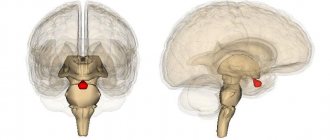
Pituitary adenoma is a tumor of the anterior lobe of this endocrine gland. The disease most often affects people aged 40-45 years. Among all brain tumors, a third of cases are pituitary adenomas. Pituitary microadenoma is a benign neoplasm growing from the glandular cells of the organ, the size of which does not exceed 10 mm.
Due to the small size of the tumor, symptoms of the disease with pituitary adenoma are absent for a long time. Doctors at the Yusupov Hospital identify the tumor using modern research methods. Early diagnosis and adequate treatment of pituitary adenoma allows patients to get rid of the disease.
Pituitary adenoma of the brain - what is it?
What is a pituitary adenoma of the brain? Pituitary adenoma is a benign tumor that is formed from the cells of the anterior lobe of the endocrine gland, which plays a huge role in maintaining the normal hormonal balance of the body. The neoplasm does not have morphological signs of malignancy, but is capable of germination and mechanical compression of brain structures adjacent to the pituitary gland.
Pituitary adenoma disease manifests itself with visual, neurological and endocrine disorders. Symptoms of pituitary adenoma of the brain are associated with the pressure of the growing tumor on the intracranial structures of the head, which are located in the area of the sella turcica.
If the pituitary adenoma is hormonally active, endocrine metabolic syndrome comes to the fore in the clinical picture. In this case, changes in the patient’s condition are often associated not with the excess secretion of pituitary tropic hormone by the pituitary gland itself, but with the activation of the target organ on which it acts. Manifestations of endocrine metabolic syndrome directly depend on the nature of the pituitary adenoma of the head.
A pituitary adenoma of the brain may be accompanied by symptoms of panhypopituitarism. It develops when pituitary tissue is destroyed by a growing tumor. The variety of symptoms of the disease complicates the diagnosis of pituitary adenoma in the early stages of the pathological process.
Types of pituitary adenoma
In the International Classification of Diseases, pituitary adenoma has ICD-10 code D35.2. Based on the size of the tumor, a distinction is made between pituitary microadenomas, the size of which does not exceed 1 cm, and macroadenomas. Depending on the hormone-forming function of the tumor, hormonally active and inactive pituitary adenomas are distinguished. There are several types of hormonally active adenomas:
- Corticotropinoma – produces adrenocorticotropic hormone ACTH;
- Somatotropinoma – produces the somatotropic hormone GH;
- Prolactinoma – synthesizes prolactin;
- Thyrotropinoma – participates in the excretion of thyroid-stimulating hormone;
- Gonadotropinoma - can produce hormones such as follicle-stimulating hormone (FSH) or luteinizing hormone (LTH).
Oncocytoma and chromophobe pituitary adenoma are hormonally inactive neoplasms. Depending on the histological structure of the tissues, the following types of pituitary adenomas are distinguished: pituitary adenocarcinoma, chromophobe, basophilic, acidophilic, acidobasophilic or mixed tumor. Endosellar pituitary adenoma is located inside the sella turcica, endosuprasellar - extends to the top of the sella turcica, endoinfrasellar - goes down from the sella turcica, endolaterosellar - grows through the side wall of the sella turcica. The cystic form of pituitary adenoma is a complication of the neoplasm.
Fragment of the “Good Morning” program dedicated to the treatment of pituitary adenomas
Classification of pituitary adenomas.
There are several types of classifications of hypertension. One of them is based on the hormonal activity of tumors , which has been actively used since the early 70s of the 20th century. According to this classification, adenomas are divided into hormonally inactive (40%) and hormonally active (60%). The latter are characterized by overproduction of various pituitary hormones. Among them are somatotropinomas , which make up 20% - 25% of the total number of pituitary adenomas and cause acromegaly, prolactinomas - 40%, corticotropinomas - 7%, causing Itsenko-Cushing's disease, and thyrotropinomas - 3%. Hormonally active pituitary adenomas, causing hyperproduction of hormones, lead to the development of various, often severe, endocrine metabolic disorders in patients.
According to the nature of growth (the relationship of the tumor to the sella turcica, in which the normal pituitary gland is located, and the surrounding structures), pituitary adenomas are divided into:
- Endosellar (inside the sella turcica).
- Endosuprasellar (extends upward beyond the sella turcica).
- Endoinfrasellar (the tumor extends downwards from the sella turcica).
- Endolaterosellar (the tumor destroys the lateral wall of the sella turcica and grows into the cavernous sinus).
- Very often, the direction of growth of a pituitary adenoma is different - up, to the side, down, etc., and then the tumor is called endo-supra-infra-laterosellar.
Based on size, the tumor is divided into microadenomas (no more than 1 cm in diameter) and macroadenomas (more than 1 cm).
| Brain MRI, T1-weighted image. Endo-supra-laterosellar macroadenoma (somatotropinoma). The tumor grows into the right cavernous sinus and invades the internal carotid artery. Spreading suprasellarly, the tumor compresses the chiasm and the bottom of the third ventricle. |
Clinic of pituitary adenomas.
The clinical picture of pituitary adenomas is polymorphic and is represented by different groups of symptoms. At the stage of microadenomas or small endosellar tumors, tumors with pronounced endocrine symptoms are more often diagnosed (Cushing's disease, acromegaly, amenorrhea-lactorrhea syndrome in women and impotence with gynecomastia in men, thyrotoxicosis).
Pituitary hormones and their function.
| Hormones of the anterior pituitary gland (adenohypophysis). | Normal concentrations of hormones in peripheral blood. | Function |
| Adrenocorticotropic hormone (ACTH) | 10.0 – 60.0 pg/ml | Regulation of the secretion of a number of hormones by the adrenal glands, including cortisol, the overproduction of which leads to the clinical picture of Itsenko-Cushing's disease. |
| Somatotropic hormone (GH, growth hormone) | 0.01 - 11.5 mU/l | The main hormone responsible for the growth of the body. Overproduction of this hormone leads to acromegaly. |
| Thyroid-stimulating hormone (TSH) | 0.25 - 3.5 m Units/l | Responsible for regulating the production of thyroid hormones (T3 and T4). |
| Prolactin (PRL) | 90 - 540 mU/l | Responsible for the formation of milk in the mammary glands. When overproduction occurs in women, the menstrual cycle is disrupted, and in men, impotence and decreased libido occur. |
| Follicle stimulating hormone (FSH) | Stimulates the growth of follicles in the ovaries in women and sperm formation in men. | |
| Luteinizing hormone (LH) | Stimulates ovulation in women and promotes pregnancy. In men, it regulates testosterone production. | |
| Posterior lobe (hormones are not formed here, but accumulate). | ||
| Antidiuretic hormone (ADH) | Controls the feeling of thirst and the amount of urine excreted by the kidneys. With a lack of this hormone, diabetes insipidus occurs. | |
| Oxytocin | Stimulates uterine contractions in women. | |
| Intermediate share. | ||
| Proopimelanocortin and lipotropin | Regulate the formation of pigment in cells and enhance fat metabolism. | |
Itsenko-Cushing's disease (CID). This is a disease associated with hyperproduction of ACTH (adrenocorticotropic hormone) by pituitary adenoma (it is possible that only hyperplasia of the corresponding cells of the adenohypophysis may occur). With NIR, microadenomas are detected in 95% of cases. Tumors not operated on at this stage tend to grow invasively, affecting the bone structures of the skull base. The disease is much more common in women aged 20–40 years. The basis of the clinic is the symptoms associated with hypercortisolism: dysplastic obesity, trophic changes in the skin, arterial hypertension, steroid cardiopathy, systemic osteoporosis, symptomatic diabetes, secondary immunodeficiency, changes in the psycho-emotional sphere. The severity of the disease and prognosis are largely determined by the degree of damage to the cardiovascular system - myocardiopathy of endocrine-metabolic origin is aggravated by a persistent and difficult to correct increase in blood pressure and leads to the development of chronic circulatory failure.
Acromegaly is a disease that is caused by overproduction of somatotropic hormone (GH). In the vast majority of cases, the cause of hyperproduction of GH is pituitary adenomas. The mortality rate of patients with acromegaly is 10 times higher than that in the population, mainly due to cardiovascular complications. There are from 50 to 70 cases of acromegaly per 1 million population; patients are usually of working age (20–40 years). A clear relationship between the incidence of acromegaly and gender has not been identified, although many doctors indicate a greater predisposition of women to this disease. The main manifestation of acromegaly is enlargement of the limbs, changes in the facial skeleton; at the onset of the disease in childhood, when calcification of the epiphyses has not yet occurred, it can manifest as gigantism. Characterized by swelling of soft tissues, greasiness of the skin, seborrhea. Often patients are bothered by a headache, which can become unbearable. The time from the appearance of the first symptoms to the establishment of an accurate diagnosis ranges from 5 to 15 years and significantly depends on the level of culture of the population. Treatment of acromegaly is a complex task, the effective solution of which depends on the timeliness and accuracy of diagnosis, the speed and severity of the disease, and the presence of concomitant diseases. Basically, treatment consists of eliminating the clinical symptoms of the disease associated with increased production of hormones, stable normalization and restoration of the rhythm of secretion of pituitary hormones. Epidemiological studies have shown that when the basal level of growth hormone is reduced to safe values (basal growth hormone level < 5 mU/L (< 2 μg/L), the level of growth hormone after an oral glucose tolerance test is < 2 mU/L (less than 1 µg/l)), the mortality rate in these patients decreases to the mortality level in the general population.
Hyperprolactinemia can be a manifestation of various diseases, including prolactin-secreting pituitary adenomas. The latter are diagnosed at the microadenomas stage in approximately 80% of cases in women; in men this happens much less frequently due to a less vivid clinical picture and not always a responsible attitude towards emerging sexual problems. Clinically, prolactinomas at the “endocrine” stage of the disease in women are manifested by menstrual irregularities, lactorrhea, and infertility. Men complain of decreased libido and potency, gynecomastia.
With macroadenomas with suprasellar growth, the main complaints of patients are decreased vision (decreased visual acuity, narrowing of visual fields) and headache.
Sometimes the course of the disease sharply worsens, which is most often manifested by a sudden deterioration in vision and/or the appearance of oculomotor disorders (double vision, ptosis) in combination with headache. This is due to hemorrhage into the tumor, which is usually clearly visualized on MRI.
| Brain MRI, T1-weighted image. Endosuprasellar adenoma of the pituitary gland with hemorrhage and severe compression of the chiasm and the bottom of the third ventricle. |
Diagnosis of pituitary adenomas.
1. Examination by a neurosurgeon, endocrinologist. 2. X-ray of the skull. 3. Hormonal blood test. 4. Computed tomography of the brain. 5. Magnetic resonance imaging.
Treatment of pituitary adenomas.
Today, there are three main types of treatment for patients with pituitary adenomas - neurosurgical, radiation (proton therapy, gamma therapy, gamma knife), drug treatment (dopamine agonists, somatostatin analogues, somatotropin receptor blockers) and their combination. The decision on the treatment method depends on the type of tumor, its size, location and degree of hormonal activity of the tumor, and is made individually for each patient. Neurosurgical treatment is in most cases considered first-line therapy; if it is ineffective, other treatment methods are followed. However, there is a group of adenomas to which, first of all, conservative treatment (some prolactinomas and somatotropinomas) or radiation therapy is applicable.
| Brain MRI, T1-weighted image. The left image shows endo-supra-laterosellar macroprolactinoma in a 40-year-old man (prolactin level before treatment was 3500 mU/l). In the center - MRI of the same patient 2 months after conservative treatment (bromocriptine). On the right - after 6 months of treatment (prolactin level 2.6 mU/l). |
If the question of surgical treatment arises, then the bulk of endosellar micro- and macroadenomas of the pituitary gland must be removed using a transnasal approach .
| Scheme of transnasal transsphenoidal surgery. |
Postoperative mortality among all adenomas is about 4%, being practically zero among endosellar and endosuprasellar tumors, and increases as the size of the tumor increases, when it invades the ventricular system and the tumor invades the vessels of the circle of Willis. Due to the infiltrative growth of pituitary adenomas, their radical removal is often impossible. In such cases, it is necessary to resort to combined treatment (neurosurgical removal + radiation therapy and/or conservative therapy). The use of combination treatment allows achieving good results in the treatment of tumors of this location.
| MRI of the brain before surgery: giant endo-supra-infrasellar pituitary adenoma with compression of the chiasm and formations of the third ventricle. | MRI of the same patient 8 months after transnasal surgery (tumor completely removed) | |
Frequently asked question.
Many patients are concerned about the question: will lost vision be restored after surgery? If the visual impairment lasts long enough—several months or about a year—the likelihood of normal vision being restored is low. The surgeon’s task is to preserve at least what remains. If the disorder has occurred recently, then vision (in almost one third of patients) is restored in the first days after surgery. A sharp deterioration as a result of hemorrhage into the tumor can only be corrected by urgent surgical intervention. In any case, the sooner you see a doctor, the greater the likelihood of a positive outcome.
Causes of pituitary adenoma
There are the following reasons for the development of pituitary adenoma:
- Past or developing infectious diseases of the brain (neurosyphilis, polio, meningitis, encephalitis);
- Intrauterine anomalies of fetal development;
- Consequences of traumatic brain injuries.
People suffering from these diseases are considered to be at risk for the possibility of developing a pituitary adenoma. The risk group includes men and women aged thirty to forty-five years. Pituitary adenoma does not occur in adolescents and young children. Long-term use of oral contraceptives can provoke the development of pituitary adenoma in women.
In some cases, the cause of pituitary adenoma is a family history. For patients whose relatives suffered from this disease, neurosurgeons recommend periodic preventive examinations. Pituitary adenoma does not develop under the influence of specific risk factors. The occurrence of a tumor is not related to environmental conditions, lifestyle or work specifics.
The patient's condition after surgery
With the development of pituitary adenoma, surgical treatment in many cases is the only option. The operation prevents vision loss due to damage to the optic nerve, neurological disorders due to compression of adjacent brain tissue, and the consequences of hormonal stimulation of the gonads, thyroid, and adrenal glands. However, complications in the postoperative period often occur. They require timely identification and treatment.
Degree of operational risk
The deterioration of the general condition of patients is associated with anesthesia and the surgical intervention itself. The risk of surgery increases in older patients. In this group of patients, the following often occurs:
- sudden changes in blood pressure levels - transition from vascular collapse to hypertensive crisis;
- inadequate response to medications, lack of results;
- heart rate disturbances (tachycardia, bradycardia, arrhythmia);
- development of cardiomyopathy and heart failure;
- blockage of the deep veins of the extremities, detachment of a blood clot with pulmonary embolism;
- postoperative pneumonia;
- stress ulcers of the stomach and intestines with massive bleeding.
Therefore, before removing the adenoma, the surgeon and anesthesiologist determine the degree of risk of removing the adenoma and correct cardiac dysfunction. After surgery, such patients are advised to monitor ECG and ultrasound of the abdominal organs.
We recommend reading the article about the symptoms and treatment of hypothyroidism. From it you will learn about the causes and symptoms of hypothyroidism in men and women, as well as about the diagnosis, treatment of the disease and prevention.
Find out more about diagnosing thyroid diseases here.
Reaction of neighboring structures
General cerebral complications include:
- cerebral edema;
- transient disorders of cerebral circulation;
- intracerebral and subarachnoid hematomas;
- ischemic stroke.
When stopping bleeding from a branch of the carotid artery, its blockage, narrowing or formation of a false aneurysm, and blood loss when flowing through the nasal passages are possible.
Disorders of the adrenal glands and hypothalamus
Insufficient formation of catecholamines (adrenaline, norepinephrine and dopamine) due to removal of an adenoma is a fairly common complication. It may be associated with damage to the pituitary gland during surgery, as well as previous compression of the brain tissue that produces adrenocorticotropic hormone. This condition reduces the patient's ability to withstand the stress of surgery.
When there is swelling of the brain in the hypothalamus region, hematoma or bleeding in this area, or compression of the arteries of the circle of Willis, a hypothalamic crisis occurs. Its main manifestations:
- high body temperature or its uncontrolled decrease;
- delirium, hallucinations, sudden agitation;
- pathological drowsiness with transition to a coma;
- heart rhythm disturbances - the heart rate per minute can increase to 200 beats at normal or low body temperature, and at high it can be even more;
- increased breathing;
- change in blood acidity.
Severe cardiovascular and pulmonary insufficiency leads to death.
Liquororrhea and meningitis
The discharge of clear or pinkish fluid from the nasal passages (cerebrospinal fluid rhinorrhea) appears after tumor removal due to bone defects through which the surgical approach passes. It may appear in the first days or even after a few years. Postoperative meningitis (inflammation of the choroids of the brain) occurs when the surgical field becomes infected; their risk increases with prolonged interventions.
Symptoms of pituitary adenoma
Symptoms of pituitary adenoma are most often observed in people of young and working age. The disease often leads to disability of patients. Among the clinical symptoms of pituitary adenomas are:
- Decreased visual acuity;
- Blindness;
- Headache;
- Vegetative crises;
- Pituitary insufficiency.
A symptom of pituitary adenoma in women is amenorrhea. Men and women with a pituitary adenoma may experience problems with libido or reproductive function. With hormonally inactive pituitary adenomas, the first symptoms of the disease appear when the patient reaches middle age. In patients of older age groups, the disease begins with visual and neurological disorders. In women under 50 years of age and men under 55 years of age, the first symptoms of pituitary adenoma may be sexual dysfunction. Women suddenly develop amenorrhea or menstrual irregularities. In men, the first symptom of a pituitary adenoma may be erectile dysfunction.
Sexual disorders predominantly precede visual ones, which occur within a period of several months to 2-3 years. The main complaints in patients suffering from hormonally dependent pituitary adenoma are divided into 4 groups:
- Visual (decreased visual acuity, limited visual fields, double vision, blindness, lacrimation, burning sensation in the eyeballs);
- Sexual (absence of menstruation and menstrual irregularities in women, sexual disorders in men);
- Neurological (sleep disturbances, headaches, dizziness, memory loss);
- General complaints (fatigue, weakness, thirst, drowsiness, vegetative crises, weight loss or gain).
With an inactive pituitary adenoma, 75% of patients have insufficient excretion of pituitary tropic hormones. In 30% of cases, hypothyroidism is determined, in 25% - adrenal insufficiency. Symptoms of hypogonadism due to pituitary adenoma in men are decreased libido, erectile dysfunction, and in women - amenorrhea and infertility. Hypothyroidism is manifested by the following symptoms:
- Headache;
- Depression;
- Decreased mental functions;
- Constipation;
- Increased body weight.
With growth hormone deficiency in adult patients, general resistance decreases, obesity occurs, bone mineral density decreases with an increased risk of fractures, anxiety, restlessness, and frequent mood swings appear. ACTH deficiency is manifested by the following symptoms:
- General weakness;
- Fatigue;
- Pain in muscles and joints;
- Symptoms of damage to the digestive organs;
- Loss of consciousness when getting out of bed.
Hormonally active pituitary adenomas are detected in 75% of patients. Excessive secretion of one or another hormone into the blood leads to the development of the corresponding clinical syndrome.
Prolactin in pituitary adenoma increases in patients suffering from prolactinoma. This type of pituitary adenoma occurs in 30% of women with galactorrhea (discharge of milk from the nipples) and amenorrhea. In men, prolactinomas are much less common. Pituitary adenoma, in which the level of prolactin increases, is manifested by certain clinical symptoms: impotence and infertility in men, amenorrhea and infertility in women. In men, the leading symptom of adenoma in this case is a decrease in libido and potency. Then infertility develops due to oligospermia and osteopenia. Rare manifestations of prolactinomas in men are galactorrhea and gynecomastia (swelling of the mammary glands).
Somatotropinoma is characterized by an increased level of growth hormone in the blood. This pituitary adenoma causes a progressive characteristic change in appearance. Patients' hands and feet enlarge, their facial features enlarge, and their tongue enlarges. This can cause obstruction of the upper respiratory tract, “night apnea” syndrome - stopping breathing during sleep. When metabolic disorders occur, diabetes mellitus and impaired glucose tolerance develop. Somatotropinomas can lead to thickening of the muscular layer of the ventricles of the heart, arterial hypertension, arrhythmia, endothelial dysfunction with the development of heart failure.
The main symptoms of thyrotropinoma are:
- Hyperthyroidism;
- Headache;
- Visual field defects.
Thyrotoxicosis is manifested by the following symptoms:
- Tachycardia (increased heart rate);
- Tremor (hand shaking);
- Increased body temperature;
- Exophthalmos (bulging eyes);
- Diarrhea (diarrhea).
Corticotropinoma causes secondary adrenal hypercortisolism, which is known as Cushing's disease. In patients, the face becomes moon-shaped, and fatty tissue accumulates along the back of the neck and above the collarbones. The skin becomes thinner, pinpoint hemorrhages and red-burgundy stretch marks appear on the body. Muscular dystrophy, myopathy, osteoporosis, and kyphosis develop. Patients experience pathological fractures, cataracts and diabetes mellitus. Due to immunological disorders, fungal infection occurs, acne occurs, and wounds do not heal for a long time. Due to the development of hormonal disorders in men, libido decreases, erectile dysfunction and oligospermia occur. Frequent symptoms of this type of pituitary adenoma in women are oligororrhea or amenorrhea, hirsutism (increased hair growth on the face and limbs), acne.
Clinical picture of acromegaly:
- Enlargement of limbs
- Enlargement of facial features
- Diastema (increased spaces between teeth)
- Prognathism (protrusion of the lower jaw)
- Headache
- Paresthesia
- Deepening the voice
- Pain in joints, back
- Swelling of the face and hands
- Sweating
- Marked decrease in working capacity
- Menstrual irregularities
- Decreased libido and potency
- Visual impairment
- Apnea
- Pain in the heart area
- Increased blood pressure
- Hirsutism
- Dyspnea
- Skin changes
- The next one is corticotropinoma
, a tumor that secretes adrenocorticotropic hormone. This is a very serious disease called Cushing's disease. Most often these tumors are microadenomas. It is extremely rare that they are large.
Diagnosis of pituitary adenoma
The diagnosis of “pituitary adenoma” is made by doctors at the Yusupov Hospital on the basis of:
- Patient complaints;
- Inspection;
- Data from laboratory and instrumental research methods.
Accurate diagnosis is of great importance for choosing treatment tactics. Oncologists at the Yusupov Hospital take into account age-related changes in the reference values of pituitary hormone levels. At 11-19 years of age, the normal concentration of somatotropic hormone varies from 0.6 to 11.2 mIU/l in women and from 2.5 to 12.2 mIU/l in men. After 19 years, reference values are less than 10 mIU/l in both sexes.
The reference value of somatomedin C at the age of 30-35 years is in the range of 125–311 ng/ml, and after 60 years – from 93–224 ng/ml. The concentration of follicle-stimulating hormone in men after 21 years is 0.95–11.95 mU/ml; in women it depends on the phase of the menstrual cycle. In children over 14 years of age, reference values for thyroid-stimulating hormone are in the range of 0.4–4.0 mIU/l. Comprehensive, accurate diagnosis of pituitary adenoma allows doctors at the Yusupov Hospital to quickly identify the disease and begin effective therapy.
Laboratory diagnostics for pituitary adenoma
Laboratory diagnostics are carried out using high-quality reagents and modern research techniques. It is necessary to determine the hormonal activity of a pituitary adenoma, make a diagnosis and subsequently monitor the treatment. The level of the following hormones is determined for patients:
- Prolactin;
- Somatotropin;
- Adrenocorticotropin;
- Luteinizing and follicle stimulating;
- Thyroid-stimulating;
- Cortisol, thyroxine, testosterone, estradiol.
A mandatory study is the determination of insulin-like growth factor-1.
Methods of instrumental diagnosis of pituitary adenomas
Diagnosis of pituitary adenomas at the Yusupov Hospital is carried out using modern instrumental methods:
- Craniography;
- Computer and magnetic resonance imaging;
- Multislice tomography;
- Other methods of radiation diagnostics;
- Visual field studies.
Visualization of pituitary adenomas is carried out using radiation diagnostic methods. Doctors determine the size and structure of the pituitary gland, the size, and condition of the walls of the sella turcica and surrounding tissues. In order to avoid diagnostic errors, at the Yusupov Hospital, before performing a computer (CT) or magnetic resonance imaging (MRI), craniography is performed. Tomography is carried out using the “amplification” technique. In difficult diagnostic cases, CT or MRI is performed dynamically.
Using craniography, the size and condition of the walls of the “sella turcica” are determined (structure, thickness, double-circuit, prevalence of changes). The leading method for diagnosing pituitary adenomas is magnetic resonance imaging. MRI cannot distinguish various hormonally active adenomas from each other and from hormonally inactive ones.
During a CT scan for pituitary microadenomas, doctors at the Yusupov Hospital use a technique to “enhance” the image. Computed tomography is used to differentiate pituitary adenomas from formations that contain calcifications or hyperostoses. The use of spiral computed tomography with a bolus injection of contrast agent according to the vascular program allows doctors at the Yusupov Hospital to study the vascular network of the sellar and parasellar region. For native tomographic studies of pituitary adenomas with suprasellar growth, digital subtraction angiography of cerebral vessels or spiral computed tomography is performed. To identify chiasmal syndrome, visual fields are determined.
Recovery and rehabilitation
Depending on the severity of the patient’s initial condition, the postoperative period proceeds in three main options, each of which has different approaches to recovery.
Stable
The patient has only the usual manifestations of stress - increased temperature, accelerated pulse, unstable blood pressure, psychological disorders after anesthesia (confused consciousness, disorientation), changes in tendon reflexes. As a rule, such violations disappear within 24 hours. The patient is indicated for observation for 5-7 days and discharge to his place of residence.
Subsequent treatment is carried out on an outpatient basis. It is recommended to limit physical, emotional and mental stress for a month, consult an endocrinologist, neurologist and ophthalmologist, and drug therapy.
With an increase in the affected area
Signs of dysfunction of the hypothalamus are progressing - high temperature, tachycardia. They are combined with sharp fluctuations in pressure; patients experience incoherent speech, motor restlessness, and trembling of the limbs. Such changes last for at least 7-10 days and then gradually decrease. Patients remain in the hospital under observation; they are prescribed drug therapy and follow-up examinations before discharge.
Focal cerebrovascular accident
Due to vascular damage at the surgical site, long-term hemodynamic disturbances occur. They are provoked by spasm or blockage of the arteries of the circle of Willis. Patients are found to have unstable pulse, blood pressure, temperature, seizures, speech and neurological disorders. Patients are transferred to the neurological department until cerebral circulation is restored.
With persistent signs of brain damage, consciousness is impaired, spontaneous breathing is absent, gross disturbances of movement and speech are noted, and water-salt metabolism suffers. In such cases, a stay in the intensive care unit is indicated until vital functions are stabilized.
Treatment of adenoma
How to treat pituitary adenoma? Patients suffering from pituitary adenoma are under the supervision of an endocrinologist and neurosurgeon at the Yusupov Hospital. They collectively determine treatment tactics. Complex cases of adenoma are discussed at a meeting of the Expert Council with the participation of professors and doctors of the highest category. Currently, conservative and surgical methods are used to treat the disease.
For the treatment of pituitary adenomas, radiation therapy is used as an auxiliary method. The main installations used to remove a tumor are:
- Gamma Knife;
- Linear accelerator;
- Cyber Knife;
- Proton accelerator.
If a pituitary adenoma is detected in women, treatment is carried out jointly with a gynecologist and reproductologist. Men are consulted by an andrologist.
Drug therapy for pituitary adenomas
The main drugs for the treatment of prolactinomas and hyperprolactinemic syndrome are bromocriptine (Parlodel) and cabergoline. These drugs actively affect the circulation of dopamine and norepinephrine in the central nervous system and reduce the release of serotonin. Bromocriptine has a stimulating effect on dopamine receptors in the hypothalamus. It inhibits the secretion of hormones of the anterior pituitary gland, especially somatotropin and prolactin and somatotropin.
Internal dopamine inhibits the production of these hormones. Bromocriptine does not interfere with prolactin synthesis. The drug promotes the reverse development of pituitary adenomas of various sizes and reduces the production of prolactin. Bromocriptine is used to treat prolactinomas of various sizes and as preoperative therapy.
In case of asymptomatic somatotropin in elderly patients, drug therapy is carried out with drugs that are somatostatin analogues (octreotide) and somatotropin receptor antagonists (pegvisomant). If a patient has undergone removal of a pituitary adenoma according to indications and after the operation a high concentration of somatotropic hormone remains, a recurrence of the tumor occurs, after radiation therapy the drug is continued. If there are contraindications to surgery for pituitary adenoma, radiation and drug therapy are performed.
The goal of drug treatment with corticotropin is to normalize the level of adrenal hormones in the blood. This is achieved by using drugs that inhibit cortisol production. Symptomatic treatment is also carried out, which is aimed at correcting disorders of protein and carbohydrate metabolism, treating heart failure, and normalizing blood pressure levels. Irradiation of pituitary adenoma is used for treatment with corticotropin as an addition to surgery, and as primary radiation treatment.
Surgery to remove pituitary adenoma
For thyrotropinoma (pituitary adenoma of the brain), surgery is the main method of treatment. Drug therapy is limited to maintaining normal hormone levels after surgery. For Cushing's disease, surgical removal of the pituitary adenoma is performed. For microadenomas, the effectiveness of surgical treatment reaches 70-90%, for macroadenomas - 50-60%. Surgery for gonadotropinoma is performed when the clinical manifestations of the disease are severe.
Currently, surgical treatment of pituitary adenomas is carried out by the main approaches: transnasosphenoidal (transnasal, transsphenoidal) and transcranial (intradural and extradural). Neurosurgeons use these approaches as two sequential steps. Transnasal adenoma removal is performed through the nose. The method of choice for the treatment of pituitary adenomas is transsphenoidal surgery. The transcranial method is used when it is impossible to use the transsphenoidal method.
Doctors at the Yusupov Hospital use microsurgical and endoscopic transsphenoidal access. A technique is used for microscopic removal of pituitary adenomas with auxiliary endoscopic control, using the following advantages of endoscopy:
- Powerful lighting;
- The phenomenon of endomicroscopy;
- Availability of side view.
This allows the surgeon to determine the boundaries of the pituitary adenoma during surgery and assess the location and size of the remaining unremoved tumor fragments. The lateral view of the endoscope allows you to remove the tumor from the optimal side, avoiding damage to the brain and the contents of the cavernous sinuses. If cerebrospinal fluid leaks, it is installed and eliminated during the operation. The prognosis in this case is good. The cost of surgery for pituitary adenoma depends on the method of surgical intervention, the necessary drug support during the preoperative and postoperative period.
Clinical picture of hypercortisolism:
- Arterial hypertension
- Dysplastic obesity
- Trophic skin changes
- Hirsutism
- Systemic osteoporosis
- Encephalopathy
- Secondary hypogonadism
- Secondary immunodeficiency
- Myopathy
- Nephrolithiasis
- Striae
- Edema
- Symptomatic diabetes mellitus
- Acne
Based on the fact that there are hormonally active tumors, there are specific indications for surgery.
For corticotropins, which I just mentioned, this is Itsenko-Cushing's disease.
Somatotropinomas are a syndrome of acromegaly, as the first stage, sometimes in the absence of effect from drug treatment. But surgery is still the first line help.
Prolactinoma - in the absence of effect from drug treatment, with intolerance to drugs, an allergic reaction, for example, to them. Still, we believe that the first line of treatment is drug treatment. Sometimes there are cases when prolactinoma is detected very late in a patient. It is large or gigantic in size. It greatly compressed the surrounding brain structures, causing, for example, visual impairment, called chiasmal syndrome. In this case, a consultation is held together with an endocrinologist and in certain situations we refuse drug therapy, at least preoperative, and take the patient straight away for surgery.
Thyrotropinomas and gonadotropinomas are a rare type of tumor. We won't discuss them for now.
Clinical picture of hormonally inactive adenomas
consists of the effect of the tumor mass on surrounding structures.
Because tumors do not secrete hormones, patients begin to feel or will feel it much later than hormonally active tumors.
chiasmal syndrome occurs
. This is a narrowing of the visual field. Decreased visual acuity. That is, visual disturbances occur. The tumor overcomes the empty space between the adenoma and the optic nerves, between the pituitary gland and the optic nerves and causes compression. There may be a disorder of the oculomotor nerves, that is, the nerves responsible for eye movement. Sometimes exophthalmos is possible - protrusion of the eye outward.
Sexual disorders
: amenorrhea, oligo-opsomenorrhea, lactorrhea, infertility, erectile dysfunction in men.
Various types of neurological disorders
. Cephalgic syndrome is a headache, a severe headache.
Also, large-sized formations, and most often these are inactive adenomas, can cause occlusion of the ventricular system of the brain
. What is it: a person has a special cavity in the head, the ventricles of the brain, they produce cerebrospinal fluid - this is a transparent liquid, it is produced there, it is absorbed in the spinal canal. With large tumors, these nodes can block the outflow of fluid. Liquid is produced, but there is nowhere for it to flow. This condition occurs, called hydrocephalus, or simply dropsy of the brain. Which, of course, requires some kind of urgent surgery.
Hypopituitary disorders
: secondary hypocortisolism, secondary hypothyroidism.
There is also sometimes an indication such as nasal liquorrhea
. What is it: nasal is through the nose, liquorrhea is the same cerebrospinal fluid, this liquid that drains from the nose. Large tumors with infrasellar growth, I showed you earlier, which grow downward, towards the nasal cavity, can destroy the structures of the base of the skull that I showed you (walls, main sinuses) and then this fluid can easily flow out of the nose. What is fraught with the fact that microbes through the nasal cavity (and this is not the cleanest place in humans) can enter the cranial cavity and, accordingly, cause symptoms such as inflammation. For example, meningitis is an inflammation of the membranes of the brain, which is fraught with all sorts of dangerous complications.
The absolute indication for surgery is:
- decreased visual acuity and narrowing of visual fields,
- dysfunction of the oculomotor nerves,
- impaired outflow of cerebrospinal fluid, hydrocephalus, as I said earlier,
- nasal liquorrhea,
- continued growth of the tumor, despite conservative treatment - sometimes this, unfortunately, happens - or, as I already said, in some cases prolactinoma grows, although this is not so common,
- pituitary apoplexy. What it is? Sometimes it happens, prolactinomas are especially prone to this, unfortunately, hemorrhage occurs in the thickness of the tumor, and the tumor can sharply increase in size. In this case, a person may suddenly suddenly lose vision. This may also be some kind of indication for some urgent surgical measures.
There are different accesses.
We mainly divide them into transcranial, that is, through the skull, through craniotomy - through the frontal bone, through the temporal bone. And transnasal.
Rice. 11 Transnasal access (surgical angle)
In the world, about 90 percent of tumors are now operated on using transnasal approaches.
, so we will only talk about this.
Transcranial approaches are needed only in selected cases and this is discussed separately with patients.
As I already said, access is through the nasal cavity. This is the main sinus, the air-bearing sinus, the main bone in which such a cavity is located. Trepanation of the anterior wall of the sinus and the posterior wall of the sinus is performed. And we find ourselves in this bone pocket, which is called the sella turcica, where the pituitary gland lies, from which large tumors can develop. The arrows show that even through the nasal cavity it is possible to remove large tumors that can extend far beyond the cavity of the sella turcica. This is the surgical angle that allows us to widely remove large tumors with a variety of growth patterns.
There is, of course, a lot to talk about surgical technique.
, I think it’s not worth it, but I’ll highlight the main points.
That is, there are some techniques that allow us to remove common complex tumors, large ones, for example, or those that have some interesting growth to the side: right, left, up, down, which are not visible with ordinary eyes, for example, through a microscope.
an endoscopic technique for this.
. The most important thing is the ability to look around the corner. It is not so often that the tumor is located strictly in the middle. Most often, they are still deviated from the midline and the endoscope allows us to remove them from around the corner. The surgeon removes these tumors from the patient in a less traumatic manner and is safer for the patient.
Rice. 11. Application of endoscopic technology
There is also a system called operational neuronavigation
. The essence of this system is that before the operation, the patient is given MRI images, his images are loaded into a computer, and during the operation, the surgeon can assess in almost real time how the tumor is being removed, what structures are encountered, so that it is safer for the patient.
In this case, if you see, the green one on top is the chiasma, that is, the optic nerves, and the red one is the carotid arteries. And the bottom picture shows how the surgeon removes part of the tumor. And it is clear that this is happening near the carotid artery and he must be careful and collected here so as not to damage this vessel. And it also allows you to see some of the instruments that can be registered by this operating system, neuronavigation. The surgeon knows where they are located. This is a very important point.
12 and 13 Use of surgical neuronavigation
Rice. 14. Use of surgical neuronavigation
The use of neuroendoscopy and operating neuronavigation systems allow:
- Freely navigate in a narrow and deep surgical wound (we are talking about transnasal surgery).
— Allows you to operate on complex and large tumors, I mean large tumors, which previously we could only operate with transcranial access, now, with the help of these systems, all this can be operated on calmly through the nose, including tumors with complex growth patterns that are growing in different directions. Now, with the help of an endoscope and navigation, they can also be removed.
“At the same time, surgery becomes safer for the patient and more convenient for the surgeon, and surgical trauma for the patient is reduced.
— Also, as I already told you, a bone defect forms in the walls of the main sinus. These systems allow it to be clearly visualized and closed at the end of the operation. It is extremely necessary to avoid this nasal liquorrhea that I told you about earlier, because this can lead to all sorts of complications.
“This system, all together, allows you to improve the general condition of the patient after surgery and as quickly as possible the patient returns to normal life and is quickly discharged from the hospital. Which I think is very important for the patient.
Some clinical cases
I'll show you.
- For example, (Figure 15) in the red circle is a giant pituitary adenoma
. In this case, it was a prolactinoma with suprasellar growth upward and infrasellar growth downward. The upper ones are before the operation, the lower ones are after the operation. But, as you can see, the tumor was completely removed. The patient has been under observation for several years and everything is fine. The operation was performed in one session, through the nose.
Rice. 15 Clinical case, giant pituitary adenoma
- The same. The patient I operated on came from Uzbekistan. (Figure 16) A patient who experienced pituitary apoplexy
. The patient became suddenly blind, practically blind, with only light perception. This is before the operation, and in the postoperative period. There is no tumor. The patient's vision returned. Such miracles also happen. Pituitary apoplexy - that's it. That is, the hematoma is located in the thickness of the tumor, expanding the tumor capsule. The tumor becomes significantly larger.
Rice. 16 Clinical case, pituitary apoplexy
- I will also show small formations
(Figure 17). They are no less important. This is a hormonally active somatotropinoma, that is, a tumor that secretes growth hormone. I don’t know whether you see it or not, this is a tumor, and the pituitary gland is a small white part, a piece remains. This tumor grows to the side, the black dots are the carotid arteries. It seems to grow over the carotid artery. And pictures after the operation. That is, this growth is laterosellar (to the right or to the left). And they managed to remove it, including around the carotid artery. Everything is fine, the patient continues to live peacefully.
Rice. 17. Clinical case, small formations
- Surgery of pituitary microadenomas
is also no less relevant (Figure 18). For which, by the way, the neuronavigation system is very important, which allows you to accurately visualize where the tumor is located. The arrow shows this dot. This is a microadenoma that is located in the thickness of the normal pituitary gland. And below - how it was removed. The pituitary gland was preserved, the person recovered, and continues to live well. It was corticotropinoma.
Rice. 18 Clinical case, microadenoma (corticotropinoma)
The average stay in the intensive care unit for patients is generally no more than a day.
The patient was operated on and the next day he was transferred to his room. He can be discharged within 3-6 days.
The photograph was taken on the third day after surgery. These are typical patients with acromegaly from whom growth hormone-secreting tumors and somatotropinomas have been removed.
The postoperative period is on average 3-5 days in the hospital
. Of course, this depends on many different factors.
Produced at this time:
- sanitation of the nasal cavity, if necessary, consultation with an ENT doctor.
- consultation with an endocrinologist, hormonal profile after surgery, after 2-3 months, after six months and after a year.
- MRI of the brain with contrast enhancement after 3-6 months,
- consultation with a neurosurgeon.
Many patients have a question, at least that’s what patients asked me. Look, a giant adenoma before surgery, after surgery, the picture itself was taken on the second day, and a year later. On the second day after the operation there is a question. What does it mean. If viewed, radiologists may describe this image as an unremoved tumor or an incompletely removed tumor (Figure 19)
.
Both the patient and the surgeon immediately wonder if this is really so. Look what happens in a year. A year later there is no tumor. Moreover, the fact that empty saddle syndrome has formed does happen. In this case, it did not lead to any pathological results. What does it mean? The fact is that the MRI method is the best method for identifying a pituitary tumor. But in the postoperative period, when swelling occurs in the operating room wound, when the surgeon puts a special material inside the wound during the operation, called hemostatic material, to stop the bleeding inside and to seal these bone defects. This material swells with blood and cerebrospinal fluid, and in the postoperative period it may look like this in the image (like an unremoved tumor)
. It is necessary that patients know this and not worry. That is, this is a moment that, in my opinion, is very important. Therefore, there is a standard that is accepted all over the world; this is done at least a month, one and a half to two months after the operation.
Rice. 19 MRI images before surgery, immediately after and one year later
Also applicable to hormonally active tumors. I am treating a patient with somatotropinoma, it was April 2007. The patient herself sent me this interesting graph (Figure 20), where she showed how her growth hormone GH and IFR-1 decreased. Growth hormone dropped almost immediately. And the IFR did not fall for a very, very long time
.
And eventually it returned to normal, it turns out, September 2010. The patient constantly underwent MRI of the brain with contrast. There was no tumor. But the IFR did not fall. The patient continued to be treated with the appropriate medications that you have already been told about. And in 2010 she was taken off therapy and is now being monitored. Both IGF and STH levels are normal, and there is nothing on MRI. This suggests that biochemical parameters may not always immediately decrease;
this also matters for patients.
Rice. 20 Dynamics of growth hormone, IRF-1 after surgery
I would like the following intermediate conclusion: that for a successful operation,
sufficient experience of the surgeon is necessary
. It is now believed in the world that a surgeon who operates on these tumors using a transnasal approach should have experience of approximately 200-300 patients. And approximately 30 to 50 patients per year. Then it is believed that patients have the least number of complications and the most radical removal with the lowest percentage of any unfavorable results.
I also believe that good communication between the patient and the surgeon is necessary.
, this is extremely important, because the patient must understand why he is doing all this, how he should behave in the postoperative period, and what will be done during the operation. I think this is a very important point.
Need excellent diagnostics
, MRI. Sometimes, as I said earlier, to visualize bone structures, this is a CT scan. Sometimes, in some cases when an MRI cannot be done, they operate using a CT scan. For example: a patient has a pacemaker. An MRI cannot be performed. Then you have to operate using a CT scan.
Of course it's a team effort
: that is, an ophthalmologist, neurologist, endocrinologist, neurosurgeon, radiologist, ENT doctor, sometimes a radiotherapist if radiation therapy is required.
Of course, what I said earlier. Modern surgical technology
, instruments, special hemostatic materials.
irradiate patients
, this actually does not happen that often, because it is believed that the pituitary gland may be damaged by radiation. But we do not at all want the patient to experience disorders—they are called hypopituitary disorders, that is, disruptions of the normal function of the pituitary gland.
Danger and forecasts
For pituitary adenoma, the prognosis depends on the size of the tumor, the possibility of radical removal and its hormonal activity. With timely diagnosis and adequate treatment of the disease, recovery occurs in more than 85% of patients. If the duration of the disease is short, the likelihood of complete restoration of visual function is quite high.
In case of hemorrhage into the tumor, only the immediate intervention of a surgeon can save the situation. The sooner the patient goes to the Yusupov Hospital and receives specialized medical care, the greater the likelihood of a successful cure.
Complications after removal of a pituitary tumor
The incidence of complications after surgery is related to the size of the tumor, the degree of its functional activity (hormone formation), and spread. Patients in whom the disease is detected at a late stage endure removal the most difficultly.
Their adenoma grows significantly over a long period of time and compresses the surrounding tissues, intensively produces hormones, and penetrates into neighboring structures.
In such cases, the volume of surgery increases, which can cause damage to nearby and distant brain structures. In this group, the likelihood of complications and adverse outcomes is higher.
Lost my sense of smell
Loss of smell can be caused by damage to the olfactory receptors in the nasal cavity during endonasal tumor removal. This condition is considered temporary; recovery usually occurs as the mucous membrane heals over the course of a month.
A more serious situation arises if low sensitivity to odors is part of the pituitary hormonal deficiency syndrome - panhypopituitarism. It occurs due to compression of the remaining parts of the organ by the growing adenoma.
Also, such a pathology can be a reaction to radiation therapy, which is needed when large tumors are incompletely removed. In such patients, the period of normalization of smell is longer. Its success depends on hormone replacement therapy.
Diabetes insipidus
When the secretion of the hormone vasopressin by the posterior lobe of the pituitary gland is impaired, patients develop a condition called diabetes insipidus. With this disease, there is constant thirst, and the volume of urine produced can reach 5-20 liters per day. The patient cannot go without fluid for more than 30 minutes.
Due to the location of the pituitary gland, this complication is more common with endonasal tumor removal. To treat it, a synthetic analogue of vasopressin is available in the form of drops or nasal spray.
Headache
Headache is considered one of the signs of an enlarging pituitary adenoma. After a successful operation, this symptom gradually disappears. The speed of this process largely depends on the initial size of the tumor and the state of cerebral circulation in general.
It was found that during the first month, a significant reduction in headaches was observed in less than half of those operated on. Most patients require 3 to 5 months. If pain persists, additional examination should be carried out.
Headache is considered one of the signs of an enlarging pituitary adenoma
Pituitary adenoma - treatment in Moscow
How much does it cost to remove a pituitary adenoma in Moscow? The operation to remove a pituitary adenoma is performed at an affordable price at the Yusupov Hospital. Surgeons are fluent in all techniques of surgical interventions on the pituitary gland. The cost of transnasal removal of a pituitary adenoma in Moscow is from 14,000 to 120,000 rubles.
At the Yusupov Hospital, doctors will conduct a comprehensive examination, establish an accurate diagnosis, and determine the optimal method of treating pituitary adenoma. If there are indications and there are no contraindications, the operation is performed using the latest equipment from leading European and American companies. Find out the cost of surgery to remove a pituitary adenoma by phone.
What other effective methods of treating pituitary adenoma are used in Top Ichilov?
- Conventional transsphenoidal adenoma removal (without an endoscope). If the tumor is located above the sella turcica or is large in size, it is first excised, and only when it descends into the sella turcica is it removed.
- Transcranial tumor removal using an open approach is performed in case of a large adenoma or if a malignant process is suspected
- Radiation therapy in the form of external radiation , carried out either alone or in combination with surgery. It can be quite effective if we are talking about a type of adenoma that is sensitive to radiation therapy.
- Stereotactic radiosurgery is precise irradiation of a tumor without affecting healthy tissue.
- Hormone therapy
Treatment
Many consequences of pituitary adenoma removal go away on their own. In the acute period, painkillers and antibiotics are needed. After sparing surgery, the patient is discharged home for 3-5 days. If you feel normal, there is no need for rehabilitation measures.
Hormonal
In case of adrenocorticotropic hormone deficiency, hydrocortisone (10-15 mg) or cortisol (25-37.5) mg is used. For central hypothyroidism, levothyroxine is prescribed. With a deficiency of the gonadotropic group, men need additional testosterone, women need estrogens. Gonadotropins are needed for those who want to restore fertility. In children, somatotropin must be adjusted so that they do not lag behind in growth. In adults, therapy is necessary when IGF-1 and blood glucose drop. If there is a persistent decrease in all hormones, therapy is lifelong. But in some cases their production is partially resumed. Therefore, it is necessary to monitor indicators and adjust drug doses. In case of water-salt imbalance, vasopressin is injected. Saline solution and saline mixtures are administered intravenously. Blood pressure deficiency develops frequently (according to some reports, in 30-40%). But mostly it goes away on its own in the shortest possible time.
Infections
For meningitis, a puncture is performed to reduce intracerebral pressure and take samples. To select therapy, the sensitivity of the flora in sinus secretions and cerebrospinal fluid is determined. Pending results, empirical antibiotic therapy is started.
Liquorrhea and meningeal defects
It is necessary to repeat the operation. The hole is closed with synthetic material or autoplasty is performed. To replace tissue, a part of the fascia of the thigh, omentum, and nasal septum is taken.
Other
Correction of neurological complications is an urgent task. Nerve damage can be irreversible. Sometimes the problem is corrected with surgery. Bleeding occurs intraoperatively, only in some cases in the first hours after completion of the manipulation. They are stopped by blocking and suturing the vessels. Conservative methods - hemostatic agents, tamponade. For diencephalic syndrome, adrenaline, norepinephrine, dopamine, and their synthetic analogues are used, and, if necessary, symptomatic therapy and resuscitation measures. Recovery for an uncomplicated process takes several days. Many studies draw a parallel between the number of complications and the qualifications of surgeons. The difference is 2-4%. This means that treatment in a modern clinic, with professional doctors and high-precision equipment, significantly reduces risks. Israeli specialists spend a long time studying and undergoing internships in medical centers in the country, Western Europe, and America. Therefore, postoperative problems are rare here. The optimal price-quality ratio attracts patients from all over the world.
Useful video
Watch the video about treating a pituitary tumor:
Similar articles
- Hypothyroidism: symptoms and treatment in women and men...
It is quite difficult to identify hypothyroidism; only an experienced doctor will determine the symptoms and treatment. It can be subclinical, peripheral, often hidden until a certain point. For example, in women it can be detected after childbirth, in men - after surgery or injury. Read more - Nodular goiter and surgery: indications, relapse, consequences...
If a rapidly growing diffuse nodular goiter is detected, then you should still weigh the pros and cons of removal, since the consequences are quite serious. Indications for surgical treatment are the lack of response of the thyroid nodule to medications. A relapse may then occur. Read more
- Diffuse toxic goiter: surgery as a chance...
If diffuse toxic goiter is detected, surgery becomes a chance to save lives. Endovascular surgery on the thyroid gland can be performed, or it can be more minimally invasive. But in any case, recovery is required after. Read more
- Diagnosis of thyroid diseases: methods...
A complete diagnosis of thyroid diseases includes several methods - ultrasound, laboratory, differential, morphological, cytological, radiation. There are specific examination features for women and children. Read more
- Subclinical thyrotoxicosis: main symptoms...
Subclinical toxicosis occurs mainly in areas unfavorable for the amount of iodine. Symptoms in women, including during pregnancy, are vague. Only irregular periods can indicate the problem of nodular goiter. Read more