonomia following traumatic brain injury. // Neurocrit Care. 2008. V. 8 p. 293-300.
- Boeve BF, Wijdicks EF, Benarroch EE Paroxysmal sympathetic storms (“diencephalic seizures”) after severe diffuse axonal head injury. // Mayo Clin. Proc. 1998. V. 73 p. 148-152.
- Clifton GL, Robertson CS, Kyper K. Cardiovascular response to severe head injury. // J Neurosurg. 1983. V. 59 p. 447-54.
- Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the European society of intensive care medicine.// Intensive Care Med. 1996. V. 22 p. 707-710.
- Popugaev K.A., Savin I.A., Goryachev A.S. and others. Scale for assessing the severity of respiratory failure in neurosurgical patients. // Anest. i rek., 2010. No. 4 p. 42-50.
- Stewart JT, Quijije N., Sheyner I., Stover KT Delirium without focal signs related to a thalamic stroke.// J. Am. Geriatr. Soc. 2010. V. 58 p. 2433-2434.
- Figueroa-Ramos MI, Arroyo-Novoa CM, Lee KA, et al. Sleep and delirium in ICU patients: a review of mechanisms and manifestations.// Intensive Care Med. 2009. V. 35 p. 781–795.
- Frontera JA Delirium and sedation in the ICU.// Neurocrit Care 2011. V. 14 p. 463-474.
- Legrand M., Payen D. Understanding urine output in critically ill patients. // Ann Intensive Care. 2011. V. 24 p.13.
- Popugaev KA, Savin IA, Goriachev AS, Kadashev BA Hypothalamic injury as a cause of refractory hypotension after sellar region tumor surgery.// Neurocrit Care. 2008. V. 8 p. 366-373.
- Cheatham ML: Intra-abdominal hypertension and abdominal compartment syndrome.// New Horiz. 1999. V. 7 p. 96–115.
- Popugaev K.A., Savin I.A., Goryachev A.S. and others. Secondary abdominal compartment syndrome in the complicated course of the postoperative period in patients with tumors of the chiasmal-sellar localization. // Anest. i rek., 2011. No. 4 p. 37-42.
- Pituitary adenomas: clinical picture, diagnosis, treatment / Ed. B.A. Kadasheva. M.-Tver: Triada Publishing House LLC, 2007. 368 p.
- Knaus WA and Wagner DP Multiple systems organ failure: epidemiology and prognosis.// Crit. Care Clin. 1989. V. 5 p. 221–232.
- Cerra FB Multiple organ failure syndrome./ In: Bihari DS, Cerra FB (eds). New Horizons. Multiple Organ Failure. Fullerton, CA: Society of Critical Care Medicine. 1989. p 1–24.
- Murray MJ, Coursin DB Multiple Organ Dysfunction Syndrome.// Yale J. Biol. Med. 1993. V. 66 p.501-510.
Making a diagnosis is not easy
During the polymorphic diagnosis of diencephalic syndrome, difficulties may arise when examining the patient. In order to make a diagnosis, the following studies are carried out and the following tests are taken:
- conducting a sugar curve;
- thermometry results in three places;
- EEG;
- A three-day Zimnitsky test is taken.
The fasting glucose level is determined with a sugar load level of 100 grams. In this case, the glucose level is determined every half hour.
A number of varieties of the sugar curve are defined:
- hyperglycemic type , when the glucose level exceeds the normal level;
- hypoglycemic type , when the glucose level is below normal levels;
- double-hump type , when the drop in glucose changes with a new increase;
- torpid type, when a small jump in blood glucose levels stops at the same level.
Thermometry is done in three zones - in two axillary places and in the rectal area. Various disorders of a thermometric nature can manifest themselves in the form of isothermia, when the temperature in the axillary region and in the rectum are equal, while the level of temperature in the rectum should be 0.5-1 degrees Celsius higher.
And also in the form of hypo- and hyperthermia (in the armpit area the temperature regime is higher or lower than normal), thermoinversion, when the temperature regime in the rectal area is lower than the temperature regime in the axillary zone.
During an electroencephalographic study, problems that relate to the deep structure of the brain can be identified.
When taking a three-day Zimnitsky test, studies are done that help determine the level of fluid consumed and excreted.
In addition, an MRI of the brain is done, which helps to determine high intracranial pressure, as well as various consequences of traumatic injuries, hypoxia, and tumor-type formations.
Studies are carried out to determine the level of hormones in the blood and determine the biochemical data of the blood composition, this is necessary to determine endocrine and metabolic disorders.
A number of studies are mandatory to determine a syndrome of organic origin:
- Ultrasound of the adrenal glands;
- Ultrasound of the thyroid gland and internal organs;
- MRI and CT scan of the adrenal glands.
Diagnostics
A feature of this disease, as we noted above, is the difficulty of diagnosis. To conduct research, the patient must contact both an endocrinologist and a gynecologist, if the case concerns a woman. Diagnostic studies in this case include:
- blood and urine tests that are taken to evaluate ACTH levels, as well as corticosteroid levels;
- special samples that are taken when dexamethasone is used;
- tomography, which is performed to verify the presence or absence of a tumor on the adrenal glands or pituitary gland;
- hormonal studies.
Classification of vascular crises
The term vascular crisis combines two pathologies:
- Hyperkinetic type of crisis, characterized by vasospasm and increased pressure without increasing the volume of circulating blood;
- Hypokinetic (water-salt) is characterized by a simultaneous increase in pressure and the formation of edema in areas of the body. In this case, the increase in pressure is accompanied by an increase in blood volume in the vessels, which lose the tone of their walls and become more permeable.
According to the prevalence of hemodynamic disorders, vascular crises are divided into:
- systemic (hypertensive, hypotonic, vegetative crises);
- regional (migraine, angioedema, angiotrophoneurosis).
Systemic crises occur when the total capacity of the peripheral veins is impaired or the peripheral resistance of blood flow is changed. This may cause a drop or increase in blood pressure. In addition, in such conditions there are signs of secondary cardiac dysfunction. With a sharp increase in pressure, a hypertensive crisis will occur; with a decrease in pressure, a vascular collapse or hypotonic crisis will occur.
Regional crises occur when the blood supply to a tissue or organ is disrupted. Here, with high blood pressure, there may be a significant reduction in blood flow to the organ or even its cessation. With arterial hypotension, on the contrary, the blood flow to the organ is exceeded. With low pressure in the veins and disruption of vascular tone in them, the outflow of blood from organs and tissues is disrupted. In this case, blood stagnates in the veins and capillaries. Diseases such as Raynaud's disease (ischemia of the fingers), migraine (sharp pain in any part of the head), hypertension (cerebral crises) are directly associated with regional blood flow disorders.