Description of the disease
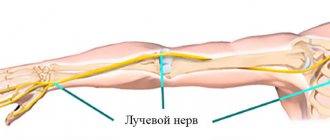
Vessels, nerves, synovial membranes, and tendons pass through the carpal (carpal) canal. The median nerve is also located here - the main nerve of the arm, running from the brachial plexus to the fingertips. Responsible for coordination of movement, fine motor skills of the hands, contraction and expansion of blood vessels from the action of external stimuli, regulates the functioning of the sweat glands. The width of the canal is limited on three sides by bones and the transverse ligament.
The carpal tunnel itself is quite narrow, which contributes to the formation of various pathologies. Any additional narrowing entails compression of the processes of nerve fibers and blood vessels, and blood supply is disrupted. Pathological processes proceed slowly, begin with a loss of physiological sensitivity, and lead to motor and trophic disorders. The picture of the disease has clear symptoms with a characteristic clinical picture, which makes it easy to make a diagnosis even at the initial stage.
Differential diagnosis
The differential diagnosis should consider all conditions that could potentially cause dysfunction of the median nerve, brachial plexus, C5-8 nerve roots, or central nervous system.
Possible differential diagnoses for CTS include:
- compression of the median nerve at another level;
- pronator teres syndrome;
- anterior interosseous syndrome;
- damage to nerve endings in the palm;
- cervicobrachial syndrome.
Symptoms of the disease
- 1. Reduced sensitivity of the hand.
First, patients begin to notice numbness in their fingers immediately after waking up. Over time, the periods of paresthesia increase, and feelings of burning, pain, cold or heat are added. Carpal tunnel syndrome is characterized by a simultaneous, radically opposite change in sensitivity. In one area it increases, but the other part of the palm does not feel anything.
- 2. Burning pain in the palms with shooting in the fingers.
Initially, the pain is felt in the area where the nerve is pinched, then it gradually begins to affect the entire arm: from the shoulder to the fingertips. This is accompanied by swelling of the wrist. As a rule, the dominant hand hurts: the right hand in a right-handed person, the left in a left-handed person, but bilateral symptoms also occur.
- 3. Muscle weakness and impaired motor activity.
As a result of prolonged pinching and inflammation of the nerve fibers, the hand loses muscle strength, and movement restrictions appear. It becomes difficult to operate small objects, such as buttoning buttons. The function of grasping and then holding objects weakens. Gradually, a decrease in the performance of the hand leads to muscle atrophy and deformation of the hand.
- 4. Lesions of the autonomic nervous system.
This is expressed in a pale and sometimes bluish color of the hand, dry skin, brittle nails, and cold hands.
Naturally, carpal tunnel syndrome affects the general physical and mental condition of the patient. He loses his ability to work, his quality of life decreases. Regular pain and a constant feeling of discomfort intensify at night, which interferes with normal sleep and causes insomnia.
A characteristic feature of this disease is that the patient can relieve discomfort on his own, without resorting to medications. To do this, just lower your hands down, move your fingers, shake your hands, stretch them, do massage, gymnastics. These manipulations help restore blood supply, but, unfortunately, not for long, since they do not get rid of the causes.
Clinical picture
The onset of the disease is usually gradual with tingling or numbness in the area of innervation of the median nerve. Patients may notice an exacerbation of symptoms when statically grasping objects such as a telephone or steering wheel, or at night or in the early morning. Many patients report improvement in symptoms after shaking or flapping their hands.
As the disease progresses, the tingling or numbness sensation may become constant and patients may complain of a burning pain. The final symptoms are weakness and atrophy of the thenar muscles. These combined symptoms of sensory impairment and weakness can lead to complaints of clumsiness and loss of grip strength, resulting in things falling.
Diagnostics
It is easy to make a diagnosis of this disease; it is enough to interview the patient and conduct several tests, since carpal tunnel syndrome has clear distinctive features. Among them are the symptoms described above and preservation of the functions of the little finger, which is not affected when the nerve and vessels in the carpal tunnel are pinched.
The doctor also performs palpation and the following tests:
- Hoffman-Tinel test: tapping the area of the median nerve. With carpal tunnel pathology, the patient feels numbness, tingling, and burning in the palm of his hand.
- Phalen test: bending the hand at the wrist joint as much as possible, the patient feels pain and numbness in the palm.
- It is difficult to hold your arms raised above your head for more than 1 minute; pain and numbness of the limbs begin.
- It is impossible to connect (touch) the thumb with the little finger.
- To confirm the correctness of the diagnosis, determine the extent of the lesion and associated complications, additional examinations are prescribed:
- Electroneuromyography to evaluate the conduction of nerve impulses is the gold standard for diagnosing carpal tunnel syndrome.
- Ultrasonography helps detect damage and inflammation.
A neurologist, physiotherapist and hand surgeon can make a diagnosis and carry out treatment.
Physical examination
May include testing for sensory and motor impairments. There are several specific tests with varying degrees of sensitivity and specificity.
- The most reliable is the wrist compression test. This is done by applying firm pressure directly over the carpal tunnel for 30 seconds. The test is considered positive if paresthesia, pain or other symptoms are reproduced.
- The square test is an assessment of the risk of developing CTS. The test is considered positive if the ratio of wrist thickness divided by wrist width is greater than 0.7.
- Another test is palpation diagnostics. In this test, the doctor examines the soft tissue over the median nerve for mechanical restriction.
- The reverse Phalen test or praying hand position is performed by having the patient extend both wrists, placing the palmar surfaces of both hands in relation to each other for one minute (as if praying). The test is considered positive when symptoms appear.
- The Phalen test or reverse prayer positioning of the hands is performed with the patient fully flexing the wrists, positioning the dorsal surfaces of both hands relative to each other for one minute. The test is considered positive when symptoms (numbness, tingling, pain) are reproduced.
- Despite its low sensitivity and specificity, the Hoffman-Tinel sign is the most commonly performed test. In this test, a healthcare professional taps directly on the carpal tunnel to stimulate the median nerve. As with the tests described above, the test is considered positive when symptoms are reproduced.
Clinical prediction rules (CPRs), particularly for carpal tunnel syndrome, are a reliable screening tool.
Treatment of carpal tunnel syndrome
All measures taken are aimed at eliminating the cause of the disease - complete or partial elimination of compression of the median nerve. The treatment method depends on the severity of the syndrome. Choose between conservative and surgical treatment. It is also the doctor’s job to identify the cause of the disease in order to limit movements that worsen the symptoms.
Conservative treatment
Patients are prescribed to wear an orthosis, which holds the wrist joint in a position that is safe for blood vessels and nerves. It is recommended to wear it constantly, during the day and at night. According to statistical data, orthotics are effective in the early and middle stages of the disease. It is recommended to switch to a salt-free diet and limit fluid intake to reduce swelling.
Medicines are also prescribed:
- Nonsteroidal anti-inflammatory agents to reduce pain and inflammation.
- Corticosteroids orally or by injection to relieve pain and restore joint mobility.
- Vascular drugs to improve blood supply to tissues.
- Diuretics to relieve swelling.
- Vitamin B6 to relieve symptoms and increase the effectiveness of treatment.
Physiotherapy helps to speed up the therapy process and achieve a positive result faster: electrophoresis, UHF, magnetic therapy and other methods. A course of physical therapy and massage are often prescribed. The complex combination of these methods of therapy and the use of medications leads to remission in 59% of patients. The rest are forced, on average, after 1-2 years to turn to a hand surgeon for surgery.
Surgery
If conservative treatment is ineffective and the disease is advanced, surgery is prescribed. They are dealt with only by hand surgeons - highly specialized specialists who perform surgical procedures on the hand. The purpose of the operation is to release the median nerve and reduce pressure. There are two ways to open the carpal tunnel:
- An open surgical procedure in which an incision of about 3 cm is made on the wrist. Having gained access, the surgeon cuts the ligament, increasing the volume of the carpal tunnel.
- Endoscopy has a shorter incision length, which is up to 1.5 cm, but is performed in two places. They are necessary to insert a microchamber, which can be used to dissect the ligament.
Both types of surgery are performed under local anesthesia. Sometimes excision of tissue around the nerve and tendons with scarring, ovaries and cords is required. On average, the procedure is carried out within 20 minutes.
At first, the patient may feel pain in the scar area and physical weakness of the wrist. It will take several months until complete recovery; the period is individual in each specific case. Rehabilitation consists of gymnastics, massage, and physiotherapy. During the recovery period, many have to give up their type of activity if it affects recovery.
According to statistics, up to 90% of patients who undergo surgical treatment completely restore the physical activity of their hands and get rid of the symptoms of carpal tunnel syndrome. Relapses occur in 8 - 12% of cases.
Alternative treatments.
You can relieve the symptoms of carpal tunnel syndrome without medication or surgery. To do this you need:
- Reduce the load on your hands and wrists, and eliminate activities that worsen the condition.
- Secure the arm with a splint, orthosis or elastic bandage to limit mobility.
- Relieve swelling with ice, limit fluid and salt intake.
- Perform hand exercises aimed at stretching the joints. We recommend exercising under the supervision of a physiotherapist.
If there is no improvement, then you should not delay consulting a doctor.
Diagnostic procedures
Ultrasound and MRI are the two imaging modalities that are best suited for investigating compression syndromes. Along with direct visualization of direct causes and anatomical variations, recognition of pathological MRI patterns from muscles can indicate the affected nerve.
Electromyography and nerve conduction studies are the basis for the diagnosis of CTS. Other clinical or special tests do not confirm CTS, but help rule out other diseases. These results may prompt electromyography and nerve conduction studies. X-rays are recommended to rule out other causes of wrist pain, such as arthritis or bone pathology.
Rating scales
There are several questionnaires available to measure outcome measures in CTS.
- Boston CTS Severity Questionnaire (BCTQ).
- Disability of the Arm, Shoulder, and Hand (DASH) Questionnaire.
- Brigham and Women's Clinic Questionnaire.
- Patient Evaluation Scale (PEM). This is a self-administered, interview, or telephone questionnaire to assess physical health. It consists of 3 components (patient perception of care, hand health profile, global assessment) and a total of 18 items scored on a 7-point scale. Low scores indicate positive results. Hobby et al. found the instrument to be valid and reliable and to have good sensitivity.
What happens if you don't get treatment?
Carpal tunnel syndrome is not life-threatening and is a slowly occurring pathological process. The disease has a favorable prognosis for recovery, but due to neglect of their health, some people are in no hurry to visit a doctor. Over time, this leads to a decrease in motor activity, muscle strength, and impaired fine motor skills. If left untreated, irreversible processes will begin and the median nerve will atrophy. This will lead to the loss of functionality of the brush, which will no longer be possible to return.
Treatment
If CTS is detected, early conservative treatment is recommended.
- Initially, the patient should be counseled regarding changes in symptoms associated with wrist movement. For example, you can ensure proper hand ergonomics by placing the keyboard at the right height to minimize flexion, extension, abduction and adduction of the hand when typing.
- If possible, it should be recommended to reduce the number of repetitive activities that cause symptoms.
Non-surgical treatment includes NSAIDs, diuretics, vitamin B6, and hand splinting/orthosis. If this is not successful, oral or topical glucocorticoids (median nerve blocks) can be tried.
- If these measures fail, surgery is indicated to free the median nerve in the carpal tunnel (but only after nerve conduction studies have shown significant axonal degeneration).
- Releasing the nerve is usually performed by an orthopedic or hand surgeon.
- This procedure can be performed either openly or endoscopically.
- This operation is considered relatively simple. The idea is that the transverse carpal ligament or flexor retinaculum is cut, allowing more space in the carpal tunnel and reducing pressure on the median nerve.
- It usually does not require a long hospital stay.
Physical therapy
Patients with mild to moderate symptoms can be effectively treated in a primary care setting.
Physiotherapists should advise such patients on how to modify their activities and work station (ergonomic compliance). Simple changes in workflow are often sufficient to control mild symptoms.
Friends, on February 13-14 in Moscow there will be a seminar by Anna Ovsyannikova “Fundamentals of anatomy and biomechanics of the hand. Diseases and injuries of the hand and fingers." Find out more...
Manual therapy techniques include mobilization of the soft tissue, carpal bones, and median nerve. Orthotics can also be performed.
Other methods may include ultrasound and electromagnetic field therapy.
Research results (vary):
- Physiotherapy modalities such as transcutaneous electrical stimulation and ultrasound have little effect on sensory deficits.
- The evidence for the effectiveness of exercise and mobilization techniques is limited and of very low quality.
- Data on postoperative rehabilitation are also limited. None of the proposed interventions appears to have a predominant advantage.
Reasons for the development of the syndrome
Carpal tunnel syndrome disease develops under the influence of several factors. A decrease in the diameter of the carpal tunnel may occur due to compression of the nerve. Swelling of surrounding tissues and for both reasons simultaneously. The root cause is trauma, both one-time and microtrauma inflicted regularly due to lifestyle or work activity.
1. “Dangerous” professions.
Among the professions at risk:
- drummers;
- programmers;
- gamers;
- artists;
- pianists;
- secretaries;
- sign language interpreters;
- seamstresses;
- engineers;
- assembly line workers and others.
Most often, the syndrome is diagnosed in women over 40 years of age, mainly due to their professional choice and hormonal changes in the body. However, the disease can occur at any age.
2. Accompanying illnesses.
- A number of medical conditions increase the risk of developing carpal tunnel syndrome, including:
- Injuries, dislocations, fractures, causing hematomas and swelling.
- Neoplasms, tumors of ligaments and tendons.
- Frequent intratunnel pressure and swelling of the limbs.
- Chronic heart failure and other diseases of the heart and blood vessels.
- Diabetes mellitus, thyroid diseases and other endocrine pathologies.
- Obesity, regardless of the causes of its occurrence.
- Chronic arthritis, sclerosis, collagenosis and vasculitis.
- Tuberculosis and non-tuberculous bacterial infections.
- Kidney failure.
- Alcoholism, smoking, drug use.
3. External factors.
- Work in low temperature conditions. For example, fishermen, butchers, public utility workers.
- Working with heavy tools and vibrating devices. For example, builders, repairmen, industrial workers.
Any of the listed effects or a number of factors together causes a narrowing of the carpal tunnel and pathology develops. Most often, the disease develops according to the following scheme: trauma - aseptic (non-infectious) inflammation, spreading to the carpal tunnel - swelling of the subcutaneous fat layer. Then everything goes around in a new circle:
increasing pressure on nerves and blood vessels leads to even greater trauma and inflammation, causing progression of the disease and transition to the chronic stage.
Causes
Tunnel syndromes are a polyetiological disease. The main reasons contributing to the development of compression/compression-ischemic neuropathies include:
- Injuries.
- Long-term microtraumatization of nerve fibers due to professional activities.
- Features of the anatomical structure (narrowness of the canals caused by the presence of bone processes/tendon constrictions).
- Congenital (hereditary) anomalies (fibrous bands, accessory muscles, bone spurs, etc.). endocrinopathies ( hypothyroidism , diabetes mellitus , acromegaly ).
- Hormonal disorders ( puberty , andro / menopause , pregnancy / lactation , hormonal contraception).
- Genetically determined (innate susceptibility to various adverse factors of peripheral nerves).
- Metabolic disorders ( hypovitaminosis , nutritional starvation , atrophy of subcutaneous fatty tissue).
- Diseases/systemic blood diseases ( systemic lupus erythematosus , myeloma , gout , rheumatoid arthritis , periarteritis nodosa , sarcoidosis , amyloidosis , etc.).
- Infections ( diphtheria , tuberculosis , syphilis , paratyphoid , AIDS , botulism , measles , etc.).
- Tumors/paraneoplastic processes ( neurofibromatosis ).
- Industrial/household intoxications (thallium, organophosphorus compounds, mercury, manganese, arsenic, household poisons).
The development of carpal tunnel syndrome is promoted by:
- Trauma accompanied by wrist fractures, tendon sprains/local swelling / hematoma .
- Factors contributing to changes in carpal tunnel anatomy: osteoarthritis / post-traumatic arthritis .
- Chronic (long-term) microtraumatization of the median nerve.
- Conditions/diseases accompanied by metabolic disorders, tendon and bone deformities ( acromegaly , rheumatoid arthritis , hypothyroidism , diabetes mellitus , pregnancy , amyloidosis , vitamin deficiency , alcoholism , poisoning with toxic substances).
- Mass formations directly on the median nerve ( schwannoma / neurofibroma ) or in the wrist area ( lipoma / hemangioma ).
Instrumental/laboratory diagnostics
Laboratory tests
There are no blood tests to diagnose carpal tunnel syndrome, but they may be ordered to screen for underlying conditions (such as diabetes or rheumatoid arthritis).
Radiation diagnostics
Radiation diagnostics is not used in routine practice.
MRI of the wrist may be useful in preoperative preparation to identify the causes of mechanical compression of the median nerve. Changes in the MR signal can be observed with chronic nerve compression, but they do not yet have practical significance for determining treatment tactics for the disease.
Many specialists now use ultrasound in addition to electrophysiological research methods. Ultrasound can reveal pathological processes that occupy space in the carpal tunnel, confirm changes in the median nerve (increase in cross-sectional area), which really help in diagnosis.
Electroneurophysiological studies
Electroneuromyography is the first-line diagnostic tool for carpal tunnel syndrome. Abnormalities found on ENMG in combination with specific symptoms and tests are the key to the correct diagnosis. Electroneuromyography can also exclude other neurological disorders.
Electrophysiological studies can also determine the extent of nerve damage, which is an objective criterion for prognosis.
Carpal tunnel syndrome is usually divided into mild, moderate and severe. The ranges for these groups may vary depending on the laboratory. In general, patients with isolated sensory disorders belong to the mild group, and if motor dysfunction occurs, they move to the moderate group. Confirmation of axonal damage (markedly decreased or absent sensory/motor response distal to the carpal tunnel) indicates severe disease.
Tracking the dynamics during ENMG helps determine the further approach to the disease.
Other quantitative tests, such as thermography or vibrometry, are less informative compared to ENMG and are not recommended for practical use.
Surgery
Sign up for a consultation
In patients for whom conservative therapy has failed, or for those who initially come to the appointment with a severe degree of carpal tunnel syndrome (according to ENMG), there are indications for surgery. Surgical dissection of the palmar ligament is highly likely (more than 90%) to lead to significant improvement with a low complication rate. The success of surgical treatment is reduced for people with normal electromyography.
Carpal tunnel decompression surgery is performed under local anesthesia in an outpatient operating room. This operation does not require hospitalization or the participation of an anesthesiologist.
The operation can be performed using a classic wide approach, as well as minimally invasive with or without the use of endoscopic equipment. The long-term results of a correctly performed operation are comparable for different methods of intervention.
The details of the surgical intervention and its necessity in your case should be discussed with a hand surgeon.
General overview
Carpal tunnel syndrome (carpal tunnel syndrome) is a set of characteristic symptoms that occur when the median nerve is compressed in the wrist, ICD-10 code: G56.0. Includes numbness, paresthesia and pain in the zone of innervation of the median nerve. These sensations may be accompanied by objective changes in sensitivity and strength in the hand.
Diagnostics
The first line of diagnosis for numbness of the fingers in our clinic is electroneuromyography, this is especially true for carpal tunnel syndrome. To make a diagnosis, a combination of characteristic clinical signs and deviations from the norm found during electroneuromyography is necessary. Electrophysiological testing can also exclude other neurological problems (for example, in the cervical spine). With this study, it is possible to assess the severity of nerve damage, which helps in choosing further treatment tactics and determines the prognosis of the disease. An ultrasound scan can reveal masses that are putting pressure on the nerve.
MRI for carpal tunnel syndrome is prescribed exclusively for preoperative planning in cases of significant joint damage or neoplasms.
Treatment
There is evidence of the benefits of aerobic exercise and weight control in carpal syndrome. A bicycle or exercise bike is not the best exercise option, as it puts constant stress on your arms.
Using physical therapy such as ultrasound may provide temporary relief.
Many people with incipient syndrome (as measured by ENMG) usually respond well to the use of a night splint to maintain a neutral hand position during sleep (minimum three weeks).
Injection (blockade) with glucocorticoids, such as diprospan, shows good results if more conservative means do not work.
Patients who do not respond to conservative methods, or those who initially present with severe disease, are referred for surgical treatment.
Surgery for carpal tunnel syndrome (CTS) involves cutting the palmar ligament, which is compressing the median nerve. The success rate is very high (more than 90%), and the risk of complications is minimal. Recurrence after complete dissection of the palmar ligament of the hand is extremely rare. Surgical success is less likely for patients with normal electroneuromyography findings.
Epidemiology
Disease frequency
The most accurate statistics are for the United States of America, where about 1–3 new cases of the disease are registered per 1000 people per year. On average, about 50 people out of 1000 suffer from carpal tunnel syndrome.
There is some lack of international statistics on this issue, but the prevalence of the syndrome in developed countries is similar to the United States, for example, in Holland there are about 2.5 new cases per year, and in the UK about 70-160 out of a thousand people ever seek help. Carpal syndrome is practically unheard of in developing countries, for example, among the indigenous population of South Africa.
Mortality/health threat
The disease is not fatal and cannot lead to a fatal outcome, but it can lead to serious irreversible impairment of hand function if correct treatment is not carried out.
It occurs more often in white Caucasian people.
It is believed that women suffer from carpal tunnel syndrome three times more often than men.
Peak occurrence occurs between 45–60 years. Only 10% of patients with this diagnosis are under 31 years of age.