Neuroma is a neoplasm of benign etiology, growing from Schwann cells (lemmocytes), which form the myelin sheath of nerve fibers. It most often affects the auditory nerve, but can occur on any other nerves. It is diagnosed in 10% of cases of cerebral neoplasms, 20% of spinal canal tumors and 50% of cases of peripheral nerve tumors.
Treatment of neuroma is surgical. The Neurosurgery Department of CELT invites you to undergo an operation to remove it in Moscow. We have been working in the market of paid medical services for more than thirty years and provide treatment in accordance with international standards. Our neurosurgeons have modern equipment and gentle techniques in their arsenal, the selection of which is carried out individually, which allows us to achieve the best results.
At CELT you can get advice from a neurosurgeon.
- Initial consultation – 3,000
- Repeated consultation – 2,000
Make an appointment
General information about pathology
Disease:
- occurs infrequently;
- proceeds slowly;
- rarely becomes malignant;
- occurs in people who are at least 35-40 years old;
- more often affects females.
The neoplasm externally resembles a rounded dense nodule, which is located in a capsule formed from connective tissue. Thanks to this, it is relatively easy to get rid of the tumor using surgery.
Neuroma - causes of occurrence
Morton's neuroma
Morton's neuroma, or compressive neuropathy of the interdigital nerve, is not a true tumor; it is a reactive thickening of the nerve and surrounding tissues that develops as a result of its compression. Interdigital neuroma, or Morton's neuroma, named after Thomas George Morton, was first described by Civinini in 1835, and later Durlacher in 1845 fully described its symptom complex.
Schematic representation of Morton's neuroma.
Morton's neuroma is most common in women (male to female ratio 1:9) of middle age. Most often it affects the 2nd and 3rd intermetatarsal nerves between the heads of the 2nd-3rd and 3rd-4th metatarsal bones. Presumably associated with compression of the intermetatarsal nerve by the intermetatarsal ligament (deep transverse ligament of the foot), located to the rear surface of the nerve. The third intermetatarsal space receives double innervation from the external and internal plantar nerves, which serves as an anatomical prerequisite for nerve injury in the third intermetatarsal space.
Pain in the third intermetatarsal space, aggravated by walking and wearing tight shoes, especially high-heeled shoes. The pain often subsides or goes away completely when shoes are removed and the foot is massaged. Numbness is often felt along the plantar surface of 3-4 toes. Sometimes it is possible to palpate the neuroma. A provoking test can be transverse compression of the foot, which often detects increased pain. Sometimes you can hear a “click” (Mulder’s sign), and instability in the metatarsophalangeal joints can also be detected.
Although the diagnosis of Morton's neuroma is usually made on the basis of clinical data, if the diagnosis is doubtful, instrumental diagnostic methods are resorted to. X-rays often do not reveal pathology, although bone usuration may be detected at the site of compression by the neuroma. Sonography shows an oval hypoechoic formation. MRI is rarely used, more often for differential diagnosis in cases of an unclear clinical picture.
For diagnosis, therapeutic and diagnostic blockade of the intermetatarsal nerve with a local anesthetic solution is also often used. If the pain syndrome completely regresses, this is considered a convincing sign in favor of intermetatarsal neuroma.
Differential diagnosis of Morton's neuroma is carried out with such diseases as: synovitis of the metatarsal joint, metatarsalgia, stress fractures of the metatarsal bones, arthritis of the metatarsal joints, osteonecrosis of the heads of the metatarsal bones, tumor lesions of the bone, diseases of the lumbar spine with irradiation of pain in the intermetatarsal spaces .
For the conservative treatment of Morton's neuroma, the use of special shoes with a wide forefoot, a rigid sole to prevent rolling of the foot, and a soft cushion under the heads of the metatarsal bones is of greatest importance. In 20% of cases, the use of such shoes leads to complete regression of symptoms.
If replacing shoes does not bring relief, the next step is to inject a glucocorticosteroid directly into the area of the neuroma. Unfortunately, this technique rarely achieves pain resolution for a long period of time.
If conservative treatment is ineffective, neurectomy is used. It can be performed from both dorsal and plantar approaches.
Schematic illustration of the dorsal surgical approach used to remove an interdigital neuroma.
An alternative method is dissection of the intermetatarsal ligament, but this technique is more effective in the early stages of the disease.
On the left is a classic dorsal approach, the deep transverse intermetatarsal ligament is visible, on the right is Morton’s neuroma after its removal.
To prevent the formation of a true neuroma at the site of Morton's neuroma, it is recommended to perform a full resection and immerse the proximal end of the nerve into the own muscles of the foot.
After surgical treatment of Morton's neuroma Excellent results were observed in 45% of cases, good in 32%, satisfactory in 15%, poor in 8%. Unsatisfactory results are often associated with the formation of a true amputation neuroma in the region of the proximal end of the intermetatarsal nerve.
Neuroma is caused by:
- genetic factors.
The likelihood of a tumor increases sharply if relatives suffered from this problem;
- difficult environmental situation
– exposure to harmful chemicals, radiation;
- cigarette addiction
.
Also, a neoplasm appears in people already suffering from another neoplasm.
Types of pathology
There are the following main types of disease:
Acoustic neuroma (aka vestibular schwannoma):
- occurs most often;
- the tumor affects the auditory nerve (usually the vestibular part, rarely the cochlear part). However, the neoplasm gradually grows and begins to penetrate the cerebelloptine angle;
- vestibular schwannoma can harm the facial nerve and even “reach” the trigeminal nerve. The optic and jaw nerves may also be affected;
- The tumor progresses very slowly (by a few millimeters per year). In rare cases, rapid, dangerous growth is observed (up to 30 mm in 12 months), due to which important parts of the brain (primarily the cerebellum) begin to be compressed;
- much more often it develops in only one ear (in two 5% of cases). Bilateral acoustic neuromas are usually caused by neurofibromatosis.
- appears at 40-50 years of age.
Vertebral neuroma:
- usually develops in the thoracic and cervical areas of the back;
- sometimes appears in the lumbar region;
- It is less common than acoustic, but also quite common.
Morton's schwannoma:
- this type of pathology appears on the foot (more precisely, its sole) of one leg, in the area of the 3rd and 4th toes;
- in rare cases, pathology develops on both feet;
- Morton's schwannoma is rare.
Development of neoplasm
In medicine, 2 classifications of this disease are used. According to KOOS there are 4 stages:
- the tumor is located in the internal auditory canal;
- extends into the cerebellopontine angle, increases to 20 mm in diameter;
- extends to the brain stem, but does not put pressure on it, reaches 21 - 30 mm;
- puts pressure on the brain stem, the size of the formation is more than 30 mm.
The famous neurosurgeon Majid Samii divided stages 3 and 4 into subsections:
- T3a – tumor fills the cerebellopontine cistern;
- T3b – spreads to the brain stem;
- T4a – causes its compression;
- T4b - grossly deforms the trunk and IV ventricle.
How does pathology manifest itself?
Often the disease is completely asymptomatic and is discovered by chance. This makes it difficult to treat neuroma. Signs of pathology depend on the location of the tumor:
For acoustic neuroma:
- tinnitus (tinnitus) develops;
- hearing deteriorates;
- coordination is impaired;
- severe dizziness appears.
If the facial nerve is damaged:
- tears flow;
- dry mouth;
- There is partial paralysis of the eyelids.
With neuroma of the dorsal vertebrae the following are observed:
- excruciating pain in the back;
- deterioration of sensitivity at the site of the lesion.
4. Morton's schwannoma causes various sensory problems:
- numbness is felt in the area of the feet;
- paresis occurs.
Symptoms of acoustic neuroma
How the disease manifests itself depends on its stage. While the tumor is small, the patient is bothered by vestibular disorders, and hearing loss may occur. As it grows, the tumor begins to put strong pressure on the brain stem. Nystagmus (involuntary movements of the eyeballs, accompanied by decreased vision), balance disorders, and impaired coordination of movements may appear. When the tumor has grown, it puts extreme pressure on the cerebral structures. Difficulties with swallowing appear, vision decreases to the point of blindness, and hydrocephalus progresses.
How is pathology diagnosed?
Treatment of neuroma is preceded by diagnosis. It is produced using:
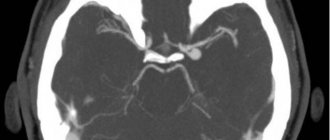
- computer or magnetic resonance imaging examination. Magnetic resonance imaging is more effective. It is able to detect microscopic tumors, while computed tomography diagnostics detects only tumors whose diameter is at least 1 cm;
- electroneurography;
- audiograms (hearing test).
Treatment of the disease – surgical, radiation, conservative
Usually the neuroma must be removed; conservative treatment is not always effective. True, in the early stages, the tumor can actually be removed using radiation therapy (cyberknife).
Operation
Surgical treatment of neuroma involves a local opening of the skull (trepanation) so that the tumor can be reached.
It will not be possible to do without surgical intervention if:
- the tumor quickly increases in size (for example, after the patient has undergone radiotherapy);
- the disease began to lead to serious complications.
Surgical tumor removal is contraindicated if:
- the patient has problems with the heart or blood vessels;
- The patient is already elderly and has heart problems.
The prognosis is 99% favorable. Relapse of the pathology is a rare phenomenon. After the operation, the patient recovers within 6-10 months.
Possible complications are as follows:
- bleeding may begin;
- there is a small risk of infection;
- the patient's facial nerve may be affected by paresis (especially if the tumor exceeds several centimeters);
- hearing will worsen. If the tumor is larger than 2 cm, there is a high risk that its surgical removal will lead to partial hearing loss.
Radiation (non-operative) therapy
In addition to traditional surgery, there is a safer way to get rid of neuroma. We are talking about stereotactic radiosurgery (cyberknife) - irradiation of the tumor:
- The advantage of this operation is that the tumor is destroyed very precisely. The nerve tissue that surrounds it remains completely unharmed;
- disadvantage - this therapy is effective only if the neuroma is detected in the early stages and does not exceed 30 mm.
Radiation therapy is mandatory if:
- the tumor is located in an “inoperable place”;
- the patient is categorically against surgical intervention;
- the person has already reached old age and has heart problems.
Radiation therapy has side effects. After the procedure, the patient can:
· to feel sick;
· pain appears in the neck (where the stereotaxic frame was located).
Reviews of doctors providing the service - Back and spine injuries
In 2000, Andrei Arkadyevich performed spinal surgery on me.
Four days in the clinic and I have been living a full life for 20 years without restrictions on movement and I remember with gratitude Dr. A.A. Khodnevich. God bless him. And in 2000 he could walk no more than 10 meters. Read full review Viktor Alexandrovich
20.05.2020
Low bow to Alexander Semenovich Bronstein and Andrei Arkadyevich Khodnevich. I arrived at CELT on July 2, 2021 with extreme pain that I endured for 10 days. Hernia C6-C-7. I was given two blockades in Ivanovo, about 9 complex IVs, I lost 6 kg in a week and was in a panic, I didn’t see a way out and nothing happened to me... Read full review
Elena Nikolaevna L.
20.10.2019