General information about the disease
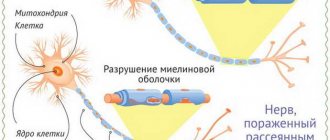
Nerve impulses are transmitted from cell to cell along long fibers called axons. They are covered with a myelin sheath, which facilitates and accelerates the movement of the impulse. The development of multiple sclerosis begins when the body begins to produce antibodies against the myelin sheath and gradually destroy it. As a result, the process of transfer of excitation is disrupted. For some time, the nervous system compensates for the disruptions, but as the disease progresses, the severity of symptoms steadily increases.
Symptoms of multiple sclerosis can appear in both men and women. Males get sick somewhat less frequently, but it is in them that the pathology is more severe and less responsive to treatment.
Make an appointment
Don't be afraid of an SPMS diagnosis
According to experts, not only the patients themselves are afraid of the diagnosis of SPMS, but also, to some extent, doctors. The fact is that for a long time there was no targeted effective therapy for this type of disease, unlike other types of multiple sclerosis, where doctors had the opportunity to slow down the progression or at least improve the patient’s condition.
“SPMS is a severe variant of the development of MS, in which our treatment options are still limited. If in the early stages of relapsing-remitting MS, 15 disease-modifying drugs (DMDs) are approved for use and are already being introduced, then in later and more severe stages of SPMS, the therapeutic choice is limited... It is important to note that many drugs that have proven themselves very well in relapsing-remitting course; at a later stage, SPRS do not work. Neurologists continue to prescribe them, and patients continue to use them in the hope of improving their condition. But this is irrational and clinically unjustified, since no positive effects are observed, only the risks of unwanted side effects accumulate. That is, in reality, these drugs do not help patients with SPMS, but large amounts of money are spent on their purchase,” explains Alexey Boyko.
But there is also hope for a change in the situation of patients with SPMS, which Alexey Boyko speaks about: “Treatment of SPMS in the Russian Federation, as well as throughout the world, is based on an adequate selection of pathogenetic and symptomatic treatment, rehabilitation. The effectiveness of immunomodulatory and immunosuppressive treatment with MS course-modifying drugs is lower in SPMS than in earlier stages of relapsing-remitting MS, but research is ongoing. There are two drugs for the pathogenetic treatment of SPMS with exacerbations; the first drugs have appeared that can help patients with SPMS without exacerbations, the most severe variant of MS. Currently, clinical trials of three more new drugs are planned for SPMS. So there is a prospect of expanding our capabilities.”
This means that it is necessary to change the attitude of both doctors and patients themselves towards SPMS. Stop being afraid and avoid diagnosing it. On the contrary, try to notice the deterioration of the condition as early as possible in order to replace therapy, prescribe rehabilitation and prevent irreversible deterioration. That is, even now, with the correct selection of modern therapy and timely rehabilitation, the condition of patients with SPMS can be significantly improved.
Reasons for appearance
At present, it is not known exactly what exactly triggers the pathological mechanism. Some scientists blame the impact of a specific virus, others put hereditary factors first. Possible causes of multiple sclerosis include:
- brain injuries (concussions, bruises);
- damage to the spinal column;
- chronic mental and/or physical fatigue;
- stress;
- hormonal imbalances (thyroid disorders, diabetes mellitus, as well as changes that occur during pregnancy);
- metabolic disorders, obesity;
- foci of chronic inflammation in the body, etc.
Types and stages
Multiple sclerosis is divided into forms depending on the nature of the disease:
- remitting: exacerbations occur rarely, during the period of remission, brain functions are fully or partially restored;
- primary progressive: the disease begins gradually, the intensity of symptoms slowly increases, and functional recovery does not occur;
- secondary progressive: the patient notes rare exacerbations, between which the symptoms continue to slowly progress;
- progressive-remitting: at first the disease has a similar course to the relapsing-remitting form, but then becomes a stable progressive course.
The severity of symptoms allows us to distinguish the following stages of multiple sclerosis:
- acute: the first two weeks from the sudden onset of symptoms;
- subacute: includes the first two months from the onset of exacerbation;
- Stabilization stage: no exacerbations for 3 months or more.
Difficulty moving
In Russia, a unique medical and social study of the quality of life of Russian patients diagnosed with secondary progressive multiple sclerosis, the most severe autoimmune disease of the nervous system, has been completed.
“SPMS is one of the variants of the course of multiple sclerosis. This type of course occurs after the stage of remitting course and is characterized by a steady progression of the severity of the patients’ condition - first with exacerbations, and then without them. SPMS does not develop immediately, but five to ten years after the initial diagnosis. And if at first the disease progresses slowly - periods of exacerbations are replaced by the absence of symptoms, then with SPMS there are no longer remissions. The situation is complicated by the fact that there is currently no adequate therapy for this type of disease, so in most cases, without treatment, by the age of 40–50, these patients are already deeply disabled,” said co-author of the study, neurologist Alexey Boyko.
Main symptoms
Signs of multiple sclerosis depend on the location of the main part of the pathological foci. As new areas are affected, the symptoms increase and become more varied.
Damage to cranial nerves
Most often, multiple sclerosis affects the optic nerve, which is responsible for image perception. Often these symptoms are the first signs of the disease:
- a sharp decrease in visual acuity in one of the eyes;
- feeling of a veil, haze, black dots or spots in the field of vision that do not go away after blinking;
- narrowing of the view: blind spots appear in the field of vision (damage to the outer or inner half, as well as narrowing like a pipe - circular);
- a sudden change in the perception of one, several or all colors;
- constant feeling of a speck in the eye;
- blurred outlines of objects;
- pain in the eyeball, worsening with eye movement.
The changes persist for 1-2 weeks, after which they disappear completely or partially. Exacerbations occur periodically.
If the oculomotor and abducens nerves are involved in the process, a person may notice the following symptoms:
- strabismus;
- double vision;
- slight drooping of one of the eyelids;
- disorders of coordinated eye movement.
Less commonly, the disease affects other nerves, in particular the trigeminal or facial. In this case, the patient notes symptoms characteristic of their inflammation.
Cerebellar lesion
The cerebellum is the part of the brain responsible for the sense of balance and coordination of movements. If multiple sclerosis affects this area, a person experiences the following symptoms:
- sudden dizziness or imbalance (including loss of ability to skate, scooter, or bicycle);
- unsteadiness when walking: manifested by a short-term sensation of falling or falling to one side;
- change in handwriting for the worse;
- sensation of objects trembling or appearing double;
- Nystagmus: small vibrations of the eyeballs that are noticeable when looking up or to the sides.
Damage to the cerebellum is often the first sign of a developing disease.
Sensory disorders
Damage to the parts of the brain responsible for sensitivity causes the appearance of paresthesia - sensations that occur without any reason. It could be:
- tingling;
- burning;
- itching;
- feeling of skin tightness;
- crawling of goosebumps;
- decreased sensitivity, etc.
Often only one small area is affected: finger, nose, foot, etc. Typically, such problems pass quickly, and the patient does not take them seriously for a long time until the severity of the symptoms becomes much stronger.
The disease can also manifest itself as a violation of temperature, pain or vibration sensitivity, and both a decrease and an increase in sensations are noted.
Pelvic function disorders
Damage to certain areas of the spinal cord leads to specific disorders that force a person to consult a urologist:
- increased or decreased urination;
- sudden and strong urge to urinate;
- feeling of incomplete emptying of the bladder;
- potency disorders in men, anorgasmia in women.
Movement disorders
Movement disorders occur at any stage of the disease. They are represented by a wide range of symptoms, including:
- problems with fine motor skills (buttoning, sewing, etc.);
- muscle weakness of varying severity;
- decreased reflexes (detected during neurological examination);
- muscle cramps, often occurring at night.
Emotional, mental disorders
This area is not often affected by multiple sclerosis, but as the disease progresses, a person may complain of emotional lability, irritability, memory impairment, apathy, etc.
Multiple sclerosis is characterized by a wide range of pathological foci, which is why signs of the disease are rarely limited to any one area. Often, a person notices several different symptoms at once, which occur simultaneously or replace each other. The doctor’s main task in this case is to tie everything together and prescribe tests that will help confirm or refute the diagnosis.
Turn back the clock: new frontiers in the treatment of multiple sclerosis
– Multiple sclerosis is a fairly common neurological disease throughout the world. What is the situation in Russia?
– I wouldn’t say that we are somehow different from the rest of the world; we have approximately the same age range of patients. In terms of incidence, we belong to a medium-risk zone, we have from 10 to 50 cases per 100 thousand population, but in different regions the situation is slightly different. Official current statistics, unfortunately, are known only to the Ministry of Health of the Russian Federation, but at a recent meeting of the Federation Council, representatives of the department reported that we already have more than 85 thousand patients in the federal register. Although the medical community assumes that there should be more than 100 thousand patients.
– How is the profile patient audience classified?
– It is customary to distinguish three types of multiple sclerosis: relapsing-remitting, secondary progressive and primary progressive. In 70–85% of patients, the disease debuts with a relapsing course, which subsequently becomes secondary progressive. Approximately 10–15% are patients with a primary progressive course. There are no official statistics on the primary progressive course in Russia yet, because there was no targeted therapy for these patients until 2021. Therefore, as a rule, their share turned out to be underestimated, somewhere between 2–5% of those officially observed. Now, since targeted therapy has appeared, the approach to both register maintenance and diagnosis has changed. We are striving for earlier diagnosis and greater consideration of these patients, because now there are solutions that we can offer them as therapy. Accordingly, we will gradually get closer to identifying 10% of patients with the primary progressive form and will approximately reflect this group statistically. If we take all patients divided by lobe, it is difficult to say unambiguously, but probably about 70% will be relapsing-remitting, 20% secondary-progressive and about 10% primary-progressive patients.
– What are the scenarios for the development of the disease?
– Patients with a remitting course have the most favorable scenario, because their disease progresses with exacerbations and remissions. Accordingly, during an exacerbation, some new symptoms appear. Some or all of them may regress or may leave behind neurological deficits. But during the period of remission, it is considered that the patient’s condition is stable, that is, there is no increase in symptoms or increase in disability. If the frequency of exacerbations is high or they generally persist, then, of course, this patient may at some point acquire signs of disability. In the secondary progressive type, which replaces the remitting phase of the disease, the disease does not progress from the very beginning. This is precisely the patient who initially had an undulating course of the disease, and then began to show signs of a steady increase in neurological deficit and, accordingly, worsening disability. At the same time, he may continue to have exacerbations, but progression does not depend on them. In some patients, exacerbations at this stage of the disease are no longer observed and only an increase in disability is observed. With the primary progressive type, it is believed that immediately, from the very onset, there is a steady increase in neurological deficit. That is, the symptoms do not regress, but only new manifestations of the disease appear.
– What are the current approaches to treating patients with relapsing-remitting multiple sclerosis?
– Therapeutic approaches remain unchanged. We have pathogenetic therapy, and there is symptomatic therapy. Pathogenetic includes hormonal therapy for exacerbations and immunomodulatory therapy aimed at preventing exacerbations, delaying the progression and increase of changes in brain tissue. For patients with relapsing-remitting multiple sclerosis, the range of drugs is the widest. Almost every year a new drug is released that adds treatment options. Tactically, among all patients with a relapsing course, patients with a rapidly progressing scenario and with highly active multiple sclerosis began to be distinguished. These are those patients in whom either each exacerbation leaves a neurological deficit, and thus the patient’s condition worsens with each new exacerbation, or those who, in principle, during the year, despite receiving any therapy, experience two or more exacerbations, that is It is difficult to keep them simply in a state of remission. When monitoring such patients, a more aggressive strategy is used: either early escalation of therapy - they are transferred from the first line to the second, or the doctor immediately has the right to begin treatment with second-line drugs.
– At what point are patients with multiple sclerosis prescribed drug therapy?
– In general, world practice, as well as Russian practice, is as follows: as soon as a patient is diagnosed with multiple sclerosis, doctors focus on early initiation of therapy. In our country, after a diagnosis is established, personalized information about the patient is entered into the federal register of the Ministry of Health of the Russian Federation, and the patient acquires the right to receive drug therapy free of charge. Another thing is that not all patients agree to treatment that lasts for years; some prefer to be monitored before starting to take medications. In any case, we try to select the optimal treatment option for everyone.
– How then is the effectiveness of the prescribed drug determined?
– Three criteria are used here: firstly, clinical observation – exacerbations persist or are absent; secondly, a neurological examination with assessment of the condition according to the international disability scale EDSS - whether or not there is an increase in neurological deficit; and thirdly, dynamic MRI of the brain/spinal cord allows one to assess the activity of the process in the form of the appearance of new foci or contrasting foci.
– Given the emergence of new drugs, do doctors’ expectations of therapy change?
– Of course, we want, in addition to influencing quantitative changes in brain tissue, to also have the opportunity to inhibit brain atrophy, the rate of which in our patients is higher than age-related physiological atrophy. This is one of the new requirements. And the second is the ability to influence neurodegeneration. In other words, it would be ideal if it were possible to reduce persistent neurological deficits and reverse the process. But so far there are no drugs that can meet these expectations.
– Do you work with the drug alemtuzumab (Lemtrada ® ) and how do you evaluate the practice of its use?
– I have extensive experience in using this drug, I am familiar with it from the development stage and have been observing patients on therapy since 2003 as part of clinical trials. I have quite good impressions, although I can immediately say that alemtuzumab is a complex drug, so it is not indicated for all patients in terms of safety profile.
In the most recent clinical trial of the drug, nine years of data are now available, 49% of patients in the CARE-MS II clinical trial experienced improvement and maintained it over that time. The maximum follow-up period for my patients treated with alemtuzumab was 15 years, but that study has now been completed and the drug has already been registered. Despite this, the developer continues to collect data regarding both the effectiveness and safety profile during phase III clinical trials. Alemtuzumab therapy differs from other immunomodulatory drugs in its cyclic dosing regimen. The first treatment course of therapy consists of two treatment cycles with an interval of a year. There are some patients in my cohort who, after receiving these two treatment cycles, no longer required re-introduction of the drug throughout the study follow-up period. And there are patients who, in some cases three years later, in others five or six years later, still had a “surge” in disease activity. They carried out another treatment cycle and thanks to this maintenance cycle they were able to keep the patient in a stable condition. Therefore, it cannot be said that 100% of patients were stable based on the results of the first starting cycle. But according to clinical studies conducted by the developer, approximately 55% of those observed did not really need to re-administer the drug and at the same time maintained a stable condition. That is, they received two treatment cycles and then everything was fine.
– For what group of patients is the drug recommended?
– Now the drug has updated instructions, which clearly define the patient profile. These are patients with ongoing disease activity on the background of first-line immunomodulatory therapy (highly active disease) or patients with rapidly progressive multiple sclerosis, who, as I have already said, have two or more exacerbations leading to an increase in neurological deficit. Such patients, in principle, according to world statistics, constitute 15–20% of all patients with the remitting type of the disease. This is the target patient population for this type of therapy.
– One of the new criteria for the effectiveness of the drug is confirmed reduction in disability (CDI). What current data does the medical community have on this indicator?
– Naturally, we doctors dream of reducing disability. Data from studies of alemtuzumab suggest that such a result is possible. But we must understand that this effect of reducing disability is not achievable in all patients. It is probably possible to obtain this result, and it will be lasting, if the patient’s profile is correctly determined and, most importantly, therapy is started in a timely manner. Turning back the clock is probably possible if therapy is started in the first three to five years from the onset of the disease.
– When and how is a confirmed reduction in disability assessed?
– Assessment is carried out using the Expanded Disability Scale EDSS. The level of disability corresponds to a certain score, which can increase or decrease. The higher the score, the greater the patient's level of disability. After a neurological examination, the doctor can assess the level of EDSS and note whether there is an increase in it, which tells us about the progression of the disease, or a decrease, indicating an improvement in the patient’s condition. Imagine you have some symptoms, and then their severity decreased, or they regressed, they are gone.
– The drug Lemtrada ® (INN alemtuzumab) was included in the list of 14 high-cost nosologies in 2021, how is this decision assessed by the medical community?
- Of course, it’s positive. This makes it possible to provide the drug to as many patients as this therapy is indicated for. Each subject of the Russian Federation determines the need for the drug itself. Previously, the availability of this therapy was limited by the financial capabilities of the subject; now these drugs are centrally purchased by the Ministry of Health.
The material was prepared with the support of the representative office of Sanofi-Aventis Group JSC (France)
MAT-RU-2001393
Diagnostics
A neurologist diagnoses multiple sclerosis. Often the patient comes to him after being examined by a specialist in another field, for example, an ophthalmologist or urologist. The doctor carefully listens to the patient’s complaints, clarifies the time and circumstances of the occurrence of each symptom, and records information about previous and chronic diseases.
A detailed neurological examination can reveal decreased muscle strength, changes in reflexes and sensory disturbances. These data help to suspect the disease. The main examination to confirm the diagnosis is MRI. The procedure allows you to identify characteristic lesions in the brain or spinal cord. The use of special contrast makes it possible to identify even small affected areas.
In parallel, the following may be prescribed:
- spinal puncture with fluid analysis for specific antibodies;
- consultations with narrow specialists, laboratory and instrumental studies to exclude another cause for the appearance of a particular symptom.
Treatment of multiple sclerosis
Treatment requires complex action. The earlier therapy is started, the greater the chance of slowing the progression of the disease and achieving stable remission.
The main purpose of the effect is to change the activity of the immune system and stop the destruction of nerve cell processes. Depending on the form and stage of the disease, the following are used:
- corticosteroids for temporary suppression of immunity (prescribed during exacerbation of the disease);
- immunomodulators for the prevention of exacerbations (used during the attenuation of symptoms);
- plasmapheresis: hardware purification of blood plasma from antibodies;
- interferons to inhibit destruction processes;
- drugs that suppress the immune system (with rapid progression of the pathology).
In parallel, symptomatic therapy is prescribed:
- antispasmodics;
- antidepressants;
- nootropic drugs;
- angioprotectors;
- painkillers, etc.
The selection of drugs depends on the type and severity of symptoms.
Outside of exacerbations, procedures are prescribed to stimulate the functioning of the nervous system and muscles:
- physical therapy and daily exercises for different muscle groups;
- physiotherapy (with the exception of warming procedures);
- psychotherapy;
- massage;
- Spa treatment;
- vitamins (especially vitamin D).
Make an appointment
Possible complications
As multiple sclerosis progresses, neurological damage becomes more severe and pronounced. In severe cases, the patient becomes bedridden, which leads to the development of bedsores and congestive pneumonia. Damage to the brain stem is fatal due to respiratory or circulatory problems. Frequent complications are:
- chronic pain syndrome;
- loss of control over urination and/or bowel movements;
- neuroses and depression, etc.
Prevention
Prevention of multiple sclerosis is, first of all, general measures that are relevant for every person:
- good sleep;
- minimizing stress and fatigue;
- complete and proper nutrition;
- normalization of body weight;
- elimination of bad habits (smoking, drinking alcohol);
- regular walks in the fresh air and amateur sports.
To prevent relapses, patients who have already been diagnosed should refrain from overheating (visiting baths, saunas, hot baths) and insolation (prolonged exposure to the open sun and visiting a solarium).
When the first signs of trouble appear, even if they occur rarely and only for a short time, it is important to undergo examination by a specialist.
Treatment at the Energy of Health clinic
Neurologists at the Energy of Health clinic offer comprehensive treatment for multiple sclerosis, aimed at eliminating symptoms, preventing relapses and stopping the progression of the disease. We use:
- the most effective drug treatment regimens used in leading clinics around the world;
- physiotherapy in accordance with indications and contraindications;
- physical therapy classes in the clinic and the preparation of a gymnastic complex for home warm-ups;
- restorative and therapeutic massage;
- help from a psychotherapist;
- organization of sanatorium-resort treatment.
Where to sign up for treatment for multiple sclerosis in Moscow?
At the multidisciplinary medical center you can always sign up for treatment for multiple sclerosis
. Our medical center is located between the Konkovo and Belyaevo metro stations (South-Western Administrative District of Moscow in the area of the Belyaevo, Konkovo, Teply Stan, Chertanovo, Yasenevo, Sevastopolskaya, New Cheryomushki metro stations " and "Trade Union"). Here you will find highly qualified personnel and the most modern diagnostic equipment. Our clients will be pleasantly surprised by our quite affordable prices.
Advantages of the clinic
Multidisciplinary medical is a full range of services for the treatment and prevention of various diseases. We offer our clients:
- modern diagnostic methods using high-precision equipment and effective techniques;
- selection of treatment in accordance with the individual characteristics of the body;
- a competent combination of medications, physiotherapy, massage and other non-drug techniques;
- minor surgical operations within the walls of the clinic;
- own day hospital with comfortable wards.
The extensive experience of our specialists allows us to achieve success even in the most difficult cases, and reasonable prices make high-quality medical services accessible to everyone.
Multiple sclerosis cannot be completely cured, but it can be successfully controlled. Remember, even minor neurological disorders may indicate the development of a serious disease. Sign up for diagnostics at Health Energy.
Waiting list
If patients, from the moment of diagnosis of multiple sclerosis (90% have relapsing-remitting multiple sclerosis), immediately begin to receive correctly selected therapy with drugs, the group of which is designated DMT, then the likelihood of transition to the SPMS stage is much lower, and the period of this transition will be longer.
The main thing is individual selection of therapy, a personalized approach at all stages and types of multiple sclerosis.
About 60 thousand patients with MS are already receiving drugs from the DMT group at government expense, and treatment options for primary progressive MS (PPMS) and MS in children and adolescents are expanding. Almost all drugs used in the world are available in the Russian Federation.
“Availability of drugs is another issue. Sometimes there are waiting lists, but the patient waits for months and sometimes even years for the right drug. But with such a course as highly active multiple sclerosis (HAMS), it is urgent to begin effective therapy. It is necessary to improve the system of providing drugs to patients with VARS, since with the existing scheme the patient can lose a lot of time, which will lead to a worsening of his condition, and restoring functions is much more difficult than preventing these disorders,” says Alexey Boyko.
Yan Vlasov agrees with him: “Unfortunately, we are now experiencing a depressive period in our country in terms of providing medicines to our citizens. Drugs for patients with SPMS are becoming less and less available.”