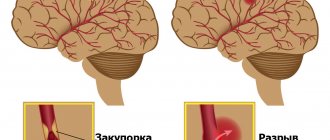
Trigeminal neuropathy (trigeminal neuralgia) is a chronic pain syndrome that involves the trigeminal (5th cranial nerve). Trigeminal neuropathy is a type of neuropathic pain (pain associated with injury or damage to a nerve). The usual or “classic” form of the disease (the so-called “Type 1”) is characterized by attacks of intense pain in the form of a burning sensation or shock that last from a few seconds to two minutes. These attacks can occur in group episodes lasting up to two hours. The “atypical” form of the disease (the so-called “Type 2”) is characterized by constant aching, burning, stabbing pain of somewhat less intensity than with type 1. Both forms of pain can occur in the same person, sometimes at the same time. The intensity of pain can lead to disability, both physical and mental.
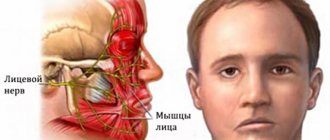
The trigeminal nerve is one of 12 paired nerves that exit the brain. The nerve has three branches that carry sensory sensations from the upper, middle and lower parts of the face, as well as the mouth, to the brain. The ophthalmic or superior ramus provides sensory sensation to most of the face, forehead, and front of the head. The maxillary or middle branch provides sensation to the cheek, upper jaw, upper lip, teeth and gums, and side of the nose. The mandibular or inferior branch innervates the lower jaw, teeth and gums, and lower lip. With trigeminal neuropathy, more than one branch may be affected. In rare cases, there may be manifestations of neuropathy on both sides at different times. Even less common is bilateral involvement.
Trigeminal neuropathy occurs most often in people over 50 years of age, although the condition can occur at any age, including in infants. The possibility of developing trigeminal neuropathy increases slightly with multiple sclerosis when it occurs in young people. The rate of new cases is approximately 12 per 100,000 people per year; the disease is more common in women than in men.
Clinical picture of osteomyelitis of the tooth socket
The clinical picture of osteomyelitis of the tooth socket is characterized by complaints of acute throbbing pain both in the area of the socket and in the area of neighboring teeth. General symptoms such as weakness, hyperthermia, headache, chills, impaired performance and sleep are also observed. Swelling of the perimandibular soft tissues develops, the submandibular lymph nodes are enlarged, dense, painful on palpation.
With osteomyelitis of the socket of only one molar of the lower jaw, the inflammatory process can spread to the area of the masseter or medial pterygoid muscle, which, in turn, can cause difficulty opening the mouth. When examining the oral cavity, the doctor may detect a dirty gray coating on the bottom and walls of the socket. You can also smell a specific smell. Percussion of adjacent teeth is painful.
The mucous membrane in the area of the transitional fold is hyperemic and swollen. Palpation of the alveolar process from the buccal and oral sides is sharply painful both in the area of the socket and adjacent teeth.
The acute phase of inflammation lasts about 6–8 days, sometimes 10 days. Then the inflammatory phenomena decrease, the process becomes chronic. The general condition improves, body temperature decreases. Swelling and hyperemia of the mucous membranes also decrease, and then pain on palpation of the alveolar process, swelling of facial tissues and submandibular lymphadenitis disappear. After 12–15 days, the tooth socket is filled with loose, pathological granulation tissue, sometimes bulges out of the socket, and pus can be released when pressure is applied.
On the x-ray we see fuzzy blurred contours of the compact lamina of the alveoli; osteoporosis and bone destruction in the alveolar region are pronounced. In rare cases, after 20–25 days from the beginning of the acute period, it is possible to identify small sequesters.
Causes of limited osteomyelitis of the socket
1. as a complication of alveolitis. 2. as a result of decreased immunity
Signs of trigeminal neuralgia
A characteristic symptom of this disease is a short-term sharp, burning pain, similar to an electric shock. It can be triggered by any movement, for example:
- facial expressions during a conversation;
- when brushing your teeth;
- touching particularly sensitive (trigger) areas.
Attacks of trigeminal neuralgia are often accompanied by facial twitching and convulsive contractions of the muscles of the masticatory apparatus. Signs of the disease also include salivation and lacrimation. If such signs occur, you should contact a neurologist.
Treatment of socket osteomyelitis
In the acute stage of the disease, therapy begins with revision of the hole. Under conduction or infiltration anesthesia, the tooth socket is cleaned of remnants of a blood clot, food and pathological tissue. Then the well is washed from a syringe with a weak antiseptic solution or a biologically active drug. The following drugs are used: staphylococcal and streptococcal bacteriophage, proteolytic enzymes, lysozyme. After this, a bandage with Alvogyl is applied to the wound.
To reduce inflammation and pain, dissection of the infiltrated area of the mucous membrane and periosteum is performed. An incision is made along the transitional fold 1.5–2 cm long, as well as an incision on the inside of the alveolar process. Drug therapy is prescribed: antibiotics, sulfa and antihistamines, analgesics, physical therapy (UHF, ultrasound, helium-neon laser). To increase specific immunological reactivity, phagocytosis stimulants are prescribed: pentoxyl, methyluracil, milife, lemongrass.
After relief of acute inflammation, treatment with multivitamins and stimulants of nonspecific resistance of the body is continued (methyluracil 0.5 g or pentoxyl 0.2 g 3-4 times a day, sodium nucleinate 0.2 g 3 times a day, milife 0.2 G). Concomitant ultrasound or laser therapy of the inflammation focus is necessary. Approximately 20 days from the onset of the acute inflammatory process, if the wound has not healed and sequesters are found on the radiograph, pathological granulations and small sequesters are removed with a surgical spoon, the walls and bottom of the hole are scraped out. The wound is washed with an antiseptic solution, dried and loosely packed with gauze soaked in iodoform liquid.
Dressings (treating the hole with an antiseptic solution and changing the iodoform gauze in it) are done every 2-3 days until young granulation tissue forms on the walls and bottom of the hole.
Prevention of socket osteomyelitis is the same as for alveolitis.
- Before the intervention, professional oral hygiene is necessary
- the doctor must inspect the socket and perform hemostasis by compression
- if more than two teeth are removed, apply sutures
- After tooth extraction, it is necessary to give clear recommendations to the patient
If, nevertheless, the appearance of alveolitis could not be avoided, and the patient complained of pain, it is necessary to stop the process as quickly as possible. Therefore, the patient must be informed about possible complications and motivated not to delay visiting the dentist if he experiences pain.
Surgical (operative)
In fact, at the moment this is the only method aimed at eliminating the problem, not its symptoms. It is used when conservative treatment does not bring results. The most commonly used types of surgical treatment are:
- Microvascular decompression is the separation of a blood vessel from the nerve it compresses using microsurgery. The disadvantage of this method is that it is highly traumatic.
- Percutaneous stereotactic rhizotomy is the destruction of tissues by high temperature, when a high-frequency electric current is passed through them.
- Percutaneous glycerol rhizotomy - glycerin injections that destroy the nerve.
- Percutaneous balloon compression - compression of nerve fibers using an inserted balloon.
- Stereotactic radiosurgery (gamma knife) is a non-invasive method that involves ionizing radiation to part of the trigeminal nerve.
It should be borne in mind that surgical methods are effective in the early stages of the disease, and the effectiveness depends on the duration of the disease and the extent of the lesion. Advanced trigeminal neuralgia can lead to decreased hearing and weakening of the facial muscles, so you should not postpone a visit to a neurologist.
Trigeminal neuritis
Today, traumatic neuritis of the trigeminal nerve is considered one of the most common causes of pain syndromes in the maxillofacial area.
As a complication, it occurs during the removal of permanent molars of the lower jaw, due to damage to the lower alveolar nerve in the mandibular canal. The apices of the roots of the lower molars are in close proximity to the mandibular canal and in some cases may be located in the canal itself. Sometimes, due to chronic apical periodontitis, the bone between the root apex and the wall of the mandibular canal is resorbed. When a tooth is loosened by an elevator, the lower alveolar nerve can be injured, which will lead to partial or complete disruption of the functions of the third branch of the trigeminal nerve. The result is pain in the jaw, numbness of the lower lip and chin, decreased or absent sensitivity of the gums, decreased electrical excitability of the dental pulp on the affected side. Usually all these phenomena gradually disappear after a few weeks.
Electroodontometry
Electroodontometry is the most effective method for assessing the functional state of the trigeminal nerve when it is damaged. EDI is based on a study of the reaction of the teeth of the lower jaw to electrical stimulation. The method is performed on all teeth of the lower jaw, with preserved pulp both in the affected area and on the opposite healthy side.
S.N. scale Fedotova (1997) to assess the severity of damage to the inferior alveolar nerve based on electrical odontometry data:
- mild degree - reaction of teeth with preserved pulp on the side of nerve damage within 20-40 μA;
- moderate severity – reaction of teeth to currents from 40 to 100 µA;
- severe degree - complete loss of pain sensitivity, reaction of teeth to currents above 100 μA
The use of EDI to diagnose traumatic injuries of the inferior alveolar nerve is impossible if:
- lower jaw teeth endodontically treated
- lower jaw teeth are covered with orthopedic structures
- metal elements of splinting structures are fixed on the teeth
- missing teeth
Locations for measuring electrical excitability of facial skin
Assessment of the area of paresthesia in traumatic neuritis of the inferior alveolar nerve
The zone of paresthesia is identified - impaired sensitivity of the skin based on a tactile test, photographed, followed by an assessment of the area of the paresthesia zone: points are drawn on the border of areas of normal sensitivity of the skin, the red border of the lips and the paresthesia zone, which are then connected by a continuous line. Zones of hyper-, hypo- and anesthesia were marked with different colors.
I - vertical lines:
- midline,
- a line passing through the outer edge of the philtrum,
- a line passing through the outer edge of the wing of the nose,
- pupil line;
II - horizontal lines:
- lip line,
- a line running along the lower edge of the red border of the lips,
- the border line between the chin and lower lip,
- a line drawn along the most protruding part of the chin,
- line of the border of the chin and submental areas.
Schematic representation of the areas for measuring facial skin paresthesia.
Each of the 12 resulting squares was assigned a score depending on the nature of the sensitivity disorder:
0-sensitivity is not impaired;
1-skin hyperesthesia
2-hypoesthesia of the skin;
3-anesthesia of the skin.
Next, the sum of points was calculated and divided by 12 (quadrants).
With the results:
3.0-2.1 – severe sensitivity impairment was diagnosed;
2.0–1.1 – moderate severity;
less than 1.0 – mild severity of the pathology being studied
Diagnostics
The diagnosis of trigeminal neuropathy is based primarily on the patient's medical history, symptoms, and physical and neurological examination findings. To make a diagnosis of NTN, it is necessary to exclude other diseases that may manifest as pain in the facial area. Some conditions that cause facial pain include: post-herpetic neuralgia, headaches, and temporomandibular joint disorders.
Due to the commonality of symptoms and the large number of conditions that can lead to facial pain, making a correct diagnosis is often difficult, but finding out the exact cause of the pain is very important, since treatment tactics for different types of pain may differ.
Most NTN patients will eventually need to undergo a magnetic resonance imaging (MRI) scan to rule out a tumor or multiple sclerosis as the cause of the pain. This test method can clearly show the compression of a nerve by a blood vessel. Special MRI techniques can reveal the presence and degree of compression of a nerve by a blood vessel.
The diagnosis of classic trigeminal neuropathy can also be confirmed by the positive effect of taking anticonvulsant medications for a short period of time. Diagnosis of T2 is more complex and difficult, but is usually confirmed by a positive response to low-dose tricyclic antidepressants in the same way as other neuropathic pain.
Treatment of neuritis
Treatment of neuritis in traumatic injuries must be timely and wait-and-see tactics are unacceptable. For mild damage to the inferior alveolar nerve, decongestant therapy (prednisolone, veroshpirone) is sufficient. In case of moderate severity of damage, drugs that improve the conductivity of the nerve trunk (neuromedin) are added to decongestant therapy. In case of severe damage to the nerve trunk, in the absence of positive dynamics in the restoration of sensitivity within 4 months, the patient should be referred for a consultation with a neurosurgeon in order to resolve the issue of the possibility of restoring the anatomical integrity of the nerve trunk.
Various reflexotherapy methods are widely used in the complex treatment of diseases of the peripheral nervous system. In the complex treatment of diseases of the peripheral nervous system, reflexology methods such as electroacupuncture and transcutaneous electrical neurostimulation are widely used.
Prevention of neuritis
Prevention of neuritis of the inferior alveolar nerve is the correct technique for removing teeth, correct diagnosis and correct reading of the radiograph, and a gentle technique for dislocating the roots of teeth in the lower jaw with an elevator.
Factors influencing neurological response to nerve injury
— Preoperative screening for neuropathic pain is necessary. Preexisting neuropathic dental pain (PDAP type 1), which exists before surgery, can be caused by many different systemic conditions, medications, and other lesions. It is critical that surgeons recognize presurgical neuropathic conditions because neuropathic pain does not respond to surgery and can often lead to worsening pain. In addition, poorly controlled preoperative pain and nerve damage can cause chronic postoperative pain.
— The main indicators for predicting chronic post-surgical pain are psychological factors, including the level of anxiety, neuroticism (a fundamental personality trait in psychology, characterized by anxiety, fear, rapid mood swings, frustration and a feeling of loneliness. It is believed that neurotic people cope worse with stress and are prone to exaggerate the negative side of a particular situation.), catastrophization and introversion. Thus, the doctor has the opportunity not to perform the surgery of choice (implantation) in such patients, but to decide in favor of an alternative treatment plan.
- The concentration of the anesthetic used is up to 2% lidocaine - the accepted standard, because higher concentrations have a greater neurotoxic effect, which may cause permanent neuropathy. Avoid using multiple (repeated) anesthetic blocks in the same area for the same reason.
— Preoperative medical examination should exclude the following diseases : Raynaud's disease, Erythromelalgia (Mitchell's disease), Irritable bowel syndrome (IBS), Migraines, Fibromyalgia.
—Location of surgery is another factor associated with neurological response. Trauma in the distal jaw is more significant (eg, angle and ramus) than in the mental foramen, because the closer the proximal nerve injury is, the greater the risk of damaging trigeminal ganglion cells and initiating retrograde effects of differentiation into the central nervous system. .
Thus, a thorough interview and examination of the patient, detailed pre-implantation planning based on CBCT data, appropriate visualization of the implantation plan and the use of surgical guides, selection of optimal implant sizes with extended safety zones, use of drill limiters and, of course, an experienced team of doctors who will carry out the implantation followed by early postoperative care, all of which will contribute to safer practice and optimized patient outcomes.
Abscess after tooth extraction
An abscess after tooth extraction is a long-term complication of a tooth extraction operation that occurs as a result of contamination of the wound surface with microorganisms. When teeth are removed, not only the tissues surrounding the tooth can be injured, but also the mucous membranes of the mouth and cheeks. A fresh wound is a favorable environment and entry point for microorganisms. Therefore, under appropriate circumstances, an abscess may form in the soft tissues or in the hole, which over time and without treatment can “spill” with the formation of phlegmon in several areas.
Causes of abscess
The cause of an abscess may be failure to comply with the rules of asepsis and antisepsis directly during the tooth extraction operation. As a result of incorrect actions by the doctor, infection occurs in the tooth socket and subsequent suppuration. Also, infection of the socket and soft tissues can occur due to the fault of the patient himself if he does not follow all the dentist’s recommendations. The patient must strictly follow the prescribed procedures, otherwise repeated surgery cannot be avoided.
Prevention and treatment of tooth abscess
Prevention of the appearance of an abscess after tooth extraction is basic regular oral hygiene and following all the recommendations of the dentist. Also, preventive measures include visiting the dentist if you experience pain within a few days after tooth extraction. Treatment of an abscess consists of opening and cleaning the abscess cavity, removing purulent formations and prescribing anti-inflammatory therapy. Sometimes the abscess opens on its own, and the pain disappears. But this does not mean that the process has been stopped, so further treatment by a dentist is necessary. Otherwise, the infection may spread to contact areas and intensify the process.
Causes of the disease and its types
The disease is conventionally divided into two types - idiopathic (primary), which occurs independently, and symptomatic (secondary) - a complication of another disease. The main causes of trigeminal neuralgia are:
- hypothermia;
- injuries received;
- various infectious diseases (tuberculosis, syphilis, herpes, etc.);
- pathologies of nearby blood vessels;
- eye, dental and otorhinolaryngological diseases;
- oncological diseases.
Clinical algorithm for determining post-traumatic neuropathy
Trigeminal Neuropathy Assessment Questionnaire
Important! Severe pain experienced during treatment may indicate a possible nerve injury.
- History of the initial onset of pain.
- Development of pain.
- Duration of pain.
- History of regular pain SOCRATES (Site, Onset, Character, Radiation, Associated signs, Timing, Exacerbating and relieving factors, Severity) - Localization, Occurrence (frequency of attacks), Character, Irradiation, Associated symptoms, Duration, Exacerbation and relief factors (what intensifies and relieves pain), severity of pain.
- Psychological screening.
- Functional screening (impact on daily life).
Mechanosensory tests (mapping the affected area)
A protocol for examining the dermatome to assess the extra-oral mechanosensory function of the alveolar branch of the trigeminal nerve.
Dermatomes are segments of skin into which the entire surface of the human body is divided in connection with its innervation by various roots of the spinal cord, in this case the trigeminal nerve.
Figure 7. Dermatomes of the branches of the trigeminal nerve
1. Logging the affected area.
Using surgical forceps, move from the normal to the neuropathic (changed) area, warning the patient that there may be increased sensitivity and/or decreased sensitivity. Mark an area on the patient's face with marker marks and take a photo. Assess the % or area of the extra-oral dermatome that is affected by neuropathy.
2. Recording the assessment of subjective sensation.
Press the surgical forceps or probe firmly (but not painfully) against the patient's arm several times at intervals (5 times per minute), explaining that this is a "normal" subjective rating of function on a scale of 10 out of 10. Press with the same pressure on the unaffected side of the face or tongue and repeat the stimulation, explaining that it should be 10 out of 10. Then remove the forceps or probe and explain that the missing stimulation is 0 out of 10. Only then repeat the same actions in the area of neuropathy that you have already confirmed and marked with markers labels, and ask the patient to report the stimulus level out of a possible 10 (if >10 = hyperesthesia and <10 = hypoesthesia). This test should be repeated in different areas of the neuropathy (lip border, lip skin, chin, tongue, etc.)
3. Recording the light touch assessment
To assess light touch thresholds, it is recommended to use a frayed cotton swab, repeating touches at intervals of 5 times per minute. First on the unaffected side and then repeating on the affected side, ask the patient to report the differences. If the patient is experiencing numbness, then the stimulation will have a reduced threshold for detecting light touch, however, if the patient suffers from hyperesthesia and possible allodynia (pain to touch), then this test can be very uncomfortable and irritating.
Dermatomal Involvement Map Interpretation and Neuropathy Assessment —Does the area of neuropathy correspond to the dermatomal area in which surgery was performed? — Dynamics of the area of the involved extraoral and intraoral area when mapping neuropathic areas (criterion reliability is low)
Important! Localized sensory neuropathy is not always present in patients, but there is almost always an area of abnormal sensation, and the patient's maximum pain is associated with the area of sensory deficit, that is, suffering from a combination of pain, numbness and altered sensation. This is an important diagnostic distinction for sensory neuropathy.
Subjective function
- Is neuropathy hyperesthesia or hypoesthesia?
- Thermal allodynia test is the occurrence of pain when exposed to heat or cold. Thermal allodynia, especially cold allodynia, is a feature in patients with trigeminal nerve damage.
- Thermal hyperalgesia test. Increased pain that occurs after a weak stimulus.
- Test "Direction of movement". The patient closes his eyes, the doctor uses a soft brush to determine the patient's ability to detect both the sensation and the direction of movement of the brush.
- Test for sensitivity to temperature stimuli. A cotton swab with cold test spray and a dental mirror handle heated to 43 - 45 ° C are used to determine the patient's ability to feel cold and heat. Alternatively, test tubes can be filled with hot (43 -45 °C) water and cold water.
There are WHO recommendations regarding which parameters of peripheral sensory consequences should be taken into account to predict the results of microsurgical restoration of a damaged sensory nerve. Zuniga JR and Yates DM adapted the recommendations to trigeminal nerve lesions. More details here: Zuniga JR and Yates DM Factors Determining Outcome After Trigeminal Nerve Surgery for Neuropathic Pain. J Oral Maxillofac Surg 2021 Jul;74(7):1323-9.
Today, a guideline for mandatory X-ray monitoring after endodontic treatment and dental implantation surgery has already been adopted in order to indicate the relationship between the root and the root filling, as well as the proximity of the implant bed and/or the implant itself to the canal of the inferior alveolar nerve. Intraoral dental radiography is considered to be sufficient to detect iatrogenicity, although post-traumatic neuropathy is primarily a clinical diagnosis.
Renton T, Yilmaz Z. Managing iatrogenic trigeminal nerve injury: a case series and review of the literature. Int J Oral Maxillofac Surg 2012 May;41(5):629-637.
Prevention
Prevention measures:
- balanced diet;
- limiting alcohol consumption, quitting smoking, reducing factors that lead to intoxication of the body;
- active sports;
- do not overcool;
- increase stress resistance;
- avoid injury;
- timely treatment of respiratory and infectious diseases;
- preventive examination at the dentist several times a year, dental treatment;
- timely contact a neurologist if pain occurs.