Traumatic brain injury is damage to the bones of the skull and/or soft tissues (meninges, brain tissue, nerves, blood vessels). The classification of TBI is based on its biomechanics, type, type, nature, shape, severity of injury, clinical phase, treatment period, and outcome of the injury.
Based on the nature of the injury, a distinction is made between closed and open, penetrating and non-penetrating TBI, as well as concussion or contusion of the brain.
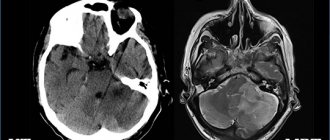
The clinical picture of traumatic brain injury depends on its nature and severity. The main symptoms are headache, dizziness, nausea and vomiting, loss of consciousness, memory impairment. Brain contusion and intracerebral hematoma are accompanied by focal symptoms. Diagnosis of traumatic brain injury includes medical history, neurological examination, skull x-ray, CT or MRI of the brain.
Based on biomechanics, the following types of TBI are distinguished:
- shock-anti-shock (the shock wave propagates from the site of the received blow and passes through the brain to the opposite side with rapid pressure changes);
- acceleration-deceleration (movement and rotation of the cerebral hemispheres in relation to a more fixed brain stem);
- combined (simultaneous impact of both mechanisms).
By type of damage:
- focal (characterized by local macrostructural damage to the brain matter, with the exception of areas of destruction, small and large focal hemorrhages in the area of impact, counter-impact and shock wave);
- diffuse (tension and spread of primary and secondary axonal ruptures in the centrum semiovale, corpus callosum, subcortical formations, brain stem);
- combined (combination of focal and diffuse brain damage).
According to the genesis of the lesion:
- primary lesions: focal contusions and crushes of the brain, diffuse axonal damage, primary intracranial hematomas, brainstem ruptures, multiple intracerebral hemorrhages;
- secondary lesions:
- due to secondary intracranial factors (delayed hematomas, disturbances in cerebrospinal fluid and hemocirculation due to intraventricular or subarachnoid hemorrhage, cerebral edema, hyperemia, etc.);
- due to secondary extracranial factors (arterial hypertension, hypercapnia, hypoxemia, anemia, etc.)
Based on their type, TBIs are classified into:
- closed - damage that does not violate the integrity of the scalp; fractures of the bones of the calvarium without damage to the adjacent soft tissues or a fracture of the base of the skull with developed liquorrhea and bleeding (from the ear or nose);
- open non-penetrating TBI - without damage to the dura mater
- open penetrating head injury - with damage to the dura mater.
In addition, isolated (absence of any extracranial damage), combined (extracranial damage as a result of mechanical energy) and combined (simultaneous exposure to various energies: mechanical and thermal/radiation/chemical) traumatic brain injury are distinguished.
Based on severity, TBI is divided into 3 degrees: mild, moderate and severe. A mild traumatic brain injury corresponds to a mild concussion and contusion of the brain, a moderate one corresponds to a moderate brain contusion, a severe one corresponds to a severe brain contusion, diffuse axonal damage and acute compression of the brain.
According to the mechanism of occurrence of TBI, there are primary (the impact of traumatic mechanical energy on the brain is not preceded by any cerebral or extracerebral catastrophe) and secondary (the impact of traumatic mechanical energy on the brain is preceded by a cerebral or extracerebral catastrophe). TBI in the same patient can occur for the first time or repeatedly (twice, three times).
The following clinical forms of TBI are distinguished:
- concussion,
- mild brain contusion,
- moderate brain contusion,
- severe brain contusion,
- diffuse axonal damage, compression of the brain.
The course of each of them is divided into 3 basic periods: acute, intermediate and long-term.
The time duration of the periods of traumatic brain injury varies depending on the clinical form of TBI:
– acute – 2-10 weeks,
– intermediate – 2-6 months,
- long-term with clinical recovery - up to 2 years.
Possible symptoms of a concussion
- Brief confusion or loss of consciousness. With a strong blow, the moment of injury disappears from memory.
- Dizziness even at rest, and when turning, bending or other changes in body position, the symptom intensifies.
- Severe headache, nausea and vomiting.
- Double vision, inability to concentrate on one point.
- Increased sensitivity to light and sounds.
- Impaired coordination of movements.
- Reaction inhibition - the victim gives an answer to the question after some time.
- Pale skin, weakness, sweating.
Important! A concussion is not always accompanied by visible head injuries, so the absence of wounds does not exclude brain injury.
Reasons for the development of cerebral edema
There are several reasons that influence the development of cerebral edema after injuries. The main one is bleeding that opens inside the skull, which in some situations can be accompanied by hematomas and brain injuries. Such swelling develops slowly, and its symptoms are often confused with a concussion.
There are many factors that influence the development of cerebral edema. Particular attention can be paid to the toxic factor. Exogenous toxic edema can occur in acute poisoning with the following substances:
- acetone;
- petrol;
- methyl alcohol;
- ethanol;
- organophosphorus compounds;
- phenols;
- trichlorethylene;
- benzene and nitrobenzene;
- cyanides;
- turpentine.
Poisoning by these substances can occur if the cause of a traumatic brain injury is a car accident. If a man-made disaster occurs (chemical production, railway junction), then the possibility of developing toxic cerebral edema cannot be ruled out.
The most common situations that result in cerebral edema:
- traffic accidents;
- sports injuries (extreme sports: alpine skiing, luge and speed skating, mountaineering);
- industrial injuries when a person falls from a great height or the cause is a heavy object falling on the head.
The development of the disease is complicated by the structure and functional characteristics of the brain. It must be taken into account that it is located in a confined space, which does not allow it to increase in size. Even a slight increase, due to excess blood or cerebrospinal fluid, entails surges in intracranial pressure and displacement of brain structures.
Swelling of the brain after injury occurs due to the fact that excess fluid begins to accumulate around or inside it, for which there is no way out of the confined space of the skull. Normally, there is only one exit from this space - the foramen magnum (the place where the spinal cord begins).
First aid for concussion
- If one or more symptoms are present, immediately call an ambulance or take the victim to a doctor.
- Treat a wound on the head if it appears as a result of an impact.
- For an hour or until the doctor arrives, it is important not to fall asleep, but to remain at rest.
- If you lose consciousness, lay the person on his side, bend his knees, and put his hands under his head.
- If symptoms of a concussion do not immediately appear, it is recommended to rest and not begin vigorous activity.
Brain contusion
Mild UGM
accompanied by loss of consciousness for up to tens of minutes. Then there is moderate stupor, drowsiness, and there may be incomplete orientation in time and in the environment. Victims complain of constant cephalalgia (headache), weakness, nausea, and dizziness. There is vomiting that does not provide relief, possibly multiple times. Amnesia is observed: the patient does not remember the events preceding the TBI (retrograde amnesia) and for some time after the injury cannot remember what happens to him (anterograde amnesia). Tachycardia or, conversely, bradycardia often develops, and less commonly, arterial hypertension.
In the neurological status: anisocoria, nystagmus, asymmetry of tendon reflexes, unexpressed meningeal symptom complex, there may be mild hemiparesis. When UHM is accompanied by subarachnoid hemorrhage, the meningeal symptom complex is pronounced. With a mild injury, all of these manifestations regress within a period of 2 to 3 weeks.
UGM of moderate degree
manifests itself in an unconscious state for tens of minutes to 4-5 hours. When consciousness is restored, intense cephalgia, repeated vomiting, con-, antero- and retrograde amnesia are observed. Amnesia, moderate or profound stupor, and disorientation may persist for up to several days. Possible mental disorders. Often there is low-grade fever, bradycardia or tachycardia, arterial hypertension, and rapid breathing. The neurological status reveals focal symptoms, varying depending on the location of the bruise area. As a rule, hemiparesis and hemihypesthesia, speech disorders (motor aphasia), anisocoria and oculomotor disorders are observed of varying severity. Typically, these symptoms gradually disappear 4-6 weeks after TBI.
Severe UGM
characterized by a longer duration of unconsciousness (up to several weeks). Motor agitation often occurs. Severe brain contusion occurs with dysfunction of vital systems: arterial hypotension or hypertension, tachy- or bradyarrhythmia, respiratory rhythm disturbance due to tachypnea. In the initial period after TBI, brainstem symptoms dominate: tonic nystagmus, bilateral ptosis and mydriasis, decerebrate rigidity, dysphagia, bilateral foot pathological reflexes, symmetrical hypo- or hyperreflexia. Against this background, signs of damage to the hemispheres are revealed: hemiparesis, hemihypesthesia, oral automatism, etc. Hyperthermia up to 41°C and convulsive paroxysms are possible. Neurological symptoms have a long course and do not fully regress. Mental and/or neurological changes of varying severity remain as persistent residual consequences of TBI.
Recommendations for the treatment of concussions
If hospitalization is not required, with the permission of a doctor, a mild concussion can be treated at home:
- Bed rest and rest are required, no work. Long sleep is very important.
- You cannot read, watch TV, play computer games or use gadgets.
- Under no circumstances should you play sports.
- You are allowed to listen to music, but not through headphones.
- You can use herbal sedative drops or herbal infusions.
- In your diet, you should give preference to dairy and plant products, limit salt intake - to prevent increased pressure, including intracranial pressure.
If the patient seeks medical help in a timely manner and all recommendations are followed, recovery will occur quickly and without complications.
Publications in the media
Disorders due to TBI are a complex of neurological and mental disorders caused by TBI. Frequency • Neuropsychiatric disorders are detected in 90% 2–10 years after TBI • Patients with consequences of TBI make up 10% of all patients observed in psychoneurological dispensaries, of which 65% are men, 35% are women.
Classification and clinical picture Disorders of the initial period • Amnesia (anterograde and retrograde) • Post-traumatic asthenia. Headache, irritability, impaired concentration, fatigue, depression, apathy, anxiety • Vestibular disorders. Gait instability, dizziness, nausea, vomiting, nystagmus, weakened convergence of the eyeballs • Autonomic disorders. Fluctuations in blood pressure and pulse rate, increased sweating and salivation • Acute traumatic psychoses: all forms of psychotic conditions are observed, most often delirium, Korsakoff psychosis, mood disorders, delirium, hallucinations • Convulsive syndrome is more often observed in the acute period of contusions after open head injuries, base fractures skulls; Partial convulsive seizures are characteristic.
Disorders of the long-term period • Traumatic encephalopathy •• Traumatic asthenia (traumatic cerebrovascular disease, traumatic asthenia). Symptoms : weakness, fatigue, decreased performance, apathy, emotional lability, tearfulness, short violent outbursts of irritation followed by repentance, hyperesthesia, autonomic and vestibular disorders, sleep disorders •• Personality disorders: strengthening of psychopathic character traits that existed before the TBI: unmotivated mood swings , attacks of irritation with aggression and antisocial behavior, litigiousness, substance abuse •• Mood disorders ••• Subdepressive states with dysphoria, fear, anxiety, hypochondria ••• Hypomanic states with euphoria, lack of criticism, disinhibition of drives, drunkenness •• • Cyclothyme-like conditions are more often represented by unipolar disorders, less often - bipolar •• Traumatic epilepsy (traumatic encephalopathy with convulsive syndrome) in the form of various convulsive seizures, ambulatory automatisms, twilight disorders of consciousness • Traumatic psychoses: in the form of affective, delusional and hallucinatory disorders are rarely observed • Traumatic dementia • Organic psychosyndrome in the form of memory impairment (amnesia, confabulation), decreased intelligence, emotional instability.
Treatment • Nootropic drugs, drugs that improve cerebral circulation and regulate metabolic processes in the central nervous system (for example, piracetam, aminalon, pyritinol, nicergoline, pentoxifylline, dimephosphone, cerebrolysin). • With the development of delusions and hallucinations, psychomotor agitation •• Haloperidol 5–15 mg/day orally or intramuscularly •• Trifluoperazine 5–15 mg/day orally or intramuscularly •• Chlorpromazine 25–50 mg intramuscularly •• Levomepromazine 25–50 mg IM. • For mood disorders - see Mood disorders. • For behavioral disorders - periciazine 10-30 mg/day orally. • For anxiety, insomnia •• Oxazepam 10–30 mg/day •• Zopiclone 7.5–15 mg/day •• Bromodihydrochlorophenylbenzodiazepine 1–3 mg/day. • For lethargy, apathy - tinctures of lemongrass, ginseng, eleutherococcus. For severe asthenia, mesocarb 10–40 mg/day. • Treatment of paroxysmal disorders is similar to treatment for epilepsy. The prognosis depends on the form and severity of the TBI. In 20% of cases, the consequences of TBI lead to disability, in 45% to decreased ability to work, only 25% of patients return to their previous work. In case of severe or repeated TBI and concomitant diseases, the course is progressive and remitting. Synonyms • Post-concussion syndrome • Post-concussion syndrome
ICD-10 • F07 Personality and behavioral disorders caused by disease, damage or dysfunction of the brain • T90.5 Consequences of intracranial trauma
Hemorrhagic stroke
Case from practice
Many people think that cerebral hemorrhage is the lot of old people and alcoholics, but this is not at all true.
One day an eleven-year-old boy was brought to us in a deep coma. The diagnosis is hemorrhagic stroke. His story came out a little later. Nothing foreshadowed trouble that day. In the morning the boy had breakfast and went to school. Russian, mathematics, physical education class... In physical education everything went as usual: running, warming up, jumping over a goat, and at the end of the lesson - basketball. No particular rules were observed, and the battle for the ring began. Excitement gripped the boys, and to the cheerful hooting of the girls, the ball ended up on one or the other half of the field. The two-point advantage forced us to fight for the ball all the way.
In the last minutes, one of the players famously threw the ball across the entire field. A rather heavy projectile whizzed through the air. A rubber ball fell on the head of our young athlete. The body was thrown to the side, the boy froze in an unnatural position. The guys surrounded him, the coach tried to bring the boy to his senses, but in vain. An ambulance was immediately called. The doctor decided to urgently take him to the hospital.
The patient was brought in already in a deep coma, the condition was threatening, and swelling began to spread around the site of injury. The brain is perfectly protected from external damage, but this is its problem - the cranium does not give room to the swollen brain. The only free foramen is the magnum magnum. As a result, the swollen brain compresses the structures located in the brain stem. But there are the most ancient vital centers - respiratory and cardiovascular, damage to which leads to death.
The boy had signs of widespread cerebral edema, and therefore he was transferred to controlled ventilation. The parents were horrified by what was happening, they begged to transport the baby to the central clinic, but the risk of increasing the hemorrhage area was too high. Long days of treatment and caring for the little patient passed. Day after day, week after week. The child, like a broken doll, lay and did not move.
We were already desperate, we thought that we had received a deep brain disability. But a little more than 20 days passed, and a weak reaction of the pupils to light appeared, then he began to move his fingers and began to resist mechanical breathing. He was switched to ventilation mode - when the breathing apparatus reacts to the patient’s respiratory movements and only ventilates when necessary. In approximately this condition, we sent him to the regional children's hospital.
A few months later, I met smiling parents at the clinic, and our baby was sitting with them. An absolutely normal child, there were no consequences from the hemorrhage. They are now being seen by a neurologist.
Unfortunately, we cannot boast of such results in all patients who have suffered a cerebral hemorrhage. Very rarely such patients are discharged; more often they die in an intensive care bed. The outcome of a hemorrhagic stroke is, on average, much worse than an ischemic stroke.
Causes of cerebral hemorrhage
1. The most common and completely controllable problem is hypertension
. More than 85% of patients suffer precisely as a result of a sharp jump in pressure in the circulatory system (hypertensive crisis). You must understand that pressure above 140 over 90 is already high blood pressure, and with such pressure you are at risk of rupturing a cerebral vessel.
2. Congenital and acquired cerebral aneurysms
. This is where things get a little more complicated. How can you tell whether there is a bomb in your head or not? Does every person really need to go and have cerebral vessels contrasted? Perhaps this is unrealistic, since not all clinics have a magnetic resonance imaging scanner, and the price is steep (both for the tomograph and for the examination itself). Although otherwise, the procedure is generally painless and low-toxic.
If the identified aneurysm makes itself felt by headaches, if it begins to compress the passing nerve pathways and manifests itself with any symptoms, then, of course, it needs to be removed. There is no other option, the pill definitely won’t help.
3. Atherosclerosis
as a cause of hemorrhage. Plaques change the vascular wall, the movement of blood becomes not free, linear, but laminar; in the places of these turbulences, against the background of high blood pressure, saccular formations (microaneurysms) are formed, ready to explode at any moment due to a sharp jump in blood pressure (hypertensive crisis). You see - again we return to the treatment of arterial hypertension.
4. Blood diseases
. This refers to those problems that lead to impaired blood clotting ability. Most likely, throughout our lives we experience small, invisible hemorrhages. But our health is guarded by a coagulation system with many different factors, and they prevent the hematoma from spreading further. Look at boxers - they regularly get hit in the head and often have hemorrhages, which, however, have little effect on their vital activity. However, if a person has leukemia or other blood diseases that lead to depletion of coagulation factors or suppress the formation of certain coagulation factors, then any blow to the head can be fatal.
5. Intoxication
. Actually, toxins play a role here, leading to high blood pressure and disruption of the blood coagulation system (for example, snake venoms).
6. Inflammatory diseases of the vascular wall
(autoimmune diseases, collagenosis, infections). Cerebral vessels are extremely impermeable to unnecessary substances, but any pathological change can lead to increased permeability and fragility of the wall.
Can it be prevented?
The disaster begins suddenly, with a sharp headache, flashes before the eyes, nausea and vomiting, dizziness, and weakness in one half of the body. There may be convulsions, disturbances in heartbeat and breathing. In the vast majority of cases, the patient loses consciousness. Unfortunately, in more than half of the cases everything ends in death. So hoping for treatment is not an option, you just need to not push yourself to the extreme. For this:
- Monitor your blood pressure. To control it, you don’t need expensive equipment or standing in line. What’s simpler: measure it in the morning, take a pill if necessary, and move on with your life. I got nervous, took a sedative, measured it, measured it again, and if necessary, take a pill. That’s it, you don’t have to endure hypertensive shocks in your head; with age, the blood vessels are not so elastic, and the next powerful contraction can hammer a nail into the lid of a box with red upholstery.
- Do not avoid a planned, annual examination of your body. Perhaps you are already accustomed to a certain problem, and the doctor with a clear eye will suspect a threatened condition.
- Quit smoking - completely, never, even when drunk, touch a cigarette. What is the connection between cigarettes and hemorrhagic stroke? Believe me, it is much easier to treat a patient with healthy lungs than a patient with COPD.
- About alcohol. My opinion: moderation is everything! Sometimes it’s better to sip a glass of cognac and calm down and get some sleep than to suffer half the night from painful thoughts. But again: I am not calling for alcoholism, especially since there are more effective sedatives.
Trite, simple and boring, but effective.
And further. If you begin to suffer from regular headaches localized on the same side, or a feeling of numbness in a limb, you may have a growing aneurysm or tumor. Run to a neurologist before it’s too late!
Vladimir Shpinev
Photo istockphoto.com
Why do violations occur?
COVID-19, like any other virus, affects the functioning of many body systems and affects not only the respiratory tract and lungs, but also the central nervous system. This is called neurotropism - the ability of an infection to infect cells of this system. Moreover, researchers believe that the virus multiplies inside the nerve cells of the brain.
Autopsy results show that coronavirus leads to inflammation of brain tissue. And neuroimaging techniques that show the structure and dysfunction of the brain reveal microstrokes and leukoencephalopathy, a condition that leads to demyelination when the covering of nerve cell processes is destroyed.
These organic damages lead to the person developing mental and neurological disorders, which are complications.
Rules of rehabilitation, physiotherapy, folk remedies
Recovering from a concussion is very difficult. In the first weeks, the patient will need to be observed inside the hospital. There he will be provided with all the conditions for rehabilitation and reducing the risk of complications. After this, the patient will go home, where he will need to follow certain rules and attend physiotherapeutic procedures. Additionally, you can use folk remedies.
Rules
Recovery can only be achieved if the patient adheres to certain rules. Also, in the first days he will be prescribed bed rest. What to consider during the rehabilitation period:
- Avoid physical activity and sudden movements;
- Provide contact with fresh air (open windows or walk);
- Do not overstrain your eyesight, limit the time allocated to the computer, TV, reading;
- Follow a diet, eat more vegetables and fruits, eliminate junk food;
- Take vitamin complexes;
- Stop drinking alcohol and smoking.
If necessary, you should visit your doctor regularly. Many patients require work with a speech therapist or psychologist.
Physiotherapy
Physiotherapeutic procedures are particularly effective during the rehabilitation period. You should visit them strictly according to your doctor's instructions. If a severe brain injury is sustained, then they may be contraindicated, which should also be taken into account.
Popular procedures:
- Electrophoresis;
- UHF therapy;
- Galvanization of the brain;
- Laser therapy;
- DMV therapy
- Air baths.
If you feel unwell after the procedures, you should inform the doctor about this in order to adjust the rehabilitation conditions.
Folk remedies
You can achieve a positive result in recovery at home using folk remedies. They will not be able to be fully treated, but they will have an additional effect, speeding up rehabilitation.
You can use the following recipes:
- Mix motherwort, hawthorn, plantain, elecampane with comfrey in equal quantities, pour boiling water over it and let it brew. Take morning, afternoon and evening.
- Pour boiling water over the rose hips, add honey and lemon, mix thoroughly. Determine the proportions to your taste.
- Grind Ginkgo Biloba leaves and add to food or tea. Can be consumed without additives with water.
- Mix hawthorn and sea buckthorn in equal quantities, bring to a mushy mass, add a small amount of honey, stir. Store in the refrigerator, taking 2 tbsp morning and evening. l. Take a break for 10 days every 2 weeks.
- Mix 200 ml of raisins and pistachios, add 200 ml of figs, chop. Drink 50 ml daily. The course of admission is 7 months.
Before use, you should consult a doctor so as not to harm your health.
How to deal with post-traumatic headaches?
Treatment of acute PTTH involves taking emergency measures to eliminate the cause that caused them (elimination of hematoma, etc.). For concussions, the following medications are prescribed:
- Cerebrolysin (peptide complex to improve metabolism in nerve cells, administered intravenously);
- Mildranate or Actovegin (antioxidants for intravenous administration);
- Cavinton (a drug for improving cerebral blood flow);
- Diacarb (dehydrant to prevent cerebral edema).
If chronic post-traumatic pain develops, treatment is carried out using the same methods as for most primary headaches. One of the most important components of therapy is the psychological rehabilitation of the patient.
They very often have concomitant mental disorders - anxiety and depression. To cope with such conditions, the help of a qualified psychotherapist is required. During the recovery period, hypnotherapy and neuroprotective therapy, as well as acupuncture, are widely used. For pain that spreads from the neck to the back of the head, the doctor may prescribe physiotherapy and therapeutic exercises, as well as exercises in the swimming pool. Drug treatment is carried out in two directions - stopping attacks and preventing them. Analgesics and β-blockers are indicated to relieve pain. In many cases, vascular agents are useful in the treatment of post-traumatic headaches. With their help, microcirculation in the brain pool improves. Thanks to this, regulatory processes in the central nervous system are restored. Memory impairment and other cognitive disorders are indications for the use of nootropics in the treatment of headaches after injury. The fight against reversible mental disorders often requires the prescription of tricyclic antidepressants. They stabilize the psycho-emotional state and normalize sleep. For the treatment of acute and chronic post-traumatic pain, patients are prescribed vitamin and mineral complexes, including folic acid, B vitamins and phosphorus. Intense cephalgia, accompanied by insomnia, is an indication for taking sedatives - Dormiplant or Adaptol. Combination therapy may include manual therapy sessions. Patients suffering from chronic PTTH need to be observed by a neurologist.
The text was checked by expert doctors: Head of the socio-psychological service of the Alkoklinik MC, psychologist Yu.P. Baranova, L.A. Serova, a psychiatrist-narcologist.
CAN'T FIND THE ANSWER?
Consult a specialist
Or call: +7 (495) 798-30-80
Call! We work around the clock!