Causes of subarachnoid hemorrhage
In most cases, this condition is caused by non-traumatic factors:
- aneurysm rupture;
- rupture of a vessel in the brain against the background of arterial hypertension, atherosclerosis and other vascular diseases.
Subarachnoid hemorrhage in the brain can also be caused by traumatic factors:
- traumatic brain injury;
- brain contusion;
- fracture of the skull bones.
Main services of Dr. Zavalishin’s clinic:
- consultation with a neurosurgeon
- treatment of spinal hernia
- brain surgery
- spine surgery
World Federation of Neurological Surgeons (WFNS) severity scale
| Severity | GCS scores | Severe neurological deficit* |
| 0** | — | — |
| I | 15 | No |
| II | 13-14 | No |
| III | 13-14 | Yes |
| IV | 7-12 | Not really |
| V | 3-6 | Not really |
“*” - aphasia, hepiparesis/hemiplegia
“**”—diagnosed unruptured aneurysm
Clinical picture of subarachnoid hemorrhage
This condition develops rapidly against the background of a person’s normal well-being and manifests itself:
- sharp acute headache, worsening with the slightest physical activity;
- nausea, vomiting;
- convulsions;
- psycho-emotional disorders (fear, agitation, drowsiness);
- increased body temperature (up to febrile and subfebrile levels);
- disorders of consciousness (from stupor to fainting, coma);
- symptoms of damage to the oculomotor nerve (gaze paresis, drooping eyelid), hemorrhage in the eyeball.
In half of the cases, this condition leads to death. The main complications and consequences of subarachnoid hemorrhage:
- spasm of cerebral vessels caused by ischemia;
- recurrence of an aneurysm episode (may occur early or several weeks after the first episode);
- hydrocephalus (in the initial stages or in the late period);
- pathologies caused by subarachnoid hemorrhage in the brain (myocardial infarction, pulmonary edema, bleeding from a stomach or duodenal ulcer).
Among the long-term consequences of subarachnoid hemorrhage in the brain: memory disorders, attention, psycho-emotional disorders (depression, insomnia, agitation). Also, a standard complaint of patients who have suffered this condition is headache. Somewhat less frequently, hormonal disorders develop in the hypothalamic and pituitary gland systems.
SAH severity scale (W. Hunt, R. Hess)
| Severity | GCS scores | Clinical criteria |
| I | 15 | Clear consciousness, asymptomatic or headache |
| II | 13-14 | Stun. Moderate cephalgic and meningeal syndrome, oculomotor disorders |
| III | 13-14 | Stun. Pronounced meningeal syndrome, moderate focal symptoms |
| IV | 7-12 | Stupor, coma I. Meningeal and focal symptoms are pronounced. Akinetic mutism. |
| V | 3-6 | Coma II, III. Violation of vital functions. |
The degree of damage determines the management tactics of a patient with this pathology. Patients whose condition corresponds to grades I–III are subject to surgical treatment, while grades IV–V are treated conservatively.
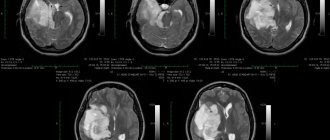
Diagnosis and treatment of subarachnoid cerebral hemorrhage
The doctor clarifies the victim’s medical history and conducts an external examination. The diagnosis is established on the basis of CT data, which makes it possible to determine the extent of the process, the presence of edema, and assess the condition of the cerebrospinal fluid system. If the results are negative, a lumbar puncture is performed.
MRI is a sensitive tool for diagnosing pathology after a few days. Vascular angiography is used to determine the source of bleeding in the brain.
Therapy for subarachnoid hemorrhage takes place in a neurological hospital and depends on the severity of the patient’s condition. It is aimed at solving the following problems:
- stabilization of the patient's condition;
- prevention of recurrent episode;
- normalization of homeostasis;
- treatment and prevention of ischemia, vascular spasm;
- therapy for the disease that caused the hemorrhage.
The aneurysm is clipped or endovascular occlusion is performed. Vasospasm and ischemia are treated with medication. In case of local spasm of a vessel, a vasodilator drug is injected directly into it or balloon angioplasty is performed.
In 50% of cases, subarachnoid hemorrhage leads to death. The majority develop significant impairments in the functional activity of the brain.
You can get help with this pathology at the Department of Neurosurgery of the City Clinical Hospital named after. A.K. Eramishantseva. The clinic has modern diagnostic equipment and advanced equipment for performing complex operations.
Classification of hemorrhages in the ventricles of the brain
Hemorrhages in the ventricles of the brain are divided into:
- Primary. They are observed very rarely (about one case out of three hundred).
- Secondary. They make up the bulk of hemorrhages of this type.
Parenchymal type hemorrhage is divided into 3 types:
- Hemorrhage into the lateral ventricles. With this type of hemorrhage, the anterior and posterior parts of the ventricles are affected, less often the central one. In this case, a syndrome of increased intracranial pressure and compression of the brain stem with blood may occur. If the bleeding is extensive, then the rush of blood usually occurs through the optic tubercle or caudate compartment. Next, the blood enters the third ventricle through the foramen of Monroy and the lateral ventricle of the adjacent hemisphere. The foramen of Luschka then passes through the aqueduct of Sylvius and enters the subarachnoid space of the spinal cord and brain.
- Hemorrhage into the third ventricle. Occur through the optic thalamus. Sometimes a rush of blood is observed in several parts of the ventricular system at once.
- Hemorrhage into the fourth ventricle.
There are several options for hemorrhage into the ventricles of the brain.
- Massive hemorrhages that destroy the walls of the third ventricle. In such cases, a very large volume of blood is poured out, which fills the entire ventricular system in a relatively short time. Extensive necrosis occurs in the brain. If surgery is performed, it is flattened. This type of hemorrhage leads to the death of the patient within about 24 hours.
- A rush of blood moves from the parenchyma to the lateral ventricle and fills several horns of the cavity of this ventricle or its entire space at once. Next, the blood fills the third ventricle and the lateral ventricle of the opposite hemisphere and enters the ventricle through the aqueduct of Sylvius. With a large volume of blood spilled, the volume of the brain also increases, this causes bilateral symptoms. The course of the pathology is about five days. There is a rupture of the gray matter under the corpus callosum, thus blood penetrates from the region of the basal ganglia into the lateral ventricle. In this case, the difference in the density of white and gray matter plays a big role.
- Hemorrhage into the third ventricle can be caused by parenchymal lesions medial to the optic thalamus. Symptoms increase quickly, which leads to rapid death. Surgical intervention in such cases is performed extremely rarely due to the inaccessibility of the lesion. Lateral lesions have a more favorable prognosis and make it possible to perform surgical intervention. In such cases, a rush of blood fills the anterior or posterior horn of the lateral ventricles and provokes hemorrhage into the intrathecal spaces.
- As a result of hemorrhage, the lateral ventricle is partially filled with blood when hemorrhaging into the brain parenchyma. The hemorrhage does not spread to other ventricles. Such pathologies most often have a long course.
- There are also extensive parenchymal hemorrhages, in which the lateral ventricle is completely filled with blood and a significant displacement of the oral part of the brain stem occurs. As a result of compression, the passage into the foramen of Monroe narrows and is completely blocked, so blood does not penetrate further into the third ventricle. In this regard, the cavity of the lateral ventricle in the adjacent hemisphere of the brain expands significantly. Thus, contralateral hydrocephalus occurs.
- Hemorrhage into the third ventricle. Basically, blood gets there from the parenchyma after hemorrhage in the area of the visual thalamus. In rare cases, the blood flow originates in the choroid plexuses.
- Blood enters the gastric system from the cerebellum. There are frequent cases of blood entering the third ventricle, and the ventricular cavity fills quickly and completely. This type of hemorrhage leads to the rapid death of the patient.
There are different options for classifying this type of pathology.
According to one of them, there are four stages of hemorrhage in the ventricles of the brain:
- Grade 1 - a small amount of blood accumulates around the vessels. This type of hemorrhage is called subependymal. It is not life-threatening and most often goes away on its own after some time without any consequences.
- 2nd degree - blood enters the ventricular cavity, but has little effect on the patient’s life. In most cases, it resolves on its own, often without consequences.
- Stage 3 - a blood clot enters the ventricular passage and blocks it, thereby causing the volume of the ventricle to expand as it fills with blood. Sometimes the elimination of such pathology occurs spontaneously, by itself. But in some cases, surgical intervention is still necessary, in which a shunt is installed to unblock the ventricular passage and prevent the development of hydrocephalus. Neurological symptoms are often observed.
- 4th degree - blood enters both the ventricles of the brain and its parenchyma. This pathology poses a threat to the patient’s life and is accompanied by severe neurological symptoms (frequent seizures, development of anemia, etc.).
According to another classification, there are three stages of hemorrhage in the ventricles of the brain:
- Subepindeminal - hemorrhage under the layer of tissue lining the internal cavity of the ventricle. It occurs in premature babies and is characterized by the absence of neurological symptoms.
- Subepindamal-intraventricular hemorrhage into the ventricular cavity. It occurs in premature babies and is accompanied by a state of shock, respiratory tract pathology (the child cannot breathe independently), increased intracranial pressure, convulsions, and in some cases coma.
- Subepindeminal-intraventricular-periventricular is a hemorrhage in which not only the ventricle is saturated with blood, but also the tissue that surrounds it. It is observed in premature babies. This stage is characterized by shock, convulsions, respiratory tract pathologies, increased intracranial pressure, and dysfunction of the brain stem.
Symptoms of various etiological types of SAH
With aneurysmal subarachnoid hemorrhage, periods are distinguished:
1. Latent
2. Prodromal - local or “migraine” headache, dizziness, which may be accompanied by photophobia, vomiting, diplopia, blurred vision and consciousness, and short-term stiff neck.
3. Hemorrhagic - damage to the II, III, V, VI pairs of the cranial nerve, short-term speech disorders, sensitivity, epileptic seizures or status with transient pyramidal symptoms, clinic of sphenoidal fissure syndrome, transient ischemic attack. Hypothalamic disorders: vasomotor disorders (pallor of the skin, increased blood pressure, tachycardia, hyperthermia, increased breathing, total vasospasm), catabolic (hyperglycemia, azotemia), neurodystrophic (papules, blisters, maceration, ulcerations, bedsores, cachexia in the last 2-3 weeks of illness).
The hemorrhagic period has 3 phases:
1) initial – the first three days after aneurysmal hemorrhage,
2) expanded – up to 1 month after aneurysmal hemorrhage;
3) outcome phase:
√ with a compensated course of the hemorrhagic period, regression of pathological symptom complexes occurs with the patient’s recovery;
√ with a subcompensated course, persistent organic damage to the brain occurs;
√ with a decompensated course, irreversible structural multiorgan changes develop, leading to death.
4. Period of recurrence of subarachnoid hemorrhage.
5. Residual or post-hemorrhagic period.