Learn more about diseases starting with the letter “P”: Panic attacks; Duchenne-Erb's palsy; Todd's palsy; Parasomnias; Paroxysmal hemicrania; Paroxysmal myoplegia, Paroxysmal positional vertigo; Peripheral autonomic failure; Hepatic encephalopathy; Pineoblastoma; Pineocytoma; Writer's cramp; Platybasia; Plexites; Brachial plexitis; Humeroscapular periarthrosis; Pneumococcal meningitis Pneumocephalus; Subacute sclerosing panencephalitis; Spinal cord injury.
Pineoblastoma is characterized by a malignant neoplasm. The disease begins with damage to the parenchymal cells of the epiphysis. Occlusive hydrocephalus, damage to the cerebral trunk and cerebellum, all this is characteristic of the course of this disease.
The manifestation may affect intracranial pressure, sleep disturbances, cerebellar syndrome, visual and oculomotor disorders. Pineoblastoma can be diagnosed using neuroimaging, studying cerebrospinal fluid, and histological examination of newly formed tissues. Sequential treatment occurs in 3 stages: neurosurgical operation to eliminate the tumor, radiation therapy, polychemotherapy.
General information
Pineoblastoma belongs to the neuroectodermal type of neoplasm - a poorly differentiated embryonic tumor. In its structure, neoplasia differs little from other malignant tumors, which begin with tissue damage of neuroectodermal origin - retinoblastoma and medulloblastoma.
The tumor begins to progress from the cells of the pineal gland, i.e. gland that produces melatonin, which regulates sleep-wake cycles. The disease is quite rare, accounting for 0.1% of all intracranial neoplasms. Applies to children, mainly males.
Table of contents
- What are embryonal, non-rhabdoid brain tumors and pineoblastoma?
- What are the types of tumors?
- How common are these types of tumors in children?
- Why do children get embryonal, non-rhabdoid brain tumors and pineoblastomas?
- What are the symptoms of the disease?
- How is the disease diagnosed?
- How is a treatment plan made?
- How are these types of tumors treated?
- What protocols and registries are used to treat children?
- What are the chances of being cured from these types of tumors?
Causes of pineoblastoma
The occurrence of pineoblastoma is associated with mutation of individual pinaeocytes, which are capable of rapid division. Mutations are sporadic, meaning a hereditary predisposition is possible. The exact reasons for the change in the state of pinaeocytes have not been identified. Presumably, mutations are caused by the following factors:
- Carcinogens. These substances can adversely affect the genetic mechanism of cellular structure. Food fillers - preservatives, artificial additives, flavors, dyes - can cause a carcinogenic effect. Also components of household chemicals, paints and other similar materials. Exposure to carcinogens during pregnancy is greater.
- Ionizing radiation. It affects the chromosomes of living organisms. Increased radiation, the use of radiation therapy in the treatment of certain diseases.
- Pregnancy with complications. Cell dysfunction can be caused by fetal hypoxia, exposure to toxins (drinking alcohol, smoking, taking drugs), and infections inside the womb. After the baby is born, cells remaining in the pineal gland can contribute to the development of a tumor.
Surgical approaches
As stated earlier, various surgical approaches have been proposed for pineal tumor removal.
A great contribution to the development and improvement of approaches to the pineal region was made by the world's leading neurosurgeons - F.Krauze, WEDandy, KGJamieson, C.Lapras, JLPoppen, K.Sano, BM Stein. Some of the previously proposed surgical approaches have now lost their practical significance, while the occipital transtentorial, infratentorial supracerebellar and subchoroidal approaches are successfully used to remove tumors of the pineal region.
Despite the fact that the technique of performing these operations is described in detail, there are no absolute standards in performing the different stages of surgery. Each author, who has experience in removing tumors of the pineal region, modifies the generally accepted surgical approaches to one degree or another.
Pathogenesis
Why malignant cells appear in the pineal gland is unknown. Here it is relevant to consider many different changes in the genetic structure within cells that can transform the properties of pinaeocytes.
The effect manifests itself in the form of uncontrolled reproduction and lack of differentiation of pineoblasts. Pineoblastoma is characterized by the instant spread of pathology in the tissue and active infiltrative growth. A malignant tumor leads to the destruction of the tissues of the pons and medulla oblongata, spreading to the meninges and subarachnoid space.
The pineal gland is located next to the aqueduct of Sylvius, which drains cerebrospinal fluid into the fourth ventricle. A growing pineoblastoma puts pressure on the aqueduct of Sylvius, thereby blocking the flow of liquor. There is an accumulation of cerebrospinal fluid in the third ventricle, the formation of occlusive hydrocephalus, the manifestation of which is characterized by symptoms of intracranial hypertension.
If we talk about the visible concept of pineoblastoma, then the tumor is a dense, elastic neoplasm of a brown hue. A study under the micro effect will show that the tumor contains small monomorphic cells with hyperchromatic nuclei.
Leading clinics in Israel
Assuta
Israel, Tel Aviv
Ikhilov
Israel, Tel Aviv
Hadassah
Israel, Jerusalem
In its structure, neoplasia is similar to other malignant neoplasms that originate in tissues of neuroectodermal origin: medulloblastoma, retinoblastoma. The cancer process originates in the cells of the pineal gland, a gland that produces melatonin (it regulates the cycles of wakefulness and sleep). The pineal gland synthesizes several bioactive substances - hormones that affect human biorhythms and participate in the activity of the endocrine, nervous and digestive systems.
This disease occurs in only 0.1% of cases of the total number of intracranial tumors; according to ICD10, pineoblastoma has code C75.3.
The pineal gland, or pineal gland, has minimal dimensions and is located between the hemispheres of the brain behind the 3rd ventricle. Next to it is the “Sylvian aqueduct” through which cerebrospinal fluid circulates. This complex anatomical zone where pineoblastoma develops is called the pineal region.
Macroscopically, pineoblastoma is a densely elastic formation of a brown hue; microscopically, this tumor is a collection of small monomorphic cells with hyperchromatic nuclei.
Several features of pineoblastoma can be distinguished:
- Aggressive growth. This leads to the appearance of a pronounced clinical picture in just a few months.
- Increased production of melatonin, a hormone that is responsible for normal falling asleep and waking up.
- Blockage of the ventricles of the brain during tumor growth, which leads to hydrocephalus.
- Spread of the tumor to the spinal cord.
- The predominant diagnosis of this neoplasia is in children and adolescents up to approximately 18 years of age.
Symptoms
The very first symptoms at the initial stage of the disease: progressive headache, vomiting, nausea, decreased performance of vision, sometimes elevated body temperature, whims and anxiety in young children, rarely the presence of convulsive syndrome.
Penetration of the tumor into the midbrain may be accompanied by strabismus, bilateral ptosis, and double vision. Damage to the cerebellum adversely affects the ability to walk normally, measured movements, and control of body coordination. Improper melatonin production is characterized by sleep disturbances. There is also a possibility of hemiparesis, poor sensitivity of body parts, and behavioral disturbances.
Complications with pineoblastoma
This disease is characterized by a rapid increase in intracranial pressure due to occlusion of the cerebrospinal fluid channels. The condition is aggravated due to damage to the third ventricle. Due to the unfavorable course of the disease, the tumor spreads to the lateral ventricles, which practically leads to dysfunction of the ventricular system.
A strong increase in ventricular volume puts pressure on the brain. Given the ability of pineoblastoma to manifest itself in metastases, secondary metastatic foci are possible in the areas of the spinal cord and brain. Hemorrhage into tumor tissues with blood breaking into the ventricles can lead to serious and irreversible consequences.
Complications may also be associated with pressure and the growth of pineoblastoma in the tissue of the medulla oblongata, where the vital centers of the cardiovascular and respiratory systems are located. When cardiovascular regulation is affected, it is fatal.
Bibliography:
- Kaatsch P, Grabow D, Spix C: German Childhood Cancer Registry - Anual Report 2021 (1980-2017). Institute of Medical Biostatistics, Epidemiology and Informatics (IMBEI) at the University Medical Center of the Johannes Gutenberg University Mainz 2021 [URI: www.kinderkrebsregister.de] KAA2019
- Fleischhack G, Rutkowski S, Pfister SM, Pietsch T, Tippelt S, Warmuth-Metz M, Bison B, van Velthoven-Wurster V, Messing-Jünger M, Kortmann RD, Timmermann B, Slavc I, Witt O, Gnekow A, Hernáiz Driever P, Kramm C, Benesch M, Frühwald MC, Hasselblatt M, Müller HL, Sörensen N, Kordes U, Calaminus G: ZNS-Tumoren. in: Niemeyer C, Eggert A (Hrsg.): Pädiatrische Hämatologie und Onkologie. Springer-Verlag GmbH Deutschland, 2. vollständig überarbeitete Auflage 2021, 359 [ISBN: 978-3-662-43685-1] FLE2018
- Mynarek M, Pizer B, Dufour C, van Vuurden D, Garami M, Massimino M, Fangusaro J, Davidson T, Gil-da-Costa MJ, Sterba J, Benesch M, Gerber N, Juhnke BO, Kwiecien R, Pietsch T, Kool M, Clifford S, Ellison DW, Giangaspero F, Wesseling P, Gilles F, Gottardo N, Finlay JL, Rutkowski S, von Hoff K: Evaluation of age-dependent treatment strategies for children and young adults with pineoblastoma: analysis of pooled European Society for Pediatric Oncology (SIOP-E) and US Head Start data. Neuro-oncology 2017 Apr 1; 19:576 [PMID: 28011926] MYN2017
- Rutkowski S, Trollmann R, Korinthenberg R, Warmuth-Metz M, Weckesser M, Krauss J, Pietsch T: Leitsymptome und Diagnostik der ZNS-Tumoren im Kindes- und Jugendalter. Gemeinsame Leitlinie der Gesellschaft für Neuropädiatrie und der Gesellschaft für Pädiatrische Onkologie und Hämatologie 2021 [URI: www.awmf.org] RUT2016
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW: The 2021 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta neuropathologica 2021, 131: 803 [PMID: 27157931] LOU2016
- Gerber NU, von Hoff K, Resch A, Ottensmeier H, Kwiecien R, Faldum A, Matuschek C, Hornung D, Bremer M, Benesch M, Pietsch T, Warmuth-Metz M, Kuehl J, Rutkowski S, Kortmann RD: Treatment of children with central nervous system primitive neuroectodermal tumors/pinealoblastomas in the prospective multicentric trial HIT 2000 using hyperfractionated radiation therapy followed by maintenance chemotherapy. International journal of radiation oncology, biology, physics 2014, 89: 863 [PMID: 24969797] GER2014
- Bode U, Zimmermann M, Moser O, Rutkowski S, Warmuth-Metz M, Pietsch T, Kortmann RD, Faldum A, Fleischhack G: Treatment of recurrent primitive neuroectodermal tumors (PNET) in children and adolescents with high-dose chemotherapy (HDC) and stem cell support: results of the HITREZ 97 multicentre trial. Journal of neuro-oncology 2014, 120: 635 [PMID: 25179451] BOD2014
- Friedrich C, von Bueren AO, von Hoff K, Gerber NU, Ottensmeier H, Deinlein F, Benesch M, Kwiecien R, Pietsch T, Warmuth-Metz M, Faldum A, Kuehl J, Kortmann RD, Rutkowski S: Treatment of young children with CNS-primitive neuroectodermal tumors/pineoblastomas in the prospective multicenter trial HIT 2000 using different chemotherapy regimens and radiotherapy. Neuro-oncology 2013, 15: 224 [PMID: 23223339] FRI2013
- Timmermann B, Kortmann RD, Kühl J, Rutkowski S, Meisner C, Pietsch T, Deinlein F, Urban C, Warmuth-Metz M, Bamberg M: Role of radiotherapy in supratentorial primitive neuroectodermal tumor in young children: results of the German HIT- SKK87 and HIT-SKK92 trials. Journal of clinical oncology 2006, 24: 1554 [PMID: 16575007] TIM2006
Embryonic tumors of the central nervous system and pineoblastoma (brief information) (443KB)
Diagnostics
This disease is diagnosed by neurologists and neurosurgeons. A general understanding of the course of pregnancy, the process of childbirth, the postpartum period, and symptoms of the initial stage of the lesion is given by collecting an anamnesis. The neurologist determines the approximate location of the pathology. Further examination involves:
Clinical tests. A complete blood count may show leukocytosis and anemia. Blood biochemistry gives a general picture of the level of ALT, AST, and protein status.
Examination by an ophthalmologist. Ophthalmoscopy is one of the fundamental diagnostic techniques. If this study reveals papilledema, this means increased intracranial pressure.
Study of cerebrospinal fluid. Eliminates infectious damage to the central nervous system. This method reveals significant cytosis, high protein concentration, and the presence of pineoblasts (tumor cells). Determines the condition of red blood cells.
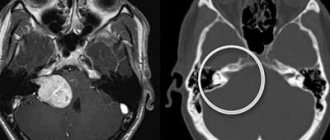
Neuroimaging. Mainly magnetic resonance imaging of the brain, or cerebral computed tomography at an older age. This method is capable of diagnosing neoplasia, its course and localization.
Stereotactic tumor biopsy. This diagnostic method is typical for complex cases when there is a question about neurosurgical treatment. Basically, this is a histological study of the material that is removed intraoperatively.
If symptoms appear in the first year of life, congenital abnormalities of brain development must be excluded. In young children, the first symptoms in the form of vomiting, nausea, and fever can be confused with the manifestation of an intestinal infection.
Treatment of pineoblastoma
Modern treatment includes 3 fundamental stages:
- Surgery. The pineoblastoma needs to be removed as much as possible. The reason for excluding this intervention is the growth of the tumor into the brain stem, threatening to damage the vital centers, as well as the involvement of the choroid plexuses, which can lead to severe bleeding during surgery.
- Radiation therapy. Due to the rapid nature of the spread, total irradiation of the spinal cord and brain is used. The frequency, quantity, and radiation exposure are regulated by the radiologist depending on the individual characteristics of the patient.
- Polychemotherapy. It is used in combination with radiation therapy, as palliative treatment, or after neurosurgery. Determined by a chemotherapist, it contains 2-3 cytostatic drugs. Side effects are accompanied by additional symptomatic treatment.
How is a treatment plan made?
After the final diagnosis, a treatment plan is drawn up. In order to create the most individual treatment program, specifically selected for a particular patient, and to assess the possible risks of relapse of the disease (risk-adapted therapy), the team of treating doctors must take into account certain factors that influence the prognosis of the disease in a particular child (the so-called prognostic factors or risk factors).
Important prognostic factors are the information that was obtained after completing the entire diagnosis: what specific type/type of tumor was found in the child, where exactly the tumor is located, how much it has managed to grow (tumor size) and metastasize. In addition, the biological (molecular biological) characteristics of the tumor tissue (specialists can talk about the molecular profile of the tumor) increasingly determine which treatment is considered the most optimal in a particular case. The age of the child and his general health also matter. The age of the child at the time of diagnosis determines whether the child can be sent for radiation therapy or not. All these factors are included in the treatment plan in order to obtain the most effective treatment result for each patient.
Prognosis and prevention
Pineoblastoma is predicted to have serious consequences. The course of the disease can be fatal due to compression of the brain, hemorrhage in the ventricles, or damage to certain areas of the medulla oblongata. Three-stage therapy has the potential to prolong the patient's life.
The prognosis is determined by the age criterion and the degree of progression of the tumor process. A patient under 5 years of age is characterized by increased malignancy; surviving to 5 years is possible only in 15% of cases. Children over 6 years of age have a more favorable prognosis. Since the causes and organization of pinaeocyte transformation are unknown, it is impossible to prevent the disease.
But it is important to listen to your body and once again consult with a specialist. At the slightest suspicion of the disease, an MRI or CT scan should be done. You can select a medical center using the service. The patient can choose a clinic based on his own needs (geolocation, price, rating, patient’s age, type of tomograph used, type of study). Registration is carried out by calling the phone number posted on the website. As a bonus, the patient receives a discount on examination in the amount of up to 1,000 rubles.
What protocols and registries are used to treat children?
In Germany, almost all children and adolescents with embryonal tumors of the central nervous system or pineoblastoma of the brain, as well as with recurrent disease, are treated according to standardized protocols called therapy optimization studies and treatment registries. German protocols, or therapy optimization studies, are clinical studies and are strictly controlled. Their goal is to treat sick children using the most modern developments. At the same time, these studies provide an opportunity to improve treatment approaches and thereby achieve progress in treatment.
Children who are not being treated according to the current research protocol (for example, if at the time of illness the old protocol was closed and a new one has not yet opened; or if the sick person does not meet the criteria that are mandatory for admission to the current protocol), go through treatment registries. Treatment registries are created and operate in order to advise all patients from modern scientific positions. Also, to ensure high quality of treatment, the research team of a particular protocol usually develops detailed therapeutic recommendations. And when attending physicians contact them, they advise them on choosing the optimal therapy for each individual child.
In Germany, in 2011, the long-term HIT 2000 protocol ended its work, according to which children and adolescents with embryonal, non-rhabdoid tumors of the central nervous system (they were previously called central nervous system-PNET), or patients with pineoblastomas (as well as patients with medulloblastomas and ependymomas) were treated. Numerous clinics throughout Germany and Austria have been using this protocol. Currently, a new protocol is not open for children and adolescents who are newly diagnosed with embryonal, non-rhabdoid brain tumor or pineoblastoma. But these patients are registered in the I-HIT-MED therapeutic registry.
Currently in Germany they operate according to the following registers:
- I-HIT-MED Therapeutic Registry : Children with embryonal tumors of the central nervous system (formerly PNET-CNS) or pineoblastoma, who are currently or in the future not eligible for inclusion in a research protocol, can be treated according to the recommendations of this therapeutic registry (the name of the registry is an abbreviation from English International HIT-MED Registry , that is, the international HIT-MED registry). Patients receive an individual treatment program, that is, it depends on the specific form of the disease. In order for a child to be included in the I-HIT-MED therapeutic register, it does not matter what type of treatment will be carried out. Evaluating the effectiveness of a particular type of treatment is not the purpose of the registry. The therapeutic register is managed by the HIT-MED research protocol team at the University Hospital Hamburg (Hamburg-Eppendorf) (research team leader Prof. Stefan Rutkowski, MD).
- Therapeutic registry HIT-REZ : this registry opened in January 2015. The opportunity to enter it exists for those children who become ill for the first time, but the disease does not respond to treatment; or if the disease has returned to a child who has already been treated (relapse). The treatment regimens in this registry do not test any new therapies or medications. However, the registry is the responsibility of the research office. And he makes therapeutic recommendations that are based on the current results of German anti-relapse protocols (for example, the results of the HIT-REZ 2005 research protocol, which closed in 2021) and international anti-relapse protocols. The central research office is located at the Center for Child and Adolescent Medicine at the University Hospital Essen (headed by Prof. Dr. Gudrun Fleischhak).