The cerebral cortex is a multi-level brain structure in humans and many mammals, consisting of gray matter and located in the peripheral space of the hemispheres (the gray matter of the cortex covers them). The structure controls important functions and processes occurring in the brain and other internal organs.
The hemispheres (hemispheres) of the brain in the cranium occupy about 4/5 of the total space. Their component is white matter, which includes the long myelinated axons of nerve cells. On the outer side, the hemisphere is covered with the cerebral cortex, which also consists of neurons, as well as glial cells and unmyelinated fibers.
It is customary to divide the surface of the hemispheres into certain zones, each of which is responsible for performing certain functions in the body (for the most part these are reflexive and instinctive activities and reactions).
There is such a thing as “ancient bark”. This is the evolutionarily most ancient structure of the telencephalon of the cerebral cortex in all mammals. They also distinguish the “new cortex,” which in lower mammals is only outlined, but in humans forms the majority of the cerebral cortex (there is also the “old cortex,” which is newer than the “ancient” one, but older than the “new one”).
Functions of the cortex
The human cerebral cortex is responsible for controlling many functions that are used in different aspects of the human body. Its thickness is about 3-4 mm, and its volume is quite impressive due to the presence of channels connecting the central nervous system. How perception, information processing, and decision-making occur through an electrical network using nerve cells with processes.
Various electrical signals are produced within the cerebral cortex (the type of which depends on the current state of the person). The activity of these electrical signals depends on the person’s well-being. Technically, electrical signals of this type are described in terms of frequency and amplitude. A larger number of connections and neurons are localized in places that are responsible for ensuring the most complex processes. At the same time, the cerebral cortex continues to actively develop throughout a person’s life (at least until his intellect develops).
In the process of processing information entering the brain, reactions (mental, behavioral, physiological, etc.) are formed in the cortex.
The most important functions of the cerebral cortex are:
- The interaction of internal organs and systems with the environment, as well as with each other, the correct course of metabolic processes within the body.
- High-quality reception and processing of information received from the outside, awareness of the information received due to the flow of thinking processes. High sensitivity to any information received is achieved due to a large number of nerve cells with processes.
- Supporting a continuous relationship between various organs, tissues, structures and systems of the body.
- Formation and proper functioning of human consciousness, the flow of creative and intellectual thinking.
- Exercising control over the activity of the speech center and processes associated with various mental and emotional situations.
- Interaction with the spinal cord and other systems and organs of the human body.
The cerebral cortex in its structure has the anterior (frontal) sections of the hemispheres, which are currently least studied by modern science. These areas are known to be virtually impervious to external influences. For example, if these sections are influenced by external electrical impulses, they will not give any reaction.
Some scientists are confident that the anterior sections of the cerebral hemispheres are responsible for a person’s self-awareness and his specific character traits. It is a known fact that people whose anterior sections are affected to one degree or another experience certain difficulties with socialization, they pay practically no attention to their appearance, they are not interested in work activity, and are not interested in the opinions of others.
From a physiological point of view, the importance of each section of the cerebral hemispheres is difficult to overestimate. Even those that have not yet been fully studied.
Your psychologist. The work of a psychologist at school.
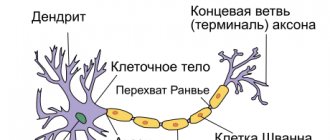
Part fourth. SENSORMOTOR ACTIVITY 4.1. Sensorimotor pathway. 4.2. Visual analyzer. 4.3. Hearing analyzer. 4.4. Speech analyzer.4.1. Sensorimotor pathway The structural unit of the nervous system is a neuron - the body of a nerve cell with processes through which it is connected to other neurons, through which nerve impulses are transmitted from neuron to neuron.
Neurons are divided into sensitive (afferent, sensory), executive (effector, motor) and intermediate (associative, intercalary). Ensembles of neurons make up the CNS - the central nervous system (spinal cord and brain) - and nerve ganglia (ganglia) located outside the central nervous system. The processes of neurons extending beyond the brain and spinal cord to various executive organs (muscles, blood vessels, glands, etc.) form the peripheral nervous system. Excitation throughout the nervous system is transmitted centripetally through afferent nerves from their endings (receptors) at the border with the external environment (extrareceptors), from the internal environment (introceptors), from tendons and muscles (propreceptors) to the central nervous system - and further along the spinal cord to the reticular formation ( providing the level of activation) and brain neurons that analyze sensory information.
The sensorimotor pathway begins with irritation of receptors, the nerve structures of which transform physical influence (light, sound, temperature, etc.) into an electrical impulse transmitted along sensitive ascending (afferent) nerves to specific (modal) sensory neurons of the spinal cord, brain stem and cerebral cortex brain (centers). The latter decipher the information of nerve impulses and form elementary sensations and holistic mental images of perception. These are the main (peripheral and central) links of the analyzers of the sensory organs (visual, auditory, tactile, olfactory, gustatory). Nervous excitation from sensory neurons, through distributive (intercalary) neurons, covers motor neurons of the central nervous system. Depending on the specifics of afferentations (sensations and sensory images), a command is sent to perform certain movements, which is transmitted along descending (efferent) motor nerves to skeletal (striated) muscles (somatic nervous system) or to the smooth muscles of internal organs and blood vessels (autonomic nervous system). The autonomic nervous system, centered in the hypothalamus, begins in the intrareceptors of the internal environment and ends with efferent fibers in the smooth muscles of the blood vessels, digestive and excretory systems, and secretory glands. In addition to the motor function, it carries out the trophic function of regulating the intensity of metabolic processes in the cells of the body. The somatic nervous system is represented by the pyramidal and estrapyramidal tracts. The central link of the pyramidal system, which carries out voluntary movements, contractions and relaxation of skeletal muscles, includes: - motor neurons (Betz pyramidal cells) of the anterior Central gyrus of the cerebral cortex; - nuclei of cranial nerves; - motor neurons of the anterior horns of the spinal cord. The peripheral part of the pyramidal system consists of motor nerves. The extrapyramidal system carries out involuntary reflation of muscle tone, maintaining balance, smoothness and emotional expressiveness of movements (facial expressions, gestures, postures). The peripheral nerve pathways of the extrapyramidal system run separately from the pyramidal ones (reticular tract). The specificity of nerve impulses carried through them is diverse and depends on the nature of the released neurotransmitters (dopamine, GABA, serotonin, etc.). The anatomical structures of the central link of the extrapyramidal system are located: - in the cerebellum; - in the nuclei of the visual thalamus (thalamus) and hypothalamus (hypothalamus); - in the striopallidal complex, which includes the basal ganglia, such as the caudate and lenticular nuclei (accumulations of gray matter of neurons in the white matter of the cerebral hemispheres), nuclei of the midbrain (substantia nigra, red nucleus); - in the vestibular nuclei of the medulla oblongata. The sensorimotor pathway, which does not reach the higher parts of the brain, the central parts of the analyzers, in which the switching of sensory excitation to motor neurons occurs mainly at the level of the spinal cord, is called a reflex arc, which performs the function of unconditioned reflexes. The inclusion of feedback into nervous activity that regulates receptor sensitivity thresholds, muscle tone, the level of neuron activation, and change or correction of motor programs turns the reflex arc into a reflex ring (N.A. Bernstein). The principle of the reflex ring underlies both unconscious (for example, adaptation of sensation thresholds to bright or dim light, loud or quiet sound) and conscious (error correction) activities. ON THE. Bernstein identified five levels, sensorimotor levels of the construction of voluntary movements from lower to higher - two subcortical and three cortical. The subcortical sensorimotor pathway at the lowest level (A) of the midbrain provides motor activity with feedback from the most ancient muscle proprioceptors and receptors of the semicircular canals of the inner ear, maintaining the tone of body posture, regulating the degree of muscle tension-relaxation (the so-called “protopathic sensitivity”). Disturbances at this level (dystonia) are manifested by symptoms of hypertension (high unregulated muscle tone), waxy flexibility with catalepsy, tremor, shaking paralysis of Parkinson's disease, static ataxia (imbalance of the body when standing, sitting). The subcortical sensorimotor pathway at a higher level (B) of the diencephalon provides movements with coordination (synergy) of the work of various muscle groups, repeatability (the simplest type of motor memory), gives them the properties of plasticity, rhythm, emotional expressiveness of facial expressions, gestural pantomimes. Smoothness, flexibility, grace of movements are the result of the work of this sensorimotor level (the so-called “extrapyramidal system”). Disturbances at level B (dyssynergia) are manifested in the case of hypofunction by a paucity of emotional and expressive movements, loss of plasticity, disorder of automatisms (for example, walking) and objective actions (skills) that require a clear rhythm. Pathological hyperfunction of level B is manifested by hyperkinesis (involuntary sweeping movements), unfocused uncontrolled athetotic (worm-like) movements (crawling, climbing, grasping-holding reflexes). The sensorimotor pathway, which closes at an even higher, already cortical level (C) of the spatial field perception analyzers and the pyramidal system of motor neurons of the cerebral cortex (Betz pyramidal cells), provides movements with adaptive properties of metricity, coordination taking into account the topography of the external environment, designing movement trajectories in it, accuracy of hitting the target, locomotor accuracy. Disturbances at this level are manifested by dynamic ataxia (disorder of coordination of movements), paralysis, paresis (partial restoration of paralysis of motor activity due to compensation from the intact extrapyramidal system). Cortical level D is responsible for performing objective actions and developing oral and written speech skills. Violations of the level are manifested by apraxia (disorders of the skills of objective activity), aphasia (speech disorders). Cortical level E provides abstract-symbolic human activity.
4.2. Visual analyzer The visual analyzer - an anatomical and functional system for perceiving light reflected from objects and constructing visual images on this basis - consists of a peripheral section (eyeballs protected by eyelids), optic nerves (with partial decussation in the opposite hemisphere of the brain) and a central section in occipital cortex of the brain. The eyeball (eye) from the side of the cranial cavity (orbit) is enclosed in a dense, opaque protein shell, the sclera. The front of the eye is additionally covered by the conjunctiva, a mucous membrane that extends from the inner surface of the eyelids. In the central zone, the conjunctiva borders on the cornea, which is transparent to light. The pupil is surrounded by the iris choroid, which also contains pigment and muscle fibers, which act as a diaphragm, narrowing (innervation from the oculomotor nerve) or expanding (sympathetic innervation) the opening of the pupil. Behind the iris there is a biconvex lens (lens), which changes the curvature of its surface (and, accordingly, the focal length) thanks to the muscle ring surrounding it. The large posterior chamber of the eye is filled with light-refracting vitreous humor. Its inner shell (retina) is the receptor zone of the analyzer with the macula (focus of vision) in the middle at the exit of the optic nerve. The retinal neuroepithelium consists of light-sensitive rods and color-sensitive cones. Visual images arise when the human eye is exposed to electromagnetic waves in the short wavelength range (0.4-0.76 microns). 4.3. Auditory analyzer In adolescence, a person distinguishes sounds in the range from 16 to 20,000 hertz, but by the age of 35, the upper limit of audible frequencies drops to 15,000 hertz. The auditory analyzer - an anatomical and functional system for the perception of sound and speech - consists of a peripheral section (outer, middle, inner ear), auditory nerve pathways (with partial crossover to the opposite hemisphere of the brain from each ear) and hearing centers (temporal cortex) . The outer ear (pinna, external auditory canal) performs a sound-conducting function. Sound can be caused not only by an air wave, but also by chemical and thermal irritants. The middle ear (tympanic cavity) allows the sound wave to be amplified. The nasopharynx, connected to the tympanic cavity by the Eustachian tube, and the temporal bone adjacent to the middle ear, the cavernous body of which is filled with air, form a joint acoustic resonance system. In the tympanic cavity, sound travels in two directions. In the lateral direction - to the temporal bone (sensations of mechanical shocks, air wave pressure), and in the main - from the eardrum through the ossicular system to the inner ear (a hammer fused to the eardrum, an anvil and stirrup, transmitting vibrations of the membrane through the oval as a vibrator window, closed by a membrane, to the fluid environment of the inner ear). The function of the auditory ossicles is to transmit and amplify (20 times) the sound wave from the eardrum to the inner ear. The inner ear is located in the temporal bone. It is a system of membranous labyrinths (channels and reservoirs) filled with tissue fluid (lymph). It consists of two structural and functional sections: the cochlea and the semicircular canals. The cochlea contains auditory nerve receptors that convert the mechanical sound wave code into nerve impulses. Thousands of thin fibers of different lengths that make up the main membrane of the cochlea resonate with sound of one frequency or another. Together, these elements form the receptor apparatus of the auditory analyzer - the organ of Corti. Three semicircular canals, located in three planes (top-bottom, left-right, front-back), constitute the vestibular (otolith) apparatus for orienting the body position in space. Nerve impulses are converted in the central sections of the auditory and speech analyzers (temporal lobes of the cerebral cortex): - into parameters of volume (amplitude, sound intensity) and pitch (frequency of the sound wave) - in the primary zones of the hearing analyzer; - into non-speech auditory images (secondary zones of the hearing analyzer) and speech images (Wernicke's area, located, as a rule, in the left hemisphere of the brain). The non-speech and speech secondary zones of the auditory and speech analyzers communicate with each other through their tertiary zones (overlap zones). 4.4. Speech analyzer Speech is a specific form of human socio-psychic activity, transmission of information, thinking, interaction, communication of people using a system of oral, written verbal (verbal) and gestural signs. In this regard, not in a narrow anatomical, but in a broad philosophical sense, language is a system of signs developed and accepted in society; sign - a method, a code for transmitting the most capacious information in a minimized form, an instrument of intellectual activity and a means of its development; a word is an auditory and visual carrier of a concept common to people and, at the same time, its individual, subjectively perceived meaning. In speech, linguistic elements are distinguished: phonemes, lexemes, semantic units. Phonemes are meaning-forming speech sounds that distinguish between letters and words. In the Russian language, phonemes are represented by vowels and consonants (voiced and voiceless, hard and soft, whistling and hissing) sounds. Other languages may have different phonemes, such as the length of a sound in English speech. Lexemes are words and phrases denoting individual objects and phenomena, the concept of which constitutes the semantic essence of speech. The characteristics of oral speech are its lexico-grammatical (words, phrases, messages), melodic-intonation (timbre, emotional coloring of the voice) and dark-rhythmic (speed of speech, pauses, stress) properties, as well as non-verbal components of expressive accompaniment of oral speech with facial expressions and gestures. At the same time, facial expressions and gestures can form an independent sign system of the language of communication. The speech analyzer has a combined sensorimotor composition with other analyzers: the voice-forming organ (peripheral department); speech centers (central department); auditory, visual and kinesthetic analyzers (peripheral and central sections of auxiliary analyzers). The central sections of the speech analyzer provide a holistic functional connection between the understanding, pronunciation and writing of words with the function of direct and reverse auditory, visual and kinesthetic information, indicating the content of oral and written speech, as well as the quality of articulation (sound pronunciation) and spelling. The vocal organ - the larynx - is the peripheral part of the oral speech analyzer. The larynx is located in the neck, in front of the esophagus, has a cartilaginous anatomical basis, and is covered inside by bicuspid elastic vocal cords, between which there is a glottis. When you inhale, the glottis expands, allowing air into the lungs. Words are pronounced as you exhale due to vibrations of the vocal cords by the air flow, which is adjusted for sound pronunciation using the muscles of the diaphragm, tongue, lips, palate, pharynx, and jaws. In this case, the role of an amplifier and sound resonator is performed by the frontonasal sinuses. The voice is characterized by strength, pitch, timbre. The strength (loudness) of sound depends on the amplitude of vibration of the vocal cords, and the height depends on the frequency of vibration associated with the frequency of incoming nerve impulses. Voice timbre is its individual characteristic (color), which depends on the composition of overtones (additional sounds due to uneven vibration of the vocal cords) and resonance in the nasopharynx and frontal sinuses. The hand is the peripheral (executive) section of the written speech analyzer and is controlled in this function by nerve conduction from the speech centers (the right hand is connected to the left hemisphere of the brain; the left - to the right due to the intersection of nerve pathways). Central speech analyzers are located, as a rule, in the left hemisphere of the brain. In the temporal lobe of the brain, Wernicke's center performs the function of understanding speech; in the frontal lobe (premotor zone of the central gyrus), Broca's center constructs the speech motor program. The process of organizing speech (phonetic, lexical, semantic coding of information), its motor (muscular) production is understood as expressive speech. Like any functional system of activity, its structure includes need (as well as the motive and purpose of speech), program (composition of speech), execution (speech) and control of utterance. In contrast to expressive, externally indicated speech (orally, in writing, by gesture), internal speech is understood as verbal thinking (with silent, subthreshold motor skills). The process of speech perception and information decoding is defined as impressive (sensory) speech.
Literature 1. Bernshtein N.A. Essays on the physiology of movements and physiology of activity. M., 1966. 2. Neiman L.V., Bogomolskikh M.R. Anatomy, physiology and pathology of the organs of hearing and speech. M., 2003.
Source: Gosudarev N.A. Special psychology: Textbook. - M.: Os-89, 2008.-288 p. Reviewers: V.I. Ekimova, Doctor of Psychology, Dean of the Academy of Psychology at Natalia Nesterova University; I. P. Krokhin, Candidate of Psychological Sciences, Associate Professor of the Department of Psychology at the Moscow State University of Service
Layers of the cerebral cortex
The cerebral cortex is formed by several layers, each of which has a unique structure and is responsible for performing specific functions. They all interact with each other, doing a common job. It is customary to distinguish several main layers of the cortex:
- Molecular. In this layer, a huge number of dendritic formations are formed, which are woven together in a chaotic manner. The neurites are parallel oriented and form a layer of fibers. There are relatively few nerve cells here. It is believed that the main function of this layer is associative perception.
- External. Many nerve cells with processes are concentrated here. Neurons vary in shape. Nothing is known yet about the exact functions of this layer.
- The outer one is pyramidal. Contains many nerve cells with processes that vary in size. Neurons are predominantly conical in shape. The dendrite is large.
- Internal grainy. It includes a small number of small neurons that are located at some distance. Between the nerve cells there are fibrous grouped structures.
- Internal pyramidal. Nerve cells with processes that enter into it are large and medium in size. The upper part of the dendrites may be in contact with the molecular layer.
- Cover. Includes spindle-shaped nerve cells. It is characteristic of neurons in this structure that the lower part of the nerve cells with processes reaches all the way to the white matter.
The cerebral cortex includes various layers that differ in shape, location, and functional components of their elements. The layers contain pyramidal, spindle, stellate, and branched neurons. Together they create more than fifty fields. Despite the fact that the fields do not have clearly defined boundaries, their interaction with each other makes it possible to regulate a huge number of processes associated with receiving and processing impulses (that is, incoming information), creating a response to the influence of stimuli.
The structure of the cortex is extremely complex and not fully understood, so scientists cannot say exactly how some elements of the brain work.
The level of a child’s intellectual abilities is related to the size of the brain and the quality of blood circulation in the brain structures. Many children who have had hidden birth injuries in the spinal area have a noticeably smaller cerebral cortex than their healthy peers.
Sensory areas of the cortex.
The area of the cortex where this type of sensitivity is projected is called the primary projection zone.
Human skin sensitivity, feelings of touch, pressure, cold and heat are projected into the postcentral gyrus. In its upper part there is a projection of the skin sensitivity of the legs and torso, below - the arms and completely below - the head.
The absolute size of the projection zones of individual areas of the skin is not the same. For example, the projection of the skin of the hands occupies a larger area in the cortex than the projection of the surface of the torso.
The magnitude of the cortical projection is proportional to the significance of a given receptive surface in behavior. Interestingly, the pig has a particularly large projection into the cortex of the snout.
Articular-muscular, proprioceptive sensitivity is projected into the postcentral and precentral gyri.
The visual cortex is located in the occipital lobe. When it is irritated, visual sensations arise - flashes of light; removing it leads to blindness. Removal of the visual zone on one half of the brain causes blindness in one half of each eye, since each optic nerve is divided at the base of the brain into two halves (forming an incomplete decussation), one of them goes to its half of the brain, and the other to the opposite.
If the outer surface of the occipital lobe is damaged, not the projection, but the associative visual zone, vision is preserved, but recognition disorder occurs (visual agnosia). The patient, being literate, cannot read what is written, recognizes a familiar person after he speaks. The ability to see is an innate ability, but the ability to recognize objects is developed throughout life. There are cases when a person blind from birth is restored to sight at an older age. For a long time he continues to navigate the world around him by touch. It takes a long time for him to learn to recognize objects using his vision.
The hearing function is provided by the precise lobes of the cerebral hemispheres. Their irritation is caused by simple auditory sensations.
Removal of both auditory zones causes deafness, and unilateral removal reduces hearing acuity. When areas of the auditory cortex are damaged, auditory agnosia can occur: a person hears, but ceases to understand the meaning of words. His native language becomes just as incomprehensible to him as a foreign language unfamiliar to him. The disease is called auditory agnosia.
The olfactory cortex is located at the base of the brain, in the region of the parahippocampal gyrus.
The projection of the taste analyzer appears to be located in the lower part of the postcentral gyrus, where the sensitivity of the oral cavity and tongue is projected.
https://www.medicinform.net/human/fisiology7_7.htm
Such zones are found in different lobes of the cortex. The zone of general sensitivity is located in the parietal lobe, the visual zone is in the occipital lobe, the auditory zone is in the temporal lobe, the gustatory zone is in the lower part of the parietal lobe, and the olfactory zone is in the two olfactory bulbs located under the cerebrum. The general sensitivity zone is located in the gyrus running along the Rolandic fissure, in the parietal lobe and receives signals from skin receptors. The entire human body - head down and toes up - is presented here in the form of areas (projections), the surface of which is proportional to the sensitivity of the corresponding parts of the body; Thus, the projection of the hand is much larger than the projections of the back or legs (Fig. A.25).
Rice. A.25. The size of the projections of sensory fibers in the comesthetic zone of the cortex is disproportionate to the size of those areas of the body from which these fibers extend (A). The same applies to the distribution of the centers of the motor zone, which are in charge of voluntary movements (B). By depicting the projections of various parts of the body in the cortex, this disproportion can be illustrated in the form of a sensory or motor homunculus.
Damage to all or any part of this area leads to a blockage of sensory signals from the corresponding areas of the body; as a result, tactile, temperature and pain sensations disappear here, although external stimuli continue to excite skin receptors and cause a flow of impulses in the nerve pathways coming from them. The association zone, located in the upper part of the parietal region, is gnostic and is responsible for the recognition and perception of stimuli that caused sensations at the level of the parietal gyrus. The zone of visual sensitivity is located in the occipital lobe along the calcarine sulcus, and the information transmitted by each retinal ganglion cell is very precisely projected to different points in it. The occipital zone of each hemisphere of the brain receives information from the opposite half of the visual field. Before entering the cerebrum, part of the fibers of both optic nerves intersect, forming the so-called optic chiasm (Fig. A.26). As a result of this crossing, the left visual lobe receives fibers from both eyes, carrying information about the right half of the visual field, and the right lobe - about the left half. Thus, as a result of the integration of nerve signals from both retinas, the brain recreates a three-dimensional image of an object, the images of which are slightly different on the right and left retinas.
Rice. A.26. Optic chiasm and visual pathways. Information about events in the right half of the visual field enters the left occipital lobe from the left side of each retina; information about the right half of the visual field is sent to the left occipital lobe from the right parts of both retinas. This redistribution of information from each eye occurs as a result of the crossing of part of the fibers of the optic nerve at the level of the optic chiasm.
Visual perception of objects, words and numbers is carried out in the associative zone located around the sensory zone. The auditory sensitivity zone is located in the temporal cortex. Each of the two temporal lobes receives information received by both ears. Therefore, even significant damage to the auditory zone cannot lead to deafness, unless, of course, it affects both cerebral hemispheres. The perception of sounds, including the interpretation of words and melodies, occurs in the association area located below the sensory area (see document 8.4). Taste and olfactory sensitivity are localized in areas located relatively close to each other. The gustatory zone is located at the base of the ascending gyrus and is responsible for deciphering nerve signals coming from the tongue. The area of olfactory sensitivity that dominates in most animals is reduced in humans to two olfactory bulbs, which are a continuation of the olfactory stripes at the base of the cerebrum.
https://www.gumer.info/bibliotek_Buks/Psihol/godfr/12.php
Prefrontal cortex
A large section of the cerebral cortex, which is represented in the form of the anterior sections of the frontal lobes. With its help, control, management, and focusing of any actions that a person performs are carried out. This department allows us to properly distribute our time. The famous psychiatrist T. Galtieri described this area as a tool with the help of which people set goals and develop plans. He was confident that a properly functioning and well-developed prefrontal cortex was the most important factor in a person’s effectiveness.
The main functions of the prefrontal cortex also include:
- Concentration, focusing on obtaining only the information a person needs, ignoring other thoughts and feelings.
- The ability to “reboot” consciousness, directing it in the right thinking direction.
- Perseverance in the process of performing certain tasks, the desire to achieve the intended result, despite the emerging circumstances.
- Analysis of the current situation.
- Critical thinking, which allows you to create a set of actions to search for verified and reliable data (checking the information received before using it).
- Planning, development of certain measures and actions to achieve set goals.
- Forecasting events.
The ability of this department to control human emotions is especially noted. Here, the processes occurring in the limbic system are perceived and translated into specific emotions and feelings (joy, love, desire, grief, hatred, etc.).
Regions
Different functions are attributed to different structures of the cerebral cortex. There is still no consensus on this issue. The international medical community now comes to the conclusion that the cortex can be divided into several large zones, including cortical fields. Therefore, taking into account the functions of these zones, it is customary to distinguish three main sections.
Area responsible for processing pulses
Impulses entering through the receptors of the tactile, olfactory, and visual centers go precisely to this zone. Almost all reflexes associated with motor skills are provided by pyramidal neurons.
This is also where the department is located, which is responsible for receiving impulses and information from the muscular system and actively interacts with different layers of the cortex. It receives and processes all impulses that come from the muscles.
If for some reason the scalp cortex is damaged in this area, then the person will experience problems with the functioning of the sensory system, problems with motor skills and the functioning of other systems that are associated with sensory centers. Externally, such disorders will manifest themselves in the form of constant involuntary movements, convulsions (of varying degrees of severity), partial or complete paralysis (in severe cases).
Sensory zone
This area is responsible for processing electrical signals entering the brain. There are several departments located here that ensure the human brain’s sensitivity to impulses coming from other organs and systems.
- Occipital (processes impulses coming from the visual center).
- Temporal (processes information coming from the speech-hearing center).
- Hippocampus (analyzes impulses coming from the olfactory center).
- Parietal (processes data received from taste buds).
In the sensory perception zone there are departments that also receive and process tactile signals. The more neural connections there are in each department, the higher its sensory ability to receive and process information will be.
The sections noted above occupy about 20-25% of the entire cerebral cortex. If the sensory perception area is damaged in some way, a person may have problems with hearing, vision, smell, and the sensation of touch. The received impulses will either not arrive or will be processed incorrectly.
Not always violations of the sensory zone will lead to the loss of some sense. For example, if the auditory center is damaged, this will not always lead to complete deafness. However, a person will almost certainly have some difficulties with the correct perception of the sound information received.
Association zone
The structure of the cerebral cortex also contains an associative zone, which ensures contact between the signals of neurons in the sensory zone and the motor center, and also provides the necessary feedback signals to these centers. The associative zone forms behavioral reflexes and takes part in the processes of their actual implementation. It occupies a significant (comparatively) part of the cerebral cortex, covering sections included in both the frontal and posterior parts of the cerebral hemispheres (occipital, parietal, temporal).
The human brain is designed in such a way that in terms of associative perception, the posterior parts of the cerebral hemispheres are especially well developed (development occurs throughout life). They control speech (its understanding and reproduction).
If the anterior or posterior parts of the association zone are damaged, this can lead to certain problems. For example, if the departments listed above are damaged, a person will lose the ability to competently analyze the information received, will not be able to make simple forecasts for the future, will not be able to build on facts in the thinking process, or will not be able to use previously acquired experience stored in memory. There may also be problems with spatial orientation and abstract thinking.
The cerebral cortex acts as a higher integrator of impulses, while emotions are concentrated in the subcortical zone (hypothalamus and other departments).
Paul Brodmann
Different areas of the cerebral cortex are responsible for performing specific functions. You can examine and determine the difference using several methods: neuroimaging, comparison of electrical activity patterns, study of cellular structure, etc.
At the beginning of the 20th century, K. Brodmann (a German researcher of human brain anatomy) created a special classification, dividing the cortex into 51 sections, basing his work on the cytoarchitecture of nerve cells. Throughout the 20th century, the fields described by Brodmann were discussed, refined, and renamed, but they are still used to describe the cerebral cortex in humans and large mammals.
Many Brodmann fields were initially defined based on the organization of neurons within them, but later their boundaries were refined in accordance with correlations with various functions of the cerebral cortex. For example, the first, second and third fields are defined as the primary somatosensory cortex, the fourth field is the primary motor cortex, and the seventeenth field is the primary visual cortex.
However, some Brodmann fields (for example, area 25 of the brain, as well as fields 12-16, 26, 27, 29-31 and many others) have not been fully studied.
Speech motor area
A well-studied area of the cerebral cortex, which is also commonly called the speech center. The zone is conventionally divided into three large sections:
- Broca's speech motor center. Forms a person's ability to speak. Located in the posterior gyrus of the anterior part of the cerebral hemispheres. Broca's center and the motor center of the speech motor muscles are different structures. For example, if the motor center is damaged in some way, then a person will not lose the ability to speak, the semantic component of his speech will not suffer, but speech will cease to be clear, and the voice will become poorly modulated (in other words, the quality of pronunciation of sounds will be lost). If Broca's center is damaged, the person will not be able to speak (just like a baby in the first months of life). Such disorders are commonly called motor aphasia.
- Wernicke's sensory center. Located in the temporal region, it is responsible for the functions of receiving and processing oral speech. If Wernicke's center is damaged, sensory aphasia will form - the patient will not be able to understand speech addressed to him (and not only from another person, but also his own). What the patient says will be a collection of incoherent sounds. If simultaneous damage to Wernicke's and Broca's centers occurs (usually this occurs during a stroke), then in these cases the development of motor and sensory aphasia is observed simultaneously.
- Center for Comprehension of Written Speech. Located in the visual part of the cerebral cortex (field No. 18 according to Brodmann). If it turns out to be damaged, then the person experiences agraphia - loss of the ability to write.
Higher cortical functions: research methods and disorders
Higher nervous activity is the neurophysiological processes that take place in the cerebral cortex and the subcortex closest to it and determine the implementation of mental functions.
1. Gnosis (recognition) - a stock of information about the world around us with constant comparison of them with the memory matrix.
— Research methods:
1) visual gnosis:
- recognition of real objects (pictures with objects),
— recognition of contour images (contours of objects),
— recognition of noisy figures (crossed out figures, superimposed images),
2) auditory gnosis:
- recognition of auditory rhythms (number of beats [2, 3, 4 beats], tempo [fast and slow]),
— reproduction of auditory rhythms (repeat the rhythm after the researcher [2 strong + 3 weak])
- recognition of everyday noises (dog barking, paper rustling).
3) spatial gnosis:
- recognition of letters and numbers (with noise and mirrored ones),
— time recognition (using a clock without numbers)
— Violations of gnosis:
1) Agnosia - a violation of recognition processes while maintaining sensitivity and consciousness:
- total agnosia - complete disorientation of a person,
- visual agnosia - impaired recognition of objects during visual perception - anterior parts of the occipital lobe (field 19),
- auditory agnosia - impaired recognition of objects by the noise they produce - Heschl’s superior temporal gyrus (field 42),
- gustatory and olfactory agnosia - impaired recognition of objects by taste and smell - insula (field 13, 14, 15, 16) ,
- spatial agnosia - impaired recognition of objects upon contact (astereognosis) - superior parietal lobule (field 5, 7),
- anosognosia - denial of the disease with an obvious defect - and autotopagnosia - violation of the body diagram, ignoring individual parts - angular gyrus of the subdominant hemisphere (field 39)
2) Distortions of perception:
- illusion - a distorted perception of a really existing object or phenomenon
— pareidolia — the formation of illusory images, the basis of which are the details of a real object
- hallucination - an image that appears in consciousness, without an external stimulus, in which an imaginary perceived object or phenomenon is located in objective mental space and is perceived by a specific sensory organ ( true , for example, taste or visual), or in subjective mental space, that is, perceived objects are not projected outward, are not identified with real objects ( false, pseudo-hallucination ).
2. Praxis (purposeful action) - the ability to perform successive complexes of conscious voluntary movements and perform purposeful actions according to a plan developed by individual practice.
— Research methods:
1) kinesthetic praxis:
- reproduction of a pose according to a visual model (poses are shown: index finger (fingers clenched into a fist), little finger (fingers clenched into a fist), rings of fingers (1 and 2, 1 and 3, 1 and 4, 1 and 5), index and middle finger (“victory”), index and little fingers (“unity”)),
- reproducing the pose according to a kinesthetic model (putting your fingers together with your eyes closed, “smoothing” your palm and asking you to repeat the pose)
2) spatial praxis (Head's tests):
- reproduction of a pose according to a visual model (straight hand in front of the chest with the palm up or down, straight hand under the chin with the palm down, straight hand under the nose with the palm down, vertical hand under the chin, vertical hand in front of the nose, right hand on the left shoulder, right hand behind the left ear).
3) dynamic praxis:
- repetition of poses according to a visual model (fist-rib-palm, drawing),
- reciprocal hand coordination (right - fist, left - palm, then vice versa)
4) ideation praxis :
- everyday poses (show lighting a cigarette, opening with a key, lighting a match)
- Apraxia - violation of focus and action plan:
1) spatial (constructive) apraxia - violation of spatial representations: right-left, top-bottom, difficulties in performing spatially oriented movements - angular gyrus of the dominant hemisphere (field 39),
2) dynamic (motor) apraxia - violation of the sequence and smoothness of movement - supramarginal gyrus of the dominant hemisphere (field 40),
3) ideational apraxia - a violation of the initiation of movements (but performs them by imitation) - field 39 and 40 of the dominant hemisphere + anterior parts of the frontal lobes.
3. Thinking is the process of reflection and cognition of essential connections and relationships of objects and phenomena of the objective world; the ability to formulate concepts, judgments and generalizations, logical operations with verbal and visual-figurative-sensory images of objects.
— Methods of thinking and methods of researching thinking
1) Analysis - dividing an object/phenomenon into its component components, synthesis - combining those separated by analysis while identifying significant connections, and comparison - comparing objects and phenomena, revealing their similarities and differences - comparing 8-10 pairs of words for commonalities and differences
2) Generalization - combining objects according to common essential characteristics, and concretization - isolating the particular from the general - “four extra”.
3) Abstraction - highlighting one aspect of an object or phenomenon while ignoring others - explanation of proverbs (“carry water in a sieve”)
— Mental retardation is a lag in mental development from one’s age while maintaining the ability to learn at a high level (with pedagogical and social neglect).
- Oligophrenia - a disorder of mental development with limited learning ability:
1) debility - maintaining adequate mental development at the everyday, everyday level,
2) imbecility - preservation of primitive motor acts and self-care skills,
3) idiocy - complete lack of speech and social maladjustment.
4. Memory is the ability to store information about events in the external world and the body’s reactions for a long time, accumulate, reproduce it many times to organize subsequent activities, and destroy information. There are mechanical and semantic memory; it consists of memorization (fixation of material), storage, recall (reproduction of material) and forgetting.
— Research methods:
1) visual memory (test 6 figures),
2) auditory memory (test 10 words),
3) spatial memory.
— Memory disorders
1) amnesia (hypomnesia) – memory loss – retrograde (for events before damage), anterograde (after damage),
2) hypermnesia - increased mechanical memory,
3) paramnesia - false memories; a mixture of past and present, as well as real and fictional events.
- confabulation - hallucination of memories, fictitious events that never took place in the patient’s life.
- pseudo-reminiscence - an illusion of memory, consisting in a displacement in time of events that actually took place in the patient’s life; the past is presented as the present.
4) sensations of “already seen” (déjà vu) or “never seen” (jema vu).
5. Speech - the use of language means to communicate with other members of the language community, the process of speaking and perception (speech activity), as well as its result (speech works recorded in memory or writing).
— Research methods:
1) nominative speech (naming objects around)
2) understanding speech (following simple and complex instructions)
3) reflected speech (repetition of sounds, words, simple sentences)
4) grammatical speech (understanding of logical constructions such as “father’s brother” and “brother’s father”)
— Speech disorders due to organic damage to the cerebral cortex:
1) Aphasia - decay of speech components with damage to cortical speech areas,
— Wernicke’s sensory aphasia – impaired understanding of oral speech, with a secondary impairment of expressive speech (cortical) [due to impaired control over one’s own speech] or without it (subcortical) – middle sections of the superior temporal gyrus of the dominant hemisphere (field 22)
1) a large number of unnecessary words , logorrhea (excessive talkativeness),
2) paraphasia (inaccurate use of words) and perseveration (monosyllabic answers to questions of different meanings)
3) with alexia (reading impairment) and agraphia (writing impairment) - cortical, and without alexia - subcortical.
- Broca's efferent motor aphasia - a combination of impairment of expressive oral speech and written speech (cortical) or only oral (subcortical) while maintaining its understanding - posterior parts of the inferior frontal gyrus of the dominant hemisphere (field 44)
1) inability to pronounce words, verbal embolus (“mu-mu” instead of any word)
- Afferent motor aphasia - impaired ability to repeat words aloud, as well as read aloud with less impaired active voluntary speech and understanding of spoken speech - the lower parts of the parietal lobe of the dominant hemisphere (damage to the connections of Wernicke's and Broca's centers).
1) literal paraphasia (rearrangement and omission of individual sounds),
2) verbal paraphasia (replacement of one word with another, similar in articulation, but different in meaning),
3) agramatisms (violations of the grammatical structure of speech).
- Acoustic-mnestic (amnestic) aphasia - while maintaining the understanding and reproduction of speech and the grammatical structure of phrases, verbal memory , difficulty in selecting the right words arises due to a decrease in vocabulary, the hint of the first syllable does not help - temporo-parietal junction (field 37).
- Optical-mnestic (amnestic) aphasia - while maintaining the understanding and reproduction of speech and the grammatical structure of phrases, verbal memory , difficulty in selecting the right words arises due to the separation of the image and the word (“what they drink from”), the hint of the first syllable helps - temporo-parietal junction (field 37).
- Semantic aphasia - violation of the grammatical logic of speech - angular gyrus of the dominant hemisphere (field 39)
— Dynamic aphasia (apraxia of speech) – retardation, poverty of speech, absence of spontaneous voluntary speech
2) Aprosodia – no perception of speech intonation while maintaining verbal information – field 22 of the subdominant hemisphere (analogous to Wernicke’s area) ,
3) Alalia – systemic underdevelopment of speech with damage to cortical speech zones in the pre-speech period (up to 2-3 years):
- Sensory alalia - impaired understanding of spoken speech while hearing is preserved (lack of speech vocabulary), motor speech is necessarily impaired,
— Motor alalia — underdevelopment of motor speech while maintaining understanding of spoken speech.
4) Agraphia - a violation of written speech - the angular gyrus of the dominant hemisphere (field 39) or with damage to the posterior part of the second frontal gyrus,
5) Alexia – reading disorder – angular gyrus of the dominant hemisphere (field 39),
6) Acalculia - violation of oral counting - angular gyrus of the dominant hemisphere (field 39),
— Acquired and congenital defects in the structure of the articulatory apparatus (NOT CORTIQUE):
1) Dysarthria - impaired pronunciation due to insufficient innervation of the vocal apparatus (“porridge in the mouth”), and nasolalia - due to impaired innervation of the soft palate (“nasal voice”)
2) Dyslalia - a violation of sound pronunciation with normal hearing and intact innervation of the articulatory apparatus.
— Functional brain disorders:
1) Stuttering - logoneurosis, a violation of the tempo-rhythmic organization of speech, caused by a convulsive state of the muscles of the speech apparatus,
2) Mutism and surdomutism - complete lack of contact or deaf-muteness of a functional nature
Thickness
All mammals that have relatively large brains (in a general sense, not in comparison with body size) have a fairly thick cerebral cortex. For example, in field mice its thickness is about 0.5 mm, and in humans it is about 2.5 mm. Scientists also highlight a certain dependence of the thickness of the bark on the weight of the animal.
With modern examinations (especially MRI), it is possible to accurately measure the thickness of the cerebral cortex in any mammal. However, it will vary significantly in different areas of the head. It is noted that in the sensory areas the cortex is much thinner than in the motor (motor) areas.
Research shows that the thickness of the cerebral cortex largely depends on the level of human intelligence. The smarter the individual, the thicker the cortex. Also, a thick cortex is recorded in people who constantly and for a long time suffer from migraine pain.
Introductory part
Exam questions:
1.24. The structure of the cerebral cortex, cyto-, myelo-, angioarchitectonics. Dynamic localization of functions in the cerebral cortex, 1-area, 2-area, 3-area cortical fields.
1.25. Sensorimotor zone of the cerebral cortex: structure, symptoms of damage.
1.29. Analyzers of the II signal system: anatomy, physiology, symptoms of damage.
1.30. Symptoms of damage to the frontal and temporal lobes. Types of aphasia.
1.32. Symptoms of damage to the occipital and parietal lobes
Practical skills:
1. Taking anamnesis in patients with diseases of the nervous system.
5. Study of speech, praxis, gnosis
Furrows, convolutions, fissures
Among the structural features and functions of the cerebral cortex, it is customary to distinguish also fissures, grooves and convolutions. These elements form a large surface area of the brain in mammals and humans. If you look at the human brain in section, you can see that more than 2/3 of the surface is hidden in the grooves. Fissures and grooves are depressions in the bark that differ only in size:
- The fissure is a large groove that divides the mammalian brain into parts, into two hemispheres (longitudinal medial fissure).
- A sulcus is a shallow depression surrounding the gyri.
However, many scientists consider this division into grooves and fissures to be very arbitrary. This is largely due to the fact that, for example, the lateral sulcus is often called the “lateral fissure” and the central sulcus the “central fissure.”
The blood supply to the parts of the cerebral cortex is carried out using two arterial basins at once, which form the vertebral and internal carotid arteries.
The most sensitive area of the cerebral hemispheres is considered to be the central posterior gyrus, which is associated with the innervation of different parts of the body.