The biological clock does not go astray
Nathaniel Kleitman, an American scientist (by the way, an immigrant from Russia) who studied sleep, once spent a whole month in an underground cave in the hope of finding out what was happening with the human biological clock. He assumed that if he did not see sunlight, sunrises and sunsets, they would get confused - and the cycle would either shorten to 21 hours or increase to 28. To his surprise, this did not happen. Our biological clock is always accurate: one sleep-wake cycle lasts 24–25 hours.
In the kingdom of Morpheus. Interesting facts about sleep and dreams
More details
The phenomenon of hypnopaedia
Due to the increasing flow of information, interest in the phenomenon of hypnopaedia – learning during physiological sleep – is growing. Advertisers' suggestion that they wake up in the morning with a good amount of knowledge is tempting. We will not enter into an argument with either opponents or followers of this method; we will only recall a few recommendations:
- The need for mandatory work on mastering the material during the waking period.
- It is strictly forbidden to practice hypnopedia on your own - this can cause mental disorders.
- Compliance with the regime.
For complete assimilation, it is important that the brain has time to go through the required number of cycles. With insufficient sleep, a person risks getting daytime sleepiness rather than fresh knowledge.
Sleep deprivation is deadly
In the 20th century, a genetic disease called “fatal familial insomnia” was discovered: it caused the death of members of more than 30 families around the world. The symptoms are the same. At first, people stopped sleeping - it simply didn’t work, then the pulse quickened and the pressure increased, in the next phase the patients could not speak, stand or walk. It all ended in a couple of months: before death, people fell into a state similar to a coma and died. As a rule, the disease affects middle-aged people and sometimes teenagers.
Article on the topic
How to fall asleep correctly so that you are alert in the morning. Advice from a somnologist
Aging and longevity
A series of articles conceived as part of the “biomolecules” special project for the Science for Life Extension Foundation.
In this series, we will consider the general problems of aging of cells and organisms, scientific approaches to longevity and prolongation of healthy life, the connection between sleep and aging, nutrition and life expectancy (let’s turn to nutrigenomics), we will talk about organisms with negligible aging, we will cover the topics of (epi)genetics of aging and suspended animation
Of course, the phenomenon of aging is so complex that it is too early to talk about radical successes in the fight against it or even a clear understanding of its causes and mechanisms. But we will try to select the most interesting and serious information about the discovered connections, model objects, developed and already available technologies for the correction of age-related disorders.
A brief summary of the special project is highlighted in the video “To grow old or not to grow old? // Everything is like animals.” You will learn more from our articles.
Stay tuned!
A dream is a rehearsal
Scientists are increasingly inclined to believe that the biological significance of sleep is to ensure the survival of the species, be it rat or human. In our dreams, we practice avoiding danger (which seems to be what dreams with threatening content are for), such as swimming across a river or running away from a dangerous animal. But thanks to the special state in sleep, in which our muscles are almost immobilized, all this rehearsal occurs at the level of the brain. Thus, we learn ways to save our lives in a dream so that someday we can use them in real life.
The work of the subconscious: how dreams help solve problems and identify diseases
More details
What to do if you constantly worry about insomnia?
When problems arise in the short term (1-2 days), there is nothing catastrophic about it.
But if you constantly count sheep in the evenings and reach a hundred in your calculations, or jump up before the alarm clock with a swarm of thoughts in your head, then the situation is very serious and requires the intervention of a specialist.
Sleep improves learning abilities
All stages of sleep are associated with learning: the stronger the brain activity during sleep, the better the ability to learn new things. The light sleep stage has been found to be responsible for the development of new skills in musicians, dancers and athletes. It is interesting that this does not happen immediately, but a day or two after the first training and memorization of a play, dance or movement. And during slow-wave sleep, factual information is well remembered: for example, dates from a history textbook.
* Andrea Roca's book "The Brain in Sleep" is provided by Mann, Ivanov and Ferber.
Parasomnias are unusual behaviors that occur in connection with the sleep process. There are parasomnias associated with the phase of slow-wave sleep (FMS, slow-wave sleep), the phase of rapid eye movement sleep (REM, rapid eye movement sleep), etc. REM sleep behavior disorder (RBSD) is a form of parasomnia and is characterized by motor and/or speech activity during sleep corresponding to the content of dreams. The occurrence of sleep behavior disorder is associated with the lack of physiological inhibition of muscle tone in the FBS. RPDS is usually manifested by searching, grasping movements, gesturing, falling out of bed, screaming, punching or kicking, as dreams often include aggressive components [1]. In a number of patients, RPPS is manifested by complex actions that imitate movements during eating, smoking, dancing, sexual behavior and including prolonged speech, singing, etc. [2].
RPPS usually begins over the age of 50 years, and is more common in men, with a frequency of 0.37-0.5% in the population. Within 10–12 years, 40–80% of patients develop a neurodegenerative disease from the group of synucleinopathies: Parkinson’s disease (PD), dementia with Lewy bodies, multiple system atrophy. Based on these data, RPPS is currently considered an early marker of these neurodegenerative diseases [3].
The pathophysiology of RPPS in PD is not fully understood. It is believed that the development of RPPS is caused by dysfunction of brain stem structures involved in the modulation of motor activity during the REM sleep phase ( locus subcoeruleus
, pedunculopontine, giant cell reticular nuclei) and their connections with the limbic system (in particular, the amygdala), frontal cortex, and basal ganglia [1].
Accurate verification of the diagnosis of RPPS is made using video polysomnography (PSG) by identifying tonic and/or phasic electromyographic (EMG) activity associated with behavioral disorders. For clinical diagnosis in the absence of PSG results, the criteria for presumptive RPHD are used [1, 4, 5].
RPPS is considered the most specific early symptom of PD, a key symptom of the pre-motor stage of the disease and can precede the symptoms of parkinsonism by 10-20 years [6]. This connection and the order of manifestation of RPPS and PD can be explained by the earlier involvement of some nuclei of the brainstem in the neurodegenerative process, which manifests itself, in particular, as symptoms of RPPS, while the motor symptoms of PD develop later, with damage to the nigrostriatal system [1]. In patients with diagnosed PD, symptoms of RPHD occur on average in 40–60% of cases [7–9]. At the early stage of the disease in patients who have not received antiparkinsonian therapy, the incidence of RPHD, according to PSG data, is 25% [9].
Despite the relatively high incidence of RPPS in PD, this disorder is not considered as a significant factor in the deterioration of the quality of life of patients [10, 11]. In the absence of severe manifestations of RPPS, leading to self-traumatization and impaired sleep quality, motor activity during sleep is often the cause of psychological and physical discomfort not in patients, but in their loved ones. Thus, according to available observations, 65% of patients with PD are not aware of their behavioral disorders during dreams [12].
Sleepwalking (sleepwalking, somnambulism), unlike RPPS, is a parasomnia associated with FMS. This parasomnia is characterized by repeated episodes of complex sleep-related behavior, including motor activity accompanied by partial (or complete) loss of consciousness, as well as amnesia for the event the next morning. A change in consciousness at the time of the episode is manifested by a lack of response (or its inappropriate nature) when trying to make contact with the patient. In the general population, sleepwalking occurs predominantly in children (18-29% of cases); among adults, its frequency is only 2-4%. Even less frequently, sleepwalking in the general population occurs for the first time in adults (0.6% of cases) [4].
We present a description of a clinical case of a patient in whom regularly recurring manifestations of RPPS, along with rare episodes of sleepwalking, were the main maladaptive disorders. As a result of a neurological examination of a patient who sought medical help for manifestations of parasomnias, a diagnosis was made: PD at an early stage of the disease and essential tremor.
Patient S.,
66 years old, complained of attacks of high-intensity motor activity that occur during sleep and are associated with the content of dreams (gesticulation, jumping out of bed, attacking someone sleeping next to them, causing damage); trembling of the hands, increasing with emotional stress; feeling of stiffness in the neck and back.
From the medical history, according to the patient, “night shudders” have bothered him since childhood. The first case of aggressive behavior in a dream took place in 2001, when during sleep he hit his wife, for what reason he does not remember. After awakening, the patient could only remember that the dream was frightening. Subsequently, episodes of aggressive behavior were repeated almost every time. The most striking of these cases was associated with an attempt to strangle his wife, who was sleeping nearby (the patient dreamed that he was saving his wife from a snake that had wrapped itself around her neck).
The first episode of sleepwalking was observed 11 years ago during a summer vacation at sea, when, having woken up at night, he felt a strong desire to leave the room, opened the door, went out, began to put on the shoes that were standing outside the door, and came to his senses, wondering how such an event had happened. could have happened to him. For 10 years he has had moderate constipation with the need to take laxatives 2-3 times a month. About 8 years ago I noticed a weakening of my sense of smell (previously I could recognize shades of odors well). Around the same time, he began to notice slight trembling of his hands, mainly during postural exertion, performing everyday activities (writing, eating liquid food, holding a glass). About 5 years ago I noticed an increased urge to urinate during the day.
Since 2009, the patient has noted an increase in startles and associated night awakenings. He cannot say what triggers the attacks.
About 9 months ago, the wife began to be concerned about the patient’s increased motor activity during sleep, which corresponded to the frightening plot of the dreams. The wife also noticed a deterioration in posture in the form of a slight stoop (previously the patient had correct posture). The patient began to experience a feeling of stiffness in the neck and back. The nature of hand tremors changed in the form of periodically occurring tremors of the thumb (usually in the right hand); sometimes hand tremors occurred when walking with the right hand hanging freely.
He was consulted by a psychotherapist, who prescribed the patient venlafaxine 150 mg/day (taken for about 3 months), chlorprothixene 5 mg/day. During therapy, a slight positive clinical effect was observed in the form of a decrease in the frequency of nocturnal motor attacks, but hand tremors increased.
About a month ago, a second episode of sleepwalking occurred, which frightened the patient and his wife: the patient got up at night to urinate, tried to leave the room, did not answer his wife’s question, who asked where he was going, then sat down on a chair, sat for a while and returned back to bed . The next morning I did not remember the episode of getting up at night.
Due to persistent attacks of motor activity at night and increased hand tremors, the patient consulted a neurologist at the Clinic of Nervous Diseases named after. AND I. Kozhevnikova. Discontinuation of chlorprothixene was recommended, as well as further neurological, somnological and neuropsychological examination.
From the life history.
Early motor and mental development without features. Academic performance at school was good. As a child, he was involved in skiing. Received a degree in economics. He served in the army twice (under contract) with a total of 20 years of experience. Currently working as a manager. Denies bad habits. Married. Lives with family. Has two healthy children.
Past illnesses
: hepatitis, A at the age of 17 years. Prostate adenoma since 2001, manifested by mild difficulties in initiating urination, weak stream when urinating. In 2011, endoprosthetics of the left hip joint was performed.
Family history:
The life expectancy of grandparents is about 85 years. His mother died at the age of 89 from breast cancer. Father is alive, 93 years old. The patient's mother had hand tremors since she was 70 years old, and the mother's sister had head tremors since she was 50-55 years old. The father has been experiencing hand tremors for the last 10-15 years without significant slowness of movements.
Somatic status.
Height 176 cm, body weight 88 kg, body mass index 28.4 kg/m2. Neck circumference 37 cm. Waist circumference 104 cm. Skin of normal color. Breathing is vesicular, no wheezing. Heart sounds of normal sonority, rhythmic, blood pressure 110/70 mm Hg, heart rate 72 beats/min. Tongue is wet. The abdomen is soft, painless, the liver is identified along the edge of the costal arch.
Neurological status
. Conscious, contactable. Oriented in place and time. A study of cranial nerve function revealed no abnormalities. Revitalization of the proboscis reflex. There are no paresis. The carporadial reflex and reflexes from the biceps, triceps, knees are symmetrical, of medium agility; Achilles reflexes are somewhat reduced and symmetrical. There are no pathological reflexes. Sensitivity is not impaired. Coordinator tests are performed satisfactorily.
Small-amplitude postural-kinetic tremor in the hands, symmetrical. Intermittent resting tremor in the right thumb. Rest tremor in the right hand is provoked by emotional excitement and dynamic load on the left hand. Mild muscle stiffness in the left arm and cogwheel phenomenon are intermittently detected. Minimal hypokinesia in the left hand and left foot when performing dynamic tests (sequential connection and separation of the thumb and index finger, clenching-unclenching the hand into a fist, pronation-supination of the hands, tapping the heel of the foot on the floor). Tendency towards a flexed posture (slight stoop). The gait is not changed. Hypocheirokinesis on the left, intermittent small-amplitude tremor of the right hand in a freely hanging arm when walking.
Assessment of emotional and affective disorders
: according to the Beck Depression Inventory - 8 points (no depression), according to the Spielberger Anxiety Inventory - 35 points (moderate anxiety).
Somnological status.
In the evening he goes to bed at 23:00, gets up at 7:00 on weekdays and weekends. Falls asleep quickly, on average about 5 minutes. Night awakenings occur 1-2 times a night (gets up to go to the toilet). After them he falls asleep quickly. Almost every night (5-7 nights a week), 1.5-2 hours after falling asleep, increased motor activity is observed: from individual winces with gesticulation to complex movements with striking. Notes frequent dreams of a threatening nature. Satisfied with the quality of night's sleep. There is no daytime sleepiness.
Results of additional examination methods
General blood test, biochemical blood test, general urine test
: no deviations from normal values.
Neuropsychological examination (psychologist's report): the identified symptoms can be considered within the framework of mild cognitive disorders. However, the nature of the identified memory impairments does not allow us to exclude signs of primary (hippocampal) mnestic disorders, which may indicate manifestations of the very initial stage of the concomitant neurodegenerative process, including those of an Alzheimer's nature. To finally clarify the nature of the disorders, dynamic observation of the patient and repeated neuropsychological examination are required.
Computed tomography of the brain
: no organic changes were detected in the brain.
Epworth Daytime Sleepiness Scale
— 0 points (norm less than 10 points); obstructive sleep apnea syndrome (OSA) screening questionnaire - 1 point (norm less than 4 points); sleep quality questionnaire - 16 points (norm 22 points or more), sleep disturbance; REM sleep behavior disorder questionnaire (RBD1Q) - 1 point (norm 0 points); REM sleep behavior disorder questionnaire - 11 points (norm up to 5 points), probable RPSD.
To verify the diagnosis of the patient in a hospital ward, an overnight PSG study was performed with registration of the following indicators: 6 electroencephalogram (EEG) channels in monopolar leads - Fp1A1, Fp2A2, C3A1, C4A2, O1A1, O2A2, 2 electrooculogram channels, 1 chin EMG channel, 2 channels of EMG of the anterior tibial muscles, 1 channel of electrocardiography, registration of breathing parameters during sleep with recording of oronasal air flow, respiratory movements of the chest wall, breathing noise, blood oxygen saturation level (saturation) and body position in bed (without adaptation night). Transcription was performed according to the recommendations of the American Academy of Sleep Medicine 2007, as modified in 2012 [13].
The patient arrived at the hospital at 21:00. At 22:45 the lights in the ward were turned off. The study ended at 7:30. The results of the study are presented in Fig. 1.
Rice. 1. Hypnogram of patient C. W - wakefulness; REM—FBS; N1, 2, 3 - corresponding stages of FMS; DC - limb movements (determined by changes in EMG of the tibialis anterior muscles on both sides). The horizontal axis represents the time of day.
The time to fall asleep was 35.5 minutes, the total sleep time was 6.2 hours, the number of awakenings from sleep was 85, the time of wakefulness during sleep was 119 minutes. Sleep efficiency index - 65.3%. The latent period of stage 1 sleep lasted 35.5 minutes, stage 2 - 36.0 minutes, FBS - 72.5 minutes. The duration of the 1st stage of sleep was 4.0 min (0.8%), the 2nd stage - 274.5 min (55.5%), the 3rd stage - 0 min, FBS - 96.5 min (19 ,5%). The periodic limb movement index is 19.5 episodes per hour.
Against the background of episodes of snoring in the patient during sleep, single episodes of breathing disorders during sleep were recorded (respiratory disorder index 1.6 episodes per hour with a norm of up to 5 episodes per hour) and associated episodes of desaturation (desaturation index 1.6 episodes per hour) .
Conclusion based on the PSG results:
The duration of night sleep is reduced. The structure of sleep is changed due to an increase in the time of falling asleep, the number of awakenings, and the time of wakefulness within sleep. There is no deep (stage 3) slow sleep. Against the background of snoring episodes, a clinically significant number of episodes of sleep-disordered breathing and associated desaturations were not identified. In the FBS, against the background of the absence of muscle atonia, various forms of motor activity are recorded from individual winces with gesticulation to complex movements with attempts to strike (Fig. 2).
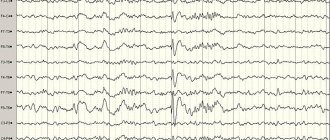
Fig 2. Polysomnogram of patient S. during one of the episodes of excessive transient muscle activity.
Registered on the EMG channels of the right and left peroneal muscles (indicated by an arrow). The epoch of analysis corresponds to the FBS: on the 2 upper channels of the electrooculogram the presence of rapid eye movements is noted (indicated by two arrows), EEG activity predominates in the theta and alpha ranges (the next 6 EEG channels). According to EMG data of the mental muscles (next channel), muscle activity has a relatively high amplitude, characteristic of other stages of sleep, but not of FBS. The first episode of conduct disorder was recorded at 05:10, when the patient suddenly sat up in bed, gestured with his hands and talked. During the attack, movement-related artifacts were noted on the EEG, after which sleep continued in the FBS. The second episode of RPPS was recorded 3 minutes after the previous one. The patient kicked the bed with his right foot and gestured with his right hand. During the attack, movement-related artifacts were also recorded on the EEG, after which sleep continued in the FBS.
The most striking episode of RPPS was recorded at 05:15. The patient rose up in bed, began to make first chaotic, then shock-like movements with his upper limbs, after which he woke up.
Effect of specific treatment
Due to the fact that the patient had clinical and PSG signs of parasomnia in the form of RPPS, he was prescribed clonazepam at a dose of 1 mg at night to eliminate the attacks. While taking the drug, the patient and his wife noted that the frequency of attacks decreased significantly (by about 70%), and the episodes themselves became less intense and disturbing to others. Instead of a developed motor act, an attack of parasomnia persists in the form of twitching of individual muscle groups.
Discussion
Based on the characteristic clinical picture, confirmed by PSG results, the patient was diagnosed with RPHD. The episodes of sleep walking that occurred twice met the clinical criteria for sleepwalking - parasomnia from the group of awakening disorders. This is confirmed by the following manifestations: the presence of repeated episodes of incomplete awakening from sleep; lack of response when trying to make contact with the patient; the patient’s lack of awareness of what is happening during the episode; morning-after episode amnesia; the inability to explain the disorder by the presence of another sleep disorder, mental illness, or taking medications or other medications [4].
The patient also has other diseases. Hereditary history of essential tremor on the part of the patient’s mother and father, and symmetrical postural-kinetic tremor in the hands became the basis for the diagnosis of “essential tremor.” At the same time, the presence of minimal hypokinesia when performing dynamic tests, resting tremor in the right hand, minimal rigidity in the patient’s left hand made it possible to diagnose parkinsonism syndrome. The combination of parkinsonism with signs supporting the diagnosis of PD [14], rest tremor, asymmetric onset of parkinsonism, as well as early non-motor symptoms characteristic of PD (RPD, constipation, hyposmia, overactive bladder), along with the absence of signs atypical for PD, allow us to draw the conclusion about the presence of PD (stage 1.0 on the Hoehn-Yahr severity scale - predominantly unilateral symptoms). As a result, a complete diagnosis of the patient can be formulated: stage 1.0 B.P. Essential tremor. REM sleep behavior disorder. Sleepwalking.
The absence of regression of hypokinesia and resting tremor upon withdrawal of the antipsychotic also indicates that the patient has primary parkinsonism. In addition to the prescribed treatment for RPPS to correct minimal symptoms of parkinsonism, also taking into account the possible neuroprotective effect of the drug [15], he was recommended to take the MAO-B inhibitor rasagiline at a dose of 1 mg/day, therapeutic exercises and increased physical activity.
Thus, a neurological examination of a patient whose main complaints were sleep disorders made it possible not only to clarify their nature and select symptomatic therapy, but also to identify extrapyramidal motor disorders that meet the diagnostic criteria for PD and essential tremor. The presented case is distinguished by a number of syndromic, phenomenological and nosological combinations. Thus, the onset of motor symptoms of PD was preceded by manifestations of essential tremor. The issues of the combination of PD and essential tremor are currently the focus of attention of researchers [16]. The results of the study by R. Feketa et al. [17] showed that 12% of patients with essential tremor developed symptoms of BP during 5 years of follow-up. The association of essential tremor with the trembling variant of PD suggests a commonality of pathophysiological processes of the diseases. It was found that the risk of essential tremor is higher in relatives of patients with the trembling and mixed form compared to the akinetic-rigid form of the disease [18]. The general genetic pathophysiological mechanisms of the development of PD and essential tremor are being clarified [19]. It is worth mentioning that RPPS can sometimes precede essential tremor, but comparative studies of non-motor disorders associated with PD and essential tremor [20] indicate a rarer association of essential tremor with RPPS, as well as other symptoms of the pre-motor stage of PD (hyposmia, hyperactive urinary bubble, memory impairment).
Sleep disorders, which caused the patient to seek medical help, are represented by a combination of two forms of parasomnias. In addition, the patient was diagnosed with subclinical insomnia disorders in the form of changes in sleep structure according to PSG data. Insomnia in the form of a reduction in the duration and quality of night sleep due to an increase in the time of falling asleep, an increase in the number of awakenings, and the time of wakefulness during sleep is the most common type of sleep disorder in patients with PD and occurs in 60–98% of patients [21–23]. Insomnia in PD may be based on primary factors caused by neurodegeneration of brain structures involved in sleep regulation, circadian disorders, as well as secondary factors—motor and non-motor symptoms of PD [22–23]. In the absence of clinically significant secondary factors (depression, nocturnal hypokinesia, sensory, nocturic disorders), in the case described above, we can assume a greater significance of the primary factors of sleep disorders. The patient's PSG results are consistent with recent work by S. Joy. et al. [24], where in patients with early stage PD who were not receiving antiparkinsonian drugs, changes in the FMS were identified (frequent awakenings, a decrease in the total duration of sleep, especially its deep stages - 3rd and 4th). Similar data on the reduction of FMS were obtained during the study of sleep disorders in PD using an experimental model of early parkinsonism [25].
Along with the high prevalence of insomnia, which is a relatively common occurrence in PD, sleepwalking is a very rare phenomenon in this disease. Sleepwalking in patients with PD, mainly in combination with other types of parasomnias, is discussed in a few publications. Thus, as a result of a clinical examination of 417 patients with PD using a questionnaire survey carried out by N. Di Fabio et al. [26], sleepwalking was detected in 9% of patients, of which in 5% it occurred for the first time. In 8 out of 10 patients with this parasomnia, PSG also revealed signs of RPPS. In a study by A. Ylikoski et al. [27], which included patients with PD ( n
=661), who completed the survey, sleepwalking (in all cases in association with RPHD) was found in 1.8%. In summary, sleepwalking is a rare phenomenon in PD, but it occurs more frequently in patients with PD than in the general population. Therefore, the combination of two forms of parasomnia (sleepwalking and RPPS) in the presented patient is a rare but not impossible phenomenon, apparently reflecting the complex nature of the neurodegenerative process in PD, which affects the mechanisms of generating both slow-wave and fast-wave sleep.
There is evidence of a connection between RPPS and a more severe course of PD, the rapid progression of moderate cognitive impairment, the development of dementia, and the addition of visual hallucinations [28–29]. An association of this parasomnia with a greater degree of deterioration in daily activity and a decrease in quality of life assessment, as well as accelerated progression of hypersomnia, depression, and nocturia has been identified [8].
According to N. Di Fabio et al. [26], patients with sleepwalking differed from patients without parasomnias in a higher incidence of depression, anxiety, severity of PD motor symptoms, and worse performance in daily activities. However, no differences in these characteristics were found between patients with sleepwalking and patients with isolated (without sleepwalking) RPPS.
The onset of RPPS at the pre-motor stage of PD development in the patient in the presented clinical case, a significant degree of clinical severity of the phenomenon can be considered as a marker of the early spread of the neurodegenerative process to the brain stem, which is the basis for a possible unfavorable further course of the disease with the development of other non-dopaminergic (or not exclusively dopaminergic) non-motor symptoms of the disease [8]. Thus, the diagnosis of PD and the objectification of RPPS seems significant in the context of predicting the patterns of the further course of PD, the need to monitor the patient (with monitoring of cognitive and other neuropsychiatric disorders) in order to timely prevent and treat concomitant symptoms of the disease.
This patient's medical history demonstrates how the lack of proper assessment of existing sleep disturbances and extrapyramidal disorders contributed to the prescription of inappropriate, potentially dangerous treatment tactics. The administration of venflaxin and chlorprothixene contributed to a reversible increase in tremor, which can be explained by both the undesirable effect of an antidepressant - a serotonin and norepinephrine reuptake inhibitor, and an antipsychotic. According to the literature, the prescription of antidepressants may also be associated with an increase in the manifestations of RPHD. In addition, prescribing an antipsychotic drug to a patient with pre-existing parkinsonism syndrome may be considered a medical error. In light of new data that taking antipsychotics can not only cause drug-induced parkinsonism, but also contribute to a 3.2-fold increase in the risk of developing PD [30], the prescription of drugs of this group to an older patient should be preceded by a thorough neurological examination to exclude extrapyramidal insufficiency. The risk group for iatrogenic parkinsonism is partly formed by patients with a subclinical stage or initial unrecognized clinical manifestations of PD [31]. An alternative to clonazepam prescribed to the patient for the purpose of correcting RPPS is melatonin 2-6 mg at night [1, 5, 32], in the case of a combination of RPPS with severe cognitive impairment, acetylcholinesterase inhibitors may be recommended [33].
Thus, manifestations of parasomnias (RPS and sleepwalking), on the one hand, contributed to the early diagnosis of PD before the development of maladaptive motor symptoms of the disease, since they attracted the attention of doctors with their unusualness, on the other hand, the presence of these concomitant conditions was the basis for clarifying the treatment tactics for PD and essential tremor with the exception of drugs that provoke the development of movement disorders.
The authors declare no conflict of interest.
Psychological reasons
If there are no pathologies, but insomnia is present, the reasons may be psychological. For example, severe anxiety, nervous tension, and stress can deprive sleep for a long time or make it intermittent. Neuroses, anxiety, and depression also prevent you from getting enough sleep.
Sleep problems appear in people who have spent a long time solving an important problem. Here the mechanism of inertia kicks in, and the brain cannot relax for a long time. Sometimes sleep problems are the result of a genetic predisposition.