People with Moebius syndrome are unable to express emotions. The disease completely deprives a person of facial expressions, and he cannot demonstrate his condition - laugh, cry or even blink. For the first time in 1888, the disease was studied by the neurologist P. J. Mobius, after whom the disease was named. The causes of congenital pathology are still not fully understood, and treatment options are limited.
The main thing about the syndrome
This is a rare, poorly studied disease. It is detected in one in 30,000 newborns. It was first described in the 19th century and has since been systematically studied, but the causes of the disease have not yet been fully identified.
In addition, even in the 21st century, the pathology is difficult to treat, even if it is started in a timely manner. A child with such a disease looks emotionless - due to improper development of the cranial nerves, he is incapable of facial reactions.
He expresses his feelings with sound, for example, crying, but without a characteristic grimace. Such crying (or laughter, in case of pleasure) sounds unnatural, because it is difficult for the baby to control the vocal apparatus.
Today, the cause of the disease is usually listed as paralysis of the facial nerves, although it can also be associated with other processes in the body, such as a lack of oxygen inside the womb.
Trainings to improve communication skills
Thanks to special trainings organized by Danish professors, people suffering from Mobius syndrome improve their social communication skills. The goal of the training is to activate paralinguistic means of communication using intonation and various gestures.
The effectiveness of the classes has been repeatedly proven by experiments and observations; during the dialogue, patients stop feeling nervous, do not fuss and become more relaxed. According to the results of the patients themselves, many do not feel any improvement.
The project's co-author is Kathleen Bogar, who was diagnosed with Mobius syndrome. Having built a career and become a successful doctor, her main goal in her work is to develop a program that will help people suffering from Mobius syndrome adapt to society.
Anatomy of cranial nerves
There are twelve pairs of cranial nerves, of which the first two arise from the brain, the rest from the trunk. Nerves are either sensory, that is, they carry sensations to the brain. Motor – control muscle movements, or mixed, both sensory and motor.
They innervate the head and neck region, with the exception of the tenth (vagus) nerve and several fibers of the 11th, which supply the chest and abdomen.
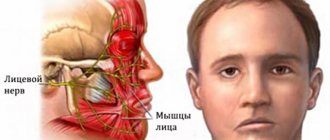
The VI cranial nerve is a motor nerve and innervates the lateral rectus muscle, which causes the eyeball to move laterally, that is, to the outer corners of the eyes. VII - mixed nerve, carries both sensory and motor impulses. The sensory part carries taste sensations from the outer 2/3 of the tongue, the soft and hard palate, which form the roof of the mouth, to the brain. The motor portion of the facial nerve controls the muscles of the face.
When the facial muscles contract, various emotions are visible on the face, such as a smile or forehead wrinkles. In addition, the facial nerve carries parasympathetic nerve fibers that control the secretion of saliva, mucous glands of the mouth and nose, and the secretion of the lacrimal gland.
Based on the extent of the disease, the disorder can be classified as:
- Moebius syndrome in children - VII and VI nerves are completely paralyzed on both sides;
- Incomplete syndrome - here some movements are present on one side of the face;
- Mobius-like forms - one side of the face is paralyzed, other cranial nerves are working.
The exact cause of Mobius syndrome is unknown. There are genetic and environmental factors.
How to check for Mobius syndrome?
Facial amyia is diagnosed during a detailed examination, which necessarily includes the following points:
- Appointment with a neurologist for examination.
If the disease is present, the doctor diagnoses facial paralysis, swallowing dysfunction and tongue atrophy. If there is a pathology of the trigeminal nerve, then hypoesthesia of the skin on the face is added to the list. Disturbances are observed on both parts of the face. - Möbius syndrome in adults requires an MRI of the brain.
Using this diagnosis, the presence of hypoplasia of the cranial nerves is revealed. MRI allows you to exclude or confirm the presence of congenital cysts, tumors, malformations of the meninges and hematomas. The procedure is not recommended for children. - Neuropsychological examination.
In young children, visual reactions and psychomotor function are checked for compliance with age standards. Appropriate tests are carried out with older children. - Appointment with a geneticist.
Moebius syndrome (the photo shows deviations from the norm) is clearly visualized during the examination, but it is important to consult a geneticist to draw up a detailed picture of the disease. The specialist draws up a family tree and identifies the type of inheritance of the disease.
Congenital anomalies
Bone and muscle abnormalities of the arms and legs. Club feet, missing fingers, short fingers or even a split hand. Club feet, where the feet turn inward at the ankles, are one of the most common bone deformities.
The breasts on one side of the body may be underdeveloped. Muscle tone is weak.
A child may have a small chin, a condition called micrognathia. Teeth may be missing or misaligned. The mouth is small with a short or unusually shaped tongue. The palate is high, arched or cleft.
These features add problems with speech development and feeding. The outer ear may be absent or underdeveloped. Hearing loss occurs if the VIII nerve is affected.
Symptoms in a newborn
Moebius syndrome is a hereditary pathology, the type of inheritance is autosomal recessive or, less commonly, dominant. With the syndrome, while still in the maternity hospital, the mother notices that the child’s facial expressions are unnatural, he does not cry or close his eyes, sometimes even at night. Such children also have abnormal defects:
- absence or fusion of fingers;
- deformation of the ears;
- epicanthus.
Although the specific causes of the disease have not yet been established, doctors suggest that taking medications and drugs during pregnancy increases the risk of pathology. Mobius syndrome in children cannot be completely cured, although its manifestations become milder with age.
Symptoms
Patients with Marden-Walker syndrome have a variety of facial features, including abnormalities in the jaw, drooping eyelids, a flat bridge of the nose, low ears, and a fixed facial expression. Other manifestations of this disorder include curvature of the spine resulting in a hump, joint contractures, cleft or high arched palate, delayed growth and slow muscle movement.
Other symptoms of Marden-Walker syndrome may include a small head circumference, heart abnormalities, abnormalities in the urinary system, decreased bone mass, abnormally small eyes, a short neck, a small mouth, and/or a low hairline. A small number of patients with this condition may also have additional tissue causing small intestinal obstruction, a narrowing of the ring separating the stomach from the first part of the small intestine that causes a blockage in the flow of partially digested food (pyloric stenosis); and/or loss of appetite, inability of the body to absorb nutrients properly, stomach pain and weight loss.
The disease is in the nature of a neurological disorder when the child is unable to move the facial muscles and eyes from side to side. This symptom is the main one in the nature of the disease, but not the only one.
Other symptoms characteristic of this disease include:
- visual impairment;
- weakening of tongue function;
- anomalies in the anatomical structure;
- deformed feet;
- sensory processing disorder;
- violation of swallowing and sucking reflexes;
- facial skin tension;
- lack of tear secretion;
- disturbances in the functioning of the vestibular apparatus.
Möbius syndrome is a fairly rare disease, so diagnosing this disease in newborns is often difficult, which often leads to an incorrect diagnosis, which carries a certain risk for the baby’s health. A newborn may be diagnosed with cerebral palsy, blindness or deafness, which in itself is not true. Treatment, accordingly, will be carried out based on an incorrect diagnosis.
Diagnosis of Möbius syndrome in a newborn
Timely diagnosis of the disease is very important, as this will allow timely detection of various forms of developmental deviations, but will also reveal the psychological and clinical mechanisms of the disorders.
The most characteristic symptom of Mobius syndrome is the absence of facial expressions.
Other symptoms that help clarify the diagnosis include:
- abnormalities of body structure;
- complete or partial dysphagia (inability to swallow), difficulty sucking;
- Often, reduced intelligence is added to the symptoms; however, intelligence in patients with Mobius syndrome may be normal.
Babies with the syndrome are difficult to feed and care for, since their wishes often have to be guessed. They require additional care in a hospital setting until the symptoms of the disease are eliminated.
The disorder is diagnosed, as a rule, within a short time after birth. The diagnosis can only be made by a doctor based on available data on the symptoms of the disease. Usually no additional procedures are required to make a diagnosis.
Signs and symptoms
The impairment and severity of Moebius syndrome varies greatly among individuals. Classically accepted diagnostic criteria include:
- facial paralysis or weakness affecting at least one, but usually both sides of the face (7th cranial nerve);
- lateral eye movement palsy (6th cranial nerve);
- maintaining vertical eye movements.
Less commonly, other cranial nerves may be affected, including the 5th, 8th, 9th, 10th, 11th, and 12th.
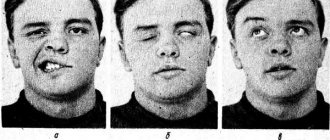
Children with Mobius syndrome may drool excessively and have cross-eyed eyes. Because the eyes do not move from side to side (laterally), the child is forced to turn his head to follow objects. Babies who lack facial expression are often described as wearing a "mask" (see photo below), which is especially noticeable when laughing or crying.
Affected babies may also have feeding problems, including trouble swallowing and poor sucking. Also, corneal ulcers can occur because the eyelids remain open during sleep.
There are many additional deviations. Some children with Moebius syndrome have a short, malformed tongue and/or an abnormally small jaw (micrognathia). A cleft palate may also be present. These disorders contribute to difficulty eating and breathing. Children with cleft palates are prone to ear infections (otitis media). There may be abnormalities of the outer ear, including underdevelopment of the outer part of the ear (microtia) or complete absence of the outer part of the ear (anotia). If the 8th cranial nerve is affected, there is a possibility of hearing loss. Dental abnormalities are not uncommon. Some affected children have speech problems and delays in language development.
Malformations of the skeletal limbs occur in more than half of children with Mobius syndrome. Malformations of the lower extremities include clubfoot and underdevelopment of the legs; Webbing of the fingers (syndactyly), underdevelopment or absence of fingers and/or underdevelopment of the hands may be found on the upper extremities. Some children may have an abnormal curvature of the spine (scoliosis), and approximately 15% of patients also have underdevelopment of the pectoral muscles and chest on one side of the body.
Some affected children have a delay in achieving certain milestones such as crawling or walking, most likely due to upper body weakness; however, most children eventually catch up. Mobius syndrome is rarely associated with mild mental retardation. Some children have been classified as having autism spectrum disorder. The exact relationship between Möbius syndrome and autism is unknown.
Some studies have shown that autism spectrum disorders are more common in children with Möbius syndrome; other studies have not confirmed this and suggest that any such relationships are overestimated.
Möbius syndrome is often associated with various social and psychological consequences. Lack of facial expressions and an inability to smile can cause observers to misinterpret what the sick person is thinking or feeling. Although clinical anxiety and depression are not common in children and adolescents with Mobius syndrome, those affected may avoid social situations due to fear and frustration.
Pathogenesis
Genetic determination and unfavorable antenatal conditions potentiate various disorders, delaying the formation of nuclei and roots of cranial nerves at the level of the brain stem. The facial and abducens nerves are primarily affected. Amymia occurs due to a disturbance in the innervation of the facial muscles.
Denervation of the muscle that rotates the eyeball outward causes convergent strabismus. Often Mobius syndrome involves underdevelopment of other cranial nerves located in the trunk. Hypoplasia of the glossopharyngeal, vagus, and hypoglossal nerves leads to disorders of sucking, swallowing, voice production, and articulation. When the VIII pair is underdeveloped, hearing loss is detected, while the V pair is characterized by a lack of sensitivity of the facial skin.
Genetic determination and unfavorable antenatal conditions potentiate various disorders, delaying the formation of nuclei and roots of cranial nerves at the level of the brain stem. The facial and abducens nerves are primarily affected. Amymia occurs due to a disturbance in the innervation of the facial muscles.
Denervation of the muscle that rotates the eyeball outward causes convergent strabismus. Often Mobius syndrome involves underdevelopment of other cranial nerves located in the trunk. Hypoplasia of the glossopharyngeal, vagus, and hypoglossal nerves leads to disorders of sucking, swallowing, voice production, and articulation. When the VIII pair is underdeveloped, hearing loss is detected, while the V pair is characterized by a lack of sensitivity of the facial skin.
Psychology of social relations
This operation is quite complex from a technical point of view; its duration is rarely less than 8 hours. After this, patients are rehabilitated in the intensive care ward for two days. Fortunately, most people suffering from this defect lead normal lives, work, start a family, and have children.
However, facial expressions are very important for communication and social adaptation. The patient cannot fully develop. Due to the fact that a person is deprived of the ability to smile and has pronounced squint, he is unfairly perceived as an intellectually retarded person. Although mental retardation is observed in only 10% of patients.
It is very difficult for interlocutors to understand what reaction their words evoke and what a person is experiencing at that moment. All this interferes with normal communication, making patients with Moebius syndrome outsiders.
Differential diagnosis
It is necessary to differentiate Moebius syndrome from tumor processes, encephalitis with damage to the brain stem, Down's disease, progressive bulbar palsy, and neuromuscular diseases. In rare cases, when Mobius syndrome occurs with unilateral facial paralysis, the pathology should be distinguished from intracerebral hematomas formed as a result of intracranial birth injury.
Imaging testing: CT scan, MRI are done to rule out any other causes of symptoms. Calcification is detected in the region of the nucleus of the VI cranial nerve. The brain stem may be underdeveloped, the VI, VII nerves are either underdeveloped or absent.
Historical reference
The syndrome was first described in medicine in 1892 by the German neurologist and psychiatrist Paul Mobius. This anomaly is extremely rare, a maximum of 10-20 times per 1 million children born.
German physician Paul Julius Mobius was born in 1853 in Germany and lived there all his life. The scientist studied the clinical development of progressive paralysis and neuropsychic abnormalities in thyrotoxicosis. He made a description of ophthalmoplegic migraine, calling it Möbius disease.
Marden-Walker syndrome. Causes
The causes of this disease in newborns have not yet been fully determined. Doctors' opinions on this matter are divided:
- the former believe that the reason for the development of pathology lies in the improper development of the cranial nerves;
- according to others, the development of pathology is associated with the negative impact of processes that arise as a result of oxygen starvation of the fetus during its intrauterine development;
- According to others, the cause of this rare disease lies in the improper development of the motor facial center.
In newborns with this syndrome, the sucking reflex is poorly developed; they are also unable to swallow food on their own, since their tongue functions are weakened. Sometimes the disease can occur in several family members at once.
Although the disease has been known for a long time, the causes of its occurrence are not fully known. Among the suspected causes, scientists identify abnormal development of cranial nerves and an anomaly in the development of the motor facial center. It is also believed that this anomaly is associated with abnormal intrauterine development of the fetus due to hypoxia.
The disease was first described in 1892 by the German physician Paul Moebius, from whose surname it received its name. The disease manifests itself in the pathology of the development of cranial nerves 6 and 7, and sometimes 3 and 12. This pathology manifests itself as facial paralysis and paralysis of the muscles responsible for lateral eye movement.
Sometimes Möbius syndrome is accompanied by hearing damage. Also, the pathology is often accompanied by other anatomical anomalies.
There are several reasons why this disease occurs. Which one exactly provokes facial nerve paralysis can only be guessed at. One of the reasons is asphyxia of newborns, more often used in the form of the terms “intrauterine hypoxia” or “fetal hypoxia”. Asphyxia (oxygen deficiency) can occur as a result of impaired uteroplacental circulation or due to various pathologies or infections during pregnancy.
The prognosis for children suffering from this rare disease is generally optimistic. There is currently no definitive way to get rid of facial paralysis. However, modern opportunities in medicine ensure that a child with such a disease can count on successful treatment and fully grow and develop on par with his peers.
Marden-Walker syndrome is inherited in an autosomal recessive manner. The exact genetic abnormality has not yet been established.
Causes
Most cases of Moebius syndrome occur accidentally for reasons unknown to doctors (sporadic) in the absence of a family history of the disorder. Sporadic mutations in the PLXND1 and REV3L genes have also been identified in a number of patients and have been confirmed to cause a pattern of findings consistent with Möbius syndrome when administered to animals.
There are also rare cases reported in families. Most likely, Moebius syndrome is a multifactorial disorder, meaning that genetic and environmental factors play a causal role. It is possible that there are different reasons in different cases (heterogeneity).
In familial cases, there is evidence that Möbius syndrome is inherited as an autosomal dominant trait. Dominant genetic disorders occur when only one copy of the abnormal gene is needed to cause the disease. The abnormal gene may be inherited from either parent or may be the result of a new mutation (gene change) in the affected person. The risk of passing the abnormal gene from the affected parent to the offspring is 50% for each pregnancy, regardless of the sex of the child.
The spectrum of findings in Möbius syndrome indicates a malformation of the hindbrain. Several different theories have been proposed to explain the cause of Mobius syndrome. One hypothesis is that the disorder results from reduced or interrupted blood flow (ischemia) to the developing fetus during pregnancy (in utero). Recent research suggests that a lack of blood affects certain areas of the lower brain stem that contain the cranial nerve nuclei. This lack of blood flow can be caused by environmental, mechanical or genetic causes. However, the cause of the syndrome remains unclear and more basic and clinical research is needed.
Complications
The prognosis for the life of children with Mobius syndrome is favorable. Most of these children lead a normal life, but modern society creates incredible difficulties for such children, preventing them from adapting among their peers. Constant ridicule and bullying from peers, especially in adolescence, undermines such children's self-confidence and makes them social outcasts.
This attitude towards them from others interferes with normal communication and development of the child. Often such children choose loneliness at a certain stage of their lives, which subsequently does not prevent them from starting a family, having friends and adapting to society.
The prognosis for newborns with Mobius syndrome is favorable. Surgical intervention will partially restore the functions of the facial nerves and give the child the opportunity to adapt in the future among his peers.
Most children with Mobius syndrome today have the opportunity to lead a normal and fulfilling life on an equal basis with other children.
The prognosis for the life of children with Mobius syndrome is favorable. Most of these children lead a normal life, but modern society creates incredible difficulties for such children, preventing them from adapting among their peers. Constant ridicule and bullying from peers, especially in adolescence, undermines such children's self-confidence and makes them social outcasts.
This attitude towards them from others interferes with normal communication and development of the child. Often such children choose loneliness at a certain stage of their lives, which subsequently does not prevent them from starting a family, having friends and adapting to society.
Swallowing disorders are dangerous due to food entering the respiratory tract with asphyxia. The accumulation of food debris in the oral cavity creates favorable conditions for the development of caries and other dental diseases. Due to disturbances in the structure and functioning of the upper respiratory tract (nasopharynx, larynx), respiratory infections often occur, which can be complicated by pneumonia.
Similar disorders
Symptoms and signs of the following disorders may be similar to those of Mobius syndrome. Comparisons may be useful for differential diagnosis.
Several investigators have reported cases in which features of Möbius syndrome occur in association with Poland syndrome . It is sometimes called Poland-Mobius syndrome. Poland syndrome is characterized by webbed fingers, absent or underdeveloped fingers or hands, and underdeveloped chest and chest muscles. Polish syndrome usually occurs on only one side of the body (ipsilateral).
There is debate in the medical literature as to whether Möbius syndrome, Poland syndrome, and Poland-Möbius syndrome represent three different disorders or three different manifestations of a single disorder.
Hereditary congenital facial palsy is characterized by isolated facial palsy, and subgroups of the disease have other associated features, including hearing loss and strabismus. Hereditary congenital facial palsy differs from Moebius syndrome by the presence of a complete horizontal gaze. HOXB1 mutations on chromosome 17q21 were identified in patients with this pathology.
Human HOXA1 syndromes are rare disorders with complex neurological and systemic manifestations. The range and types of clinical outcomes in patients suffering from this disease vary greatly. Affected individuals have Duane phenomenon (“conjugate gaze palsy”), which is characterized by restriction of lateral eye movements. Hearing loss, developmental delays, and a spectrum of internal carotid artery and spinal malformations have also been documented. Facial asymmetry and minor malformations of the outer ear are also sometimes present. Affected people may also show signs of cognitive and behavioral impairment, and some people have been classified as having autism spectrum disorder.
There are other causes of congenital facial paralysis, in particular microsomia of the facial hemisphere and, possibly, birth trauma. There are also acquired types of facial paralysis. Melkersson-Rosenthal syndrome is characterized by sudden onset in childhood/adolescence, bilateral or unilateral facial weakness, chronic swelling of the face (especially the lips), and a furrowed tongue.
Other Possible Causes:
- infections such as Ramsay-Hunt syndrome;
- systemic and neurological disorders, including cerebral palsy, congenital muscular dystrophy, spinal muscular atrophy, Guillain-Barré syndrome, multiple sclerosis and autoimmune disorders;
- brain injury;
- tumors or damage to the brain stem.
Treatment
Children with Mobius syndrome rarely suffer from heart disease. Sometimes there is dextrocardia (the heart is located on the right side of the heart instead of the left), a ventricular septal defect, or abnormal attachments of large blood vessels to the heart (great vessel transfer or complete anomalous pulmonary venous connection).
Genetic counseling can be beneficial for patients and their families. Treatment is symptomatic and supportive only.
Conservative orthopedic treatment and physical therapy will be indicated. Developmental problems will be persistent and severe, but contractures are not progressive and will improve with age and physical therapy.
In relation to the disease, complex therapy is carried out, aimed at correcting existing congenital anomalies, maintaining the functioning of the brain, musculoskeletal system, and psychological support for the patient and his loved ones. Nutrition is provided using a special syringe, through a tube, and, if necessary, parenterally. The child is consulted by a pediatrician, a pediatric surgeon, a plastic surgeon, an ophthalmologist, a psychologist, and an orthodontist. Treatment includes the following components:
- Neurological. Supportive neurotropic pharmacotherapy with amino acids, nootropic, vascular, and vitamin preparations is carried out. Correction of amymia is performed surgically; the operation involves transplanting a muscle graft from the thigh to the face.
- Ophthalmological. In order to prevent complications of xerophthalmia, moisturizing eye drops are constantly instilled. If inflammation develops, antibacterial drops are prescribed. To protect the cornea, partial tarsorrhaphy is indicated - suturing the edges of the eyelids. Strabismus requires surgical treatment.
- Orthopedic. Involves surgical correction of malformations of the extremities: separation of the fingers in case of syndactyly, elimination of clubfoot, operations on the bones and joints of the foot. It is recommended to wear orthopedic shoes, regular exercise therapy, physiotherapy, and massage.
- Dental. Closing of the cleft palate, orthodontic treatment of malocclusions, and straightening of the dentition are carried out. In severe cases, treatment is carried out using maxillofacial surgery.
- Speech therapy. Articulation gymnastics and speech therapy massage are used. Regular classes with a speech therapist are prescribed to correct dysarthria, OHP.
- Psychological. Of great importance in complex treatment are the child’s sessions with a psychologist, child psychotherapy, art therapy, and psychological counseling of parents. For the purpose of social adaptation, older children take part in group psychological trainings.
What can you do
Since the causes of this disease are not fully understood, it is not possible to completely get rid of the pathology today.
It is for this reason that doctors are trying to help not only such children, but also their parents. In this matter, psychological assistance to parents is very important, which in turn will help support the normal functioning of the child at every stage of his development and maturation. Such children need the help of qualified specialists who can provide certain symptomatic assistance - correction of gait, speech, strabismus, etc.
What does a doctor do
There is currently no radical method of therapy in the treatment of this pathology. The only thing that modern medicine can offer in solving this issue is surgical intervention, the essence of which is to replace non-working muscles on the face with others, which are usually transplanted from the child’s hip.
The operation is quite complex and lasts about 9 hours, after which the child is transferred to the intensive care unit, where he must remain for several days.
Properly performed surgical intervention will make it possible to restore facial expressions. The child’s tongue function may be partially restored, he will be able to close his lips and subsequently adapt to society. Unfortunately, it is impossible to completely cure this disease.
What can you do
To date, there are no radical methods of treating this disease in children.
At the same time, parents of such a special child should know that in the process of his growing up and development, he can be provided with symptomatic assistance, which consists of correcting speech, pronunciation, strabismus, and more. The only way to help such children is to perform a surgical operation aimed at eliminating the defect of atrophied facial muscles. This operation will allow the child to partially restore his facial abilities and give him the opportunity to adapt among his peers.
What does a doctor do
Due to the fact that it is impossible to completely cure this pathology, the only way out of the situation seems to be surgical intervention, which is aimed at restoring facial expressions.
The essence of the operation is to replace atrophied facial muscles with others. Typically, muscles are taken from the thigh and transplanted to the face. The operation is technically complex and lasts about 9 hours. After this, the child will still have to spend several days in the intensive care unit.
In addition, the following activities will help alleviate the condition of a child with Mobius syndrome:
- early speech therapy work;
- special classes for the development of articulation;
- facial and tongue massage.
Mobius syndrome - treatment
Answering the question - how to treat Mobius syndrome is not so simple. There is no definitive system suitable for all patients. Treatment of this disease involves complex therapy involving many highly qualified specialists. Therapy corrects disorders of a certain type that a particular patient has, depending on his individual picture of the disease.
Mobius syndrome requires the involvement of the following specialists:
- neurologist;
- pediatrician;
- otolaryngologist;
- orthopedist;
- dentist;
- speech therapist;
- plastic surgeon;
- audiologist;
- ophthalmologist.
The list can be continued indefinitely, because each case requires the involvement of a larger number of specialists, or a selective one of one direction or another. The pathology is so unique and unpredictable that it is possible to give a definite direction of treatment only after a detailed study of the medical history. Moebius syndrome is treated in various ways, including surgery, but mainly involves accompanying constant monitoring.
It is difficult to imagine a person who cannot laugh, cry or express any emotions. However, there are such people, and they have been given a terrible diagnosis - Moebius syndrome. Photos of such people at first glance may seem quite normal, but during live communication you realize that their face is completely immobilized. This is a congenital anomaly that develops for the main reason due to the abnormal structure of the cranial nerves. Facial paralysis is one of the most terrible defects of the human body. It is characterized by a lack of facial expressions; the face appears frozen and mask-like.
Historical reference
The syndrome was first described in medicine in 1892 by the German neurologist and psychiatrist Paul Mobius. This anomaly is extremely rare, occurring maximum 10-20 times per 1 million children born. German physician Paul Julius Mobius was born in 1853 in Germany and lived there all his life. The scientist studied the clinical development of progressive paralysis and neuropsychic abnormalities in thyrotoxicosis. He made a description of ophthalmoplegic migraine, calling it Möbius disease.
Alleged reasons for development
The most severe form of pathology is considered to be Mobius syndrome, the causes of which are still unknown to medicine. The opinions of researchers and specialists are divided.
- The first believe that the reason is improper development of the cranial nerves.
- The latter are convinced that this is the harmful influence of destructive processes that develop as a result of oxygen starvation of the child in the womb.
- Still others point to the abnormal development of the motor personal center as the main cause of the disease.
- anatomical abnormalities;
- foot is deformed;
- difficulty swallowing and sucking;
- sensory perception disorders;
- weakening of language functions;
- visual impairment.
- cerebral paralysis;
- blindness;
- deafness.
- absence or fusion of fingers;
- deformation of the ears;
- epicanthus.
Moebius syndrome is a fairly old and very mysterious disease. This is a congenital anomaly of the facial muscles, due to which facial expressions are completely absent. Paralysis can be unilateral or bilateral. The person does not react in any way to external stimuli, does not smile, does not frown, and is completely devoid of emotions. Children have a poorly developed sucking reflex; they cannot swallow food and water on their own due to weakened tongue function. Often the disease affects several family members.
Symptoms
Mobius syndrome is a congenital neurological disorder that is quite rare. People with this pathology lack the ability to move their facial muscles and eyes from side to side. This disease entails serious disturbances in the functioning of the musculoskeletal system and deformation of the feet. The main clinical manifestation of the syndrome is mobility restrictions, but there are others, pronounced ones, which confirm that this is Mobius syndrome, symptoms:
There is also a violation of vestibular excitability and lack of tear secretion. The skin of a sick person on the face is stretched, without wrinkles, even when laughing or crying. It does not move in relation to the subcutaneous tissue; the corners of the mouth are always lowered. The defect is accompanied by limb abnormalities such as syndactyly, clubfoot, brachydactyly and extra digits. With partial paralysis, the process mainly involves the muscles of the upper part of the face; the tissues do not sag as much as with an acquired disease.
Diagnosis of pathology
An anomaly such as Moebius syndrome is quite rare. Diagnosis is therefore difficult, especially in young children, and often leads to misdiagnosis, which is more dangerous and requires surgical treatment, for example:
Examination and subsequent therapy are being conducted in this direction. Modern medicine cannot yet fully study the cause of this disease, therefore, it is also not possible to cure it completely. Research and study of genetic material from patients at the chromosome level is being conducted in search of cell mutations. Today, doctors set themselves the task of helping parents of children suffering from this syndrome in maintaining normal functioning at every stage of life. This is possible when correcting speech, strabismus, and strokes. Timely diagnosis is necessary not only to identify various forms of developmental disorders, but also to assess the degree of development of mental functions and identify psychological and clinical mechanisms of disorders. The diagnosis of abnormal development includes psychological, pedagogical and clinical genetic research. It is carried out to determine the level of delay in emotional, behavioral, intellectual and speech development. It also influences the establishment of a connection between the underlying disease and other pathological manifestations, age and neurological condition of the patient.
Treatment of Mobius syndrome
Only surgical treatment can help get rid of such an insidious disease as Mobius syndrome. It is impossible to completely cure the disease, except for cosmetic deformity, impaired swallowing functions and other problems of the body, which entails a defect; patients experience severe psychological stress throughout their lives. This condition can only be alleviated through surgery. With the help of plastic surgery, it is possible to create artificial facial expressions, which means that the patient will be able to raise the corners of the mouth, experiencing a feeling of joy. The rest of the face will remain immobilized and expressionless. There are cases that after such procedures, patients are disappointed with the results. Therefore, before the operation, the patient is fully informed about the consequences and possible complications.
Psychology of social relations
This operation is quite complex from a technical point of view; its duration is rarely less than 8 hours. After this, patients are rehabilitated in the intensive care ward for two days. Fortunately, most people who suffer from this defect lead normal lives, work, create families, and give birth to children. However, facial expressions are very important for communication and social adaptation. The patient cannot fully develop. Due to the fact that a person is deprived of the ability to smile and has a pronounced squint, he is unfairly perceived as an intellectually retarded person. Although mental retardation is observed in only 10% of patients. It is very difficult for interlocutors to understand what reaction their words evoke and what a person feels at that moment. All this interferes with normal communication, making patients with Moebius syndrome outsiders.
Mobius syndrome in children
Young children tend to express various emotions and quite often, so a child suffering from Mobius syndrome is immediately visible. He does not react in any way to external stimuli, does not cry, does not laugh, and even blinks with difficulty. Only by sounds can you vaguely understand what the baby needs. From birth, such children have a motionless face, a clear asymmetry, an open mouth, eyes that close poorly, and the child can only follow objects by moving his head. Mental retardation is rarely observed; the patient needs massage not only of the face, but also of the tongue, developing articulation classes.
Symptoms in a newborn
Moebius syndrome is a hereditary pathology, the type of inheritance is autosomal recessive or, less commonly, dominant. With the syndrome, while still in the maternity hospital, the mother notices that the child’s facial expressions are unnatural, he does not cry or close his eyes, sometimes even at night. Such children also have abnormal defects:
Although the specific causes of the disease have not yet been established, doctors suggest that taking medications and drugs during pregnancy increases the risk of pathology. Mobius syndrome in children cannot be completely cured, although its manifestations become milder with age.
Trainings to improve communication skills
Thanks to special trainings organized by Danish professors, people suffering from Mobius syndrome improve their social communication skills. The goal of the training is to activate paralinguistic means of communication using intonation and various gestures. The effectiveness of the classes has been repeatedly proven by experiments and observations; during the dialogue, patients cease to experience nervousness, do not fuss and become more relaxed. According to the results of the patients themselves, many do not feel any improvement. The project's co-author is Kathleen Bogar, who was diagnosed with Mobius syndrome. She built a career and became a successful doctor; in her work, she pursues the main goal - to develop a program that will help people suffering from Mobius syndrome adapt to society.