Why does the body need B vitamins?
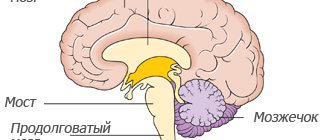
Our central nervous system, and especially its leader, the brain, simply requires sufficiently large amounts of energy for productive work.
B vitamins are involved in the synthesis of energy for the central nervous system. They are also noticed in close connections with the circulatory and cardiovascular system; without them, it also begins to “slow down”. Of course, not all B vitamins immediately perform the designated roles; each vitamin has its own “role,” and we will also talk about this in detail. But how do you know if you are lacking B vitamins?
You may notice a lack of energy, irritability, a tendency to tantrums, a basic decrease in mood, and even suspect that you are depressed. If the cause is B deficiency, the symptoms will most likely be supplemented by insomnia and loss of “former beauty” (brittle hair and nails, deterioration of skin quality).
The use of neurotropic vitamins in the treatment of patients with pain syndromes
For several decades, neurotropic vitamins have been used as part of complex treatment of patients with pain syndromes caused, in particular, by degenerative diseases of the spine.
A modern complex drug is Larigama®, 1 ml of which contains 50 mg of thiamine hydrochloride, 50 mg of pyridoxine hydrochloride and 500 mcg of cyanocobalamin. In addition, the drug contains 10 mg of lidocaine, which reduces pain and does not significantly affect the risk of unwanted side effects. The ampoule with the drug contains 2 ml of solution for intramuscular administration. In accordance with the specific clinical situation, Larigama® is administered intramuscularly at a dose of 2 ml for 5–10 days, in the future it is possible to switch to oral administration of neurotropic vitamins or less frequent administration of the drug (2–3 times/week for 2–3 weeks). , the course of treatment can be continued if necessary. As an example, we give our own clinical observation.
Clinical observation
Patient V., 54 years old, was monitored for 2 months. for spondylogenic dorsopathy, radicular syndrome L5–S1 on the left, caused by a lateral herniation of the intervertebral disc up to 5.5 mm in size at the corresponding location. He has been ill for about 4 years, exacerbations occur twice a year, the size of the hernia does not change, and he refuses surgical treatment. During the last exacerbation for 1.5 months. received two courses of nonsteroidal anti-inflammatory drugs (NSAIDs), and the pain decreased slightly (from 7 to 5 points at rest and from 8 to 6 points when moving on a visual analog scale, VAS). The patient is recommended: reflexology, local application of gel with NSAIDs, taking diclofenac and Larigama® intramuscularly 2 ml for 10 days daily, and taking analgesics if necessary. After 2 days, there was a decrease in pain intensity (from 5 to 4 points at rest and from 7 to 5 points when moving according to VAS), and after another 2 days the patient noted a significant decrease in pain intensity (up to 3 points at rest and up to 3 points when moving along VAS). It is recommended to continue treatment and begin therapeutic exercises.
As a result of a series of randomized clinical trials, a significant increase in the analgesic effect of NSAIDs, which were prescribed simultaneously with neurotropic vitamins, was demonstrated [17–20]. Thanks to this combination, the treatment time was reduced, and the dependence of the therapeutic effect on the type of NSAID used was not established.
Numerous reports of randomized trials made it possible to perform a systematic review and meta-analysis of the results obtained and evaluate the effectiveness and safety of combination therapy in patients with dorsopathies who received diclofenac (75–150 mg/day) and complex preparations of B vitamins containing thiamine, pyridoxine and cyanocobalamin in standard dosages [21]. The review examined the results of five randomized clinical trials involving 1207 patients, half of whom received NSAIDs and neurotropic vitamins (main group), while patients in the comparison group received monotherapy with NSAIDs only in comparable dosages. In the main group, there was a significant reduction in the time of pain relief by half (odds ratio 2.23; 95% confidence interval (CI) 1.59–3.13; p<0.00001). The number of patients who needed to be treated to achieve a positive effect in the main group was 9 (95% CI 6–16; p=0.003). In addition to high clinical efficacy, the combination treatment was well tolerated and had a low incidence of side effects. Thus, the number of cases of adverse events did not differ significantly in both groups (risk ratio 0.90; 95% CI 0.37–2.17; p=0.81). It should be noted that a significant proportion of patients in the main group stopped treatment ahead of schedule, thereby reducing the risk of complications of the therapy. The results of this meta-analysis indicate that combined treatment of patients with dorsalgia is effective and safe.
According to studies conducted in the Russian Federation and abroad, the simultaneous use of NSAIDs and neurotropic vitamins can not only shorten the duration of treatment for dorsalgia, but also reduce the drug load on the body, thereby reducing the risk of complications. In addition, it turned out that combination treatment in some cases improves the prognosis of the disease, increasing the duration of remission [22]. The use of neurotropic vitamins in the complex treatment of patients with vertebrogenic neurological complications is also justified if the patient has a neurological deficit caused by compression of the spinal roots.
B vitamins
Let's look at the unique roles of the seven vitamins:
B1 (thiamine)
Plays an important role in metabolism, helping to convert nutrients into energy, normalizes the condition of the cardiovascular and endocrine systems. Necessary for the protection of nerve cell membranes, transmission of nerve impulses and nutrition of the brain.
The richest food sources include pork, sunflower seeds and wheat germ.
B2 (riboflavin)
Helps convert food into energy and also acts as an antioxidant. Increases the level of hemoglobin in the blood, stimulates hematopoiesis. Improves the general condition of the nervous system.
Foods highest in riboflavin include organ meats, beef and mushrooms.
B3 (niacin, vitamin PP)
Plays a role in transmitting signals from cell to cell, normalizes inhibitory processes in the central nervous system, prevents the occurrence of neuroses and hysteria. Participates in metabolism, production and repair of DNA. It is also critically important for metabolic processes in the heart muscle, good blood circulation and normal blood clotting.
Food sources: chicken, tuna, lentils.
B5 (pantothenic acid)
Like other B vitamins, pantothenic acid helps the body obtain energy from food, and is also involved in the production of hormones, cholesterol and tissue regeneration. In the nervous system it is responsible for “feelings”, as it plays a role in the synthesis of acetylcholine, the most important substance for the transmission of nerve impulses in the central nervous system to the parasympathetic nervous system.
Liver, fish, yogurt and avocados are rich in pantothenic acid, but cooking them significantly reduces the dose.
B6 (pyridoxine)
Participates in the metabolism of amino acids, the production of red blood cells, and has a beneficial effect on the condition of blood vessels. In the nervous system, it plays a role in the creation of neurotransmitters (substances through which electrical impulses are transmitted in nerve cells). It is also responsible for the uptake of glucose by neurons and the absorption of magnesium, which ensures the transmission of nerve impulses. Pyridoxine also helps improve memory and mood, as it participates in the synthesis of serotonin.
Foods with the highest content: chickpeas, salmon and potatoes.
B9 (folic acid)
Necessary for cell growth and proper division, amino acid metabolism, formation of red and white blood cells, and prevention of anemia. In the nervous system, it is responsible for the synthesis of glycine, which has anti-stress and nootropic effects and regulates inhibition processes.
Can be obtained from leafy greens, liver and legumes.
B12 (cobalamin)
Perhaps the best known of all the B vitamins, it is vital for neurological function. Affects the formation of the sheath of nerve fibers (myelin), which protects nerve cells from destruction and strengthens the nervous system. Involved in the production of DNA and red blood cells. Improves muscle function, including the heart.
Contained in foods of animal origin: meat, eggs, seafood and dairy products.
I.A. Strokov, L.T. Akhmedzhanova, O.A. Solokha Department of Nervous Diseases MMA named after. THEM. Sechenov
Many scientists remain skeptical about the therapeutic capabilities of B vitamins, attributing their effectiveness to the placebo effect. At the same time, practitioners widely use B vitamins to treat various neurological diseases. Who is right? Do B vitamins have an effect on the pathogenetic mechanisms of various diseases? What studies have been conducted on the effectiveness of B vitamins within the framework of evidence-based medicine and what did they show? There is no doubt that if there is a lack of B vitamins in the body, there is a need to compensate for their deficiency. This is due to the fact that the lack of basic B vitamins (thiamine - vitamin B1, pyridoxine - vitamin B6, cobalamin - vitamin B12) leads to the development of pathology of the peripheral nervous system. With a chronic deficiency of thiamine in food, distal sensory-motor polyneuropathy develops, reminiscent of alcoholic and diabetic polyneuropathy. Pyridoxine deficiency leads to the development of distal symmetrical, predominantly sensory polyneuropathy, manifested by a feeling of numbness and paresthesia in the form of “pins and needles”. Cobalamin deficiency, in addition to pernicious anemia, forms subacute degeneration of the spinal cord with damage to the posterior columns, and in a relatively small number of patients - distal sensory polyneuropathy, which is characterized by numbness and loss of tendon reflexes. In developing countries, in the general population, a deficiency of B vitamins is detected quite often, but in developed countries this is not uncommon. In the USA and England, vitamin B12 deficiency is observed in 6% of the population, mainly in older age groups [8]. When examining 581 patients with polyneuropathies, B12 deficiency was detected in 4% and possible deficiency (increased methylmalonic acid content > 243 nmol/l) in 32% of patients. Administration of vitamin B12 to these patients improved their condition in 87% of cases with obvious cobalamin deficiency and in 43% of cases with possible cobalamin deficiency [33]. B vitamins can be prescribed in the absence of their deficiency due to the active participation of this group of vitamins in the biochemical processes that ensure the normal functioning of the structures of the nervous system, for example, in diabetic polyneuropathy. It is known that thiamine, localized in the membranes of nerve cells, has a significant effect on the processes of regeneration of damaged nerve conductors, and also participates in ensuring energy processes in nerve cells and the normal function of axoplasmic current. Pyridoxine supports the synthesis of transport proteins in axial cylinders; in addition, in recent years it has been shown that vitamin B6 has an antioxidant effect [30]. Cobalamin affects membrane lipids and is involved in biochemical processes that ensure normal myelin synthesis. In this regard, these B vitamins are often called neurotrophic vitamins. With long-term use of large doses of vitamins B1 and B12, no side effects from the nervous system develop. When taking pyridoxine at a dose of 500 mg/day, sensory polyneuropathy may develop. Water-soluble preparations of vitamins B1, B6 and B12 can be used as monotherapy with any vitamin, which is determined by the role of this vitamin in the pathogenesis of a particular disease. There are water-soluble forms for parenteral administration and for taking in tablet form. To quickly achieve a high concentration of vitamins in the blood and cytoplasm of cells, parenteral administration in large doses of water-soluble forms of B vitamins is used. At the same time, for most diseases, it is advisable to use not one of the B vitamins, but their complex. In this case, one vitamin has a pathogenetic effect and, in addition, other vitamins have a nonspecific positive effect on the functional state of the structures of the nervous system. The most widely used and certainly priority drug for the injection of B vitamin complex (thiamine, pyridoxine, cyanocobalamin) is Milgamma, containing 100 mg of thiamine and pyridoxine, and 1,000 mcg of cyanocobalamin. If there are indications for therapy, treatment begins with 10 injections of large doses of water-soluble forms of B vitamins. Thus, the drug Milgamma, containing 100 mg of thiamine and pyridoxine, and 1,000 mcg of cyanocobalamin, is the optimal choice due to a balanced complex of neurotropic vitamins in optimal therapeutic doses . Milgamma injections are practically painless due to the presence of 20 mg lidocaine and a small (2 ml) ampoule volume. After parenteral administration of B vitamins, there may be a need for their long-term use in the form of oral administration or such a need exists from the very beginning of treatment. The use of water-soluble B vitamins for treatment in the form of tablets has limitations, which primarily concern thiamine. The fact is that the bioavailability of small doses of water-soluble thiamine is extremely low due to the fact that they are destroyed in the intestines by thiaminases. When increasing the dose of water-soluble thiamine, a “saturation” effect occurs when, despite increasing the dose, its concentration in the blood does not increase significantly, which is associated with blocking its transfer from the intestine to the blood. In this regard, the widely used drug Milgamma compositum (dragees) contains 100 mg of fat-soluble benfotiamine and 100 mg of pyridoxine. The standard therapeutic dose is to take 3 tablets per day for 2-3 months. Why is it necessary to replace water-soluble thiamine with benfotiamine, a lipophilic substance with thiamine-like activity? A group of fat-soluble substances with thiamine-like properties - allithiamins - were first synthesized in Japan by a group of scientists led by Taizo Matsukawa (Takeda, 1952) and described in detail by Motonori Fujiwara in (Takeda) 1958. The ultimate goal of scientists was to find an effective means of combating the beriberi disease that was raging in Japan in those years. Allithiamins are resistant to the action of intestinal thiaminases I and II and are therefore better absorbed. Among all the compounds in this group, benfotiamine showed the greatest bioavailability and ability to penetrate the nerve fiber [17]. Comparative studies of the bioavailability of benfotiamine and water-soluble thiamine showed that benfotiamine provides the highest concentration of the substance in plasma, red blood cells, cerebrospinal fluid, liver, peripheral nerves and is retained in the body for a longer time [36]. Thiamines and benfotiamine affect metabolic processes in the cell after being converted into a physiologically active compound - thiamine diphosphate. The ability of benfotiamine to penetrate into cells is much higher than that of water-soluble thiamines, which determines the higher intracellular level of thiamine diphosphate when taking benfotiamine. This explains why drugs containing benfotiamine, mainly Milgamma compositum, are used for long-term and preventive treatment of various diseases. Thiamine deficiency plays a major role in the development of alcoholic polyneuropathy (ALP), which in Russia is one of the most common forms of generalized damage to peripheral nerves. Alcohol-induced damage to peripheral nerves occurs in 10% of people suffering from alcoholism, mainly at the age of 40-70 years and can be detected in both men and women [46]. LSA begins in the distal lower extremities and may then involve the proximal legs and distal arms as the process progresses. In most cases, alcoholic polyneuropathy develops slowly, although there are cases of acute development of polyneuropathy in patients with alcoholism [5], which can also be observed in non-alcoholic thiamine deficiency [25]. The cause of the formation of alcoholic polyneuropathy may be the direct toxic effect of ethanol and its metabolites (acetaldehyde) and the lack of thiamine intake in the body, including those associated not only with poor nutrition of patients with alcoholism, but also due to malabsorption syndrome. Patients with alcoholism have an increased risk of insufficient supply of all B vitamins [13]. A controlled study on 78 healthy volunteers showed that constant use of vodka or red wine for 2 weeks significantly reduced plasma vitamin B12 levels [16]. In all cases of ALP, the axonal nature of nerve damage is revealed. ALP without thiamine deficiency is characterized by slow onset, predominantly sensory symptoms, severe pain and burning legs, and axonal degeneration of small fibers is found in the sural nerve. In the presence of thiamine deficiency, ALP often begins acutely with muscle weakness and impairment of deep sensitivity, and in the sural nerve, during biopsy, changes and death of thick nerve fibers are primarily detected. One of the first studies of the use of thiamine in ALP in 12 patients with alcoholism and ALP revealed a decrease in sensory symptoms in 10 patients with a duration of therapy of 2 weeks; with longer use of thiamine in 2 patients for 8 weeks, sensitivity, muscle strength and reflexes improved [43 ]. In the controlled study “BAP 1 STUDY” (Benfotiamine in Treatment of Alcoholic Polyneuropathy), for the treatment of ALP for 8 weeks in the first group of patients (30 patients), benfotiamine was used orally at a dose of 320 mg/day, in the second group (26 patients) - orally a combination of benfotiamine, pyridoxine and cyanocobalamin, and in the third group (28 patients) - oral placebo [45]. Benfotiamine improved vibration sensitivity, muscle strength and the condition of patients on a scale of neuropathic disorders in both groups receiving only benfotiamine or its combination with other B vitamins. Modern studies have shown that benfotiamine significantly reduces the intensity of pain in ALP. In 14 men with ALP, benfotiamine administered orally at a dose of 450 mg/day for 2 weeks and then at a dose of 300 mg/day for an additional 4 weeks was noted to reduce pain, sensory and motor deficits, and improve EMG parameters [1, 2]. . It is possible that the decrease in pain intensity during treatment with ALP is due not only to the replenishment of thiamine deficiency, but also to the direct antinociceptive effect of the drug. In a multicenter, randomized, double-blind, placebo-controlled study, 325 patients with positive and negative symptoms of PAL and changes in vibration sensitivity received oral B complex vitamins for 12 weeks [34]. The first group of patients received a B complex of vitamins, the second group of patients additionally received folic acid (1 mg), and the third group received placebo. A significant reduction in pain intensity was noted compared to the placebo group (p The ability of B vitamins to reduce pain until recently was questioned, since the mechanisms of their action in various pain syndromes were not known. However, the antinociceptive effect of pyridoxine and cobalamin is well known clinicians: for example, vitamin B12 has been used in various countries for the treatment of pain since 1950. Research in recent years has created a serious theoretical basis confirming the antinociceptive effect of B vitamins in nociceptive and neuropathic pain. A number of experimental studies have revealed a clear antinociceptive effect of individual vitamins and their complexes in neuropathic pain. With compression of the dorsal ganglion or ligation of the sciatic nerve, vitamins B1, B6 and B12 administered intraperitoneally reduced temperature hyperalgesia. Repeated administration of B vitamins caused a persistent decrease in temperature hyperalgesia, and the combination of B vitamins had a synergistic effect in both models of neuropathic pain [44]. In an experiment with tactile allodynia caused by a ligature applied to the spinal root, it was shown that B vitamins (thiamine, pyridoxine, cyanocobalamin) significantly reduce allodynia, and the most pronounced dose-dependent effect was observed with the introduction of B12 (73% of cases) and thiamine (58% of cases). cases). Simultaneous administration of thiamine or cyanocobalamin with dexamethasone significantly increased the antiallodynic effect (90% of cases) [10]. In a similar experimental model of neuropathic pain, it was shown that benfotiamine and cyanocobalamin can significantly reduce pain, and the best effect was obtained when combining vitamins B1 and B12 with gabapentin. In high doses, gabapentin, when prescribed as monotherapy for the treatment of pain, significantly reduced allodynia, but caused coordination problems. The combination of gabapentin with benfotiamine or cyanocobalamin achieved a similar effect on pain with a lower dose of gabapentin and without changes in coordination [29]. The effect of vitamin B12 on neuropathic pain is confirmed by the fact that it reduces experimental tactile allodynia caused by a spinal root ligature, but this does not do diclofenac, which is not a drug for reducing neuropathic pain [15]. The effect of B vitamins on the activity of nociceptive neurons of the central nervous system was studied. The experiment showed that the activity of nociceptive neurons upon stimulation of the C-fibers of the sciatic nerve with injections of vitamin B6 and the complex of vitamins B1, B6 and B12 decreases in a dose-dependent manner. Injections of vitamin B6 and B12 reduced nociceptive activity to a greater extent than vitamin B1. Multiple repeated injections are more effective than a single dose of B vitamin complex [22]. Vitamin B12 is able to reduce the release of the excitatory neurotransmitter glutamate in the nerve terminals of the central nervous system [21]. B vitamins also have an effect on nociceptive pain. In an experiment with a formaldehyde model of “inflammatory”, i.e. nociceptive, pain, the antinociceptive effect was determined with oral administration of diclofenac, its combination with vitamins B1, B6, B12, or only with B vitamins. It was shown that there is a synergistic effect of diclofenac and vitamins group B in relation to the studied form of pain syndrome. An experiment with a formaldehyde model of nociceptive pain showed the antinociceptive effect of a combination of B1, B6 and B12, which suggests the effect of a combination of B vitamins on the synthesis and effects of inflammatory algogens [14]. In an experiment on healthy and diabetic animals, the effect of benfotiamine on inflammatory and neuropathic pain was studied. Benfotiamine significantly reduced nociceptive and neuropathic pain accompanied by tactile allodynia [35]. An experiment on mice revealed that thiamine dose-dependently reduces acute and chronic neuropathic and inflammatory pain [31]. In the experiment, thiamine dose-dependently reduced temperature hyperalgesia caused by compression of the dorsal ganglion and reduced the hyperexcitability of dorsal ganglion neurons mainly in small neurons, normalizing the current of sodium ions in them [38]. It can be assumed that the antinociceptive effect of thiamine is realized through a decrease in the activity of various isoforms of protein kinase C. In 1992, when treated with a complex of B vitamins (pyridoxine, thiamine, cyanocobalamin) for 3 weeks, 1,149 patients with pain syndromes and paresthesias caused by polyneuropathies, neuralgia, radiculopathies, mononeuropathies, a significant decrease in the intensity of pain and paresthesia was noted in 69% of cases [12]. In a review of studies on the antinociceptive effect of vitamin B complex (B1, B6, B12), I. Jurna in 1998, having analyzed the experimental and clinical studies available at that time, came to the conclusion that their use can reduce both musculoskeletal and and radicular back pain. The effectiveness of vitamin B complex as an adjuvant therapy when using nonsteroidal anti-inflammatory drugs (NSAIDs) has been particularly noted [23]. In a controlled study of the effectiveness of treatment with intramuscular injections of vitamin B12 at a dose of 1,000 mcg for 10 days in 60 patients with chronic lumbago and lumbar compression radiculopathies, a significant decrease in pain intensity, assessed on a visual analogue scale (VAS), was noted compared with placebo, despite the fact that the initial pain intensity was more than 60 mm [28]. When comparing the effectiveness of parenteral administration of vitamin B12 and nortriptyline in two groups of 50 patients with painful diabetic polyneuropathy, it was found that vitamin B12 was more effective in reducing burning and shooting pain, paresthesia and a feeling of coldness [42]. In Germany and Russia, the effectiveness of B vitamins as adjuvant therapy in the treatment of back pain with diclofenac has been studied. In the study of domestic neurologists, when comparing groups of patients who parentely received the drug Milgamma or Decolofenac, high efficiency of monotherapy in the back with Milgamma was revealed. Combined therapy with Diclofenac and Milgamma more pronounced reduced back pain than monotherapy with any of these drugs, however, Milgamma monotherapy was better for tolerance and safety [3]. Experimental and clinical studies of the action of group B vitamins with nociceptive and neuropathic pains allow us to believe that in individual vitamins of this group (B1, B6, B12) and complex drugs of B vitamins (Milgamma, Milgamma Compositum) there is a pronounced antinocyceptive effect. In this regard, the possibility of using group B vitamins in the treatment of tunnel syndromes is of interest. Carpal syndrome is the most common version of tunnel neuropathies. In a large examination of 994 patients with a carpal channel syndrome, it was shown that with traditional treatment with additional prescription of vitamin B6, symptoms decreased in 68 % of patients, and with similar treatment without pyridoxine - only in 14.3 % of patients [24]. In a review of 14 studies devoted to the effectiveness of pyridoxine in carpal syndrome, it was revealed that the results of 8 works confirm the fact of reducing clinical manifestations and electrophysiological disorders in carpal syndrome as a result of the administration of vitamin B6. This can be associated either with the antinociceptive effect of B6 or hidden deficiency of vitamin, since it is known that with its deficiency, paresthesia and numbness in the hands can occur. In the treatment of diabetic polyneuropathy (DPN), the effect of thiamine on the biochemical processes of glucose metabolism is used. The formation of DPN is associated with a blockade of glucose metabolism and the accumulation of intermediate products that launch the main mechanisms that form cellular pathology, first of all, the formation of a large amount of Ages (Advanced Glicated End Products - ultimate products of excess glycation) [9]. An enzyme transcetic enzyme can reduce the content of intermediate glucose metabolism, the activity of which depends only on thiamine [18]. It is proved that thiamine is able to inhibit the formation of Ags in experimental animals and humans. It is important that the action of thiamine in DPN is not associated with its deficiency, but with the activation of transcetolase. When using thiamine, the activity of the main metabolic processes that form pathological changes in cellular structures and vascular wall decreases. On the other hand, in some experimental work, data were obtained indicating the possible direct antioxidant effect of benfotiamine [37]. The experiment demonstrates the ability of Tiamin to reduce hypoperfusion and improve tissue oxygenation, restore endothelium -dependent vasodilation and inhibit apoptosis. At the same time, it cannot be excluded that when using a combination of thiamin with pyridoxine (the drug Milgamma Compositum) for the treatment of patients with DPN, a certain effect on the pathogenetic mechanisms of DPN formation has not only thiamine, but also pyridoxine. It is shown that the pyridoxal-5'-phosphate, the active form of pyridoxine, prevents the progression of the late complications of the diabetes, inhibiting the formation of Ages [32]. Vitamin B12 is also able to cause a decrease in the manifestations of DPN. An analysis of seven clinical controlled studies performed in the world from 1954 to 2004, which studied the effectiveness of vitamin B12 in DPN, shows that its use can reduce pain and paresthesia, symptoms of damage to the autonomous system [41]. Currently, drugs of a complex of vitamins of group B are no less broadly than antioxidants are used to treat DPN. Basically, drugs of tiamin, pyridoxine, cyanocobalamin, as well as benfotiamine containing large doses of drug components (Milgamma and Milgamma compositum preparations) are used. These drugs can improve the structural and functional state of the peripheral nerves in DPN due to the active effect on the condition of the nerve fibers. In 1989, a double blind placebo-controlled study of the effectiveness of benfotiamine was carried out in combination with vitamins B6 and B12 in DPN in 20 patients with diabetes. Treatment for 3 weeks led to a reliable decrease in pain, paresthesia and improvement of vibration sensitivity compared to placebo [26]. In a controlled study, 40 patients with DPN have a reliable decrease in positive neuropathic symptoms compared to placebo (pain, burning, numbness, paresthesia) with 3-week-old Benfotiamin treatment [19]. The effect of prolonged use of benfotiamine is studied in a randomized placebo-controlled double blind examination, in which a drug containing 40 mg of benfotiamine, 90 mg of pyridoxine and 0.25 mg of cyanocobalamin was prescribed for 24 patients for 14 days in a hospital (two capsules per day) and then) and then) and then Another 10 weeks outpatient (one capsule per day). It is noted that in patients who received a combination of group B vitamins significantly increased the rate of excitation of excitement along the fibula (p = 0.006), and this effect was preserved during the examination after 9 months [39]. The effectiveness of the combination of benfotiamine (100 mg) and pyridoxine (100 mg) was investigated in 14 patients with DPN, who received the drug Milgamma compositum one drame 3 times a day for 6 weeks. After the treatment, the severity of all neuropathic symptoms (pain, numbness, paresthesia, chilliness) has significantly decreased, vibrational sensitivity and autonomous innervation (a decrease in tachycardia, an increase in the variability of the heart rhythm, a decrease in latent and an increase in the amplitude of the caused skin sympathetic response) improved. A reliable improvement in the function of somatic and autonomous nerves was noted from the 3rd week of treatment [4]. In the treatment of DPN, a more pronounced effect of benfotiamine was noted in combination with pyridoxine, compared with water -soluble groups of the group [7]. In a placebo-controlled study, the effectiveness of various forms of group B vitamins was studied in 70 patients with DPND [6]. Within 6 weeks, one group (40 patients) received the drug Milgamma Compositum, the second group (15 patients) - vitamins B1 and B6 (100 mg of each) V/m and the third group (15 patients) - placebo. In the group of patients who received Milgam compositum, there was a significant decrease in the intensity of shooting pain, burning, numbness, paresthesia on the TSS scale compared to the placebo group. The neurological deficit rated in points on the Nisll (Neuropathy Impairment Score scale), after 6 weeks, decreased significantly in the group of patients who received the drug Milgamma Compositum, compared with the group taking water -soluble vitamins of the group B, and the placebo group. Based on the results of electrophysiological testing, when taking Milgamma compositum, a reliable improvement in the function of the unlice and calf nerves, as well as autonomous nerves, was noted. An important advantage of work was to compare clinical and electrophysiological data with the concentration of thiamine in blood plasma and hemokalizate. Against the backdrop of parenteral administration, there was a faster increase in the concentration of thiamine in plasma and hemokolizate, however, from the 14th day of treatment, the concentration of thiamine in plasma against the backdrop of the intake of Milgamma compositum significantly exceeded the patients who received in/m water-soluble thiamine (p controlled clinical studies, showing the possibility of the use of benfotiamine for the preventive purpose to prevent the development of late complications of diabetes, was not carried out. A specific guideline gives a pilot study of 9 patients with type 1 diabetes that did not have any late complications of diabetes, who received benfotiamine for simultaneously (300 mg 2 times within 28 days per day) and alpha lipoic acid (600 mg 2 times a day) [11]. Against treatment, there is an increase in the activity of the transcetic enzyme by 2-3 times, which led to a decrease in the content of intracellular ages and a decrease in the hexamine glucose utilization. Interestingly, interesting that with a decrease in the activity of the main biochemical mechanisms that determine the development of late complications, patients have no changes in hyperglycemia. The study showed that in a patient of diabetes, when using benfotiamine, in combination with alpha-lipoic acid, the same metabolism improvements are observed as in experimental models of diabetes on rats when using benfotiamine. Summarizing the currently experimental and clinical data on the pathogenetic effects and clinical effectiveness of B vitamins B, we can conclude on the advisability of prescribing drugs by Milgamma and Milgamma compositum in the forms of the pathology of the nervous system.
Literature 1. Anisimova E.I., Danilov A.B. The effectiveness of benfotiamine in the treatment of alcoholic polyneuropathy // Journal of Neurology and Psychiatry named after. S.S. Korsakov. 2001; 4: 216-221. 2. Anisimova E.I., Danilov A.B. Neuropathic pain syndrome: clinical and neurophysiological analysis // Neurol journal. 2003; 10: 15-22. 3. Danilov A.B. B vitamins in the treatment of acute back pain: myth or reality? // Attending doctor. 2007; 4:1-8. 4. Sadekov R.A., Danilov A.B., Vein A.M. Treatment of diabetic polyneuropathy with Milgamma 100 // Journal of Neurology and Psychiatry. 1998; 9:30-32. 5. Strokov I.A., Alekseev V.V., Aizenberg I.V., Volodina A.V. Acute alcoholic polyneuropathy // Neurological journal. 2004; 9:1:45-50. 6. Markina O.A. The importance of the dosage form and route of administration of B vitamins to ensure effective treatment of diabetic polyneuropathy // Clinical pharmacology and therapy. 2003; 2:6-9. 7. Chernysheva T.E. B vitamins in complex therapy of diabetic neuropathy // Ross Med Vesti. 2001; 4: 48-51. 8. Allen LH How common is vitamin B12 deficiency // Am J Clin Nutr. 2009: 89: 2: 6935-6965. 9. Brownlee M. The pathobiology of diabetic complications: a unifying mechanism // Diabetes. 2005; 54: 1615-1625. 10. Caram-Salas NL, Reyes-Garcia G., Medina-Santillián R. et al. Thiamine and cyanocobalamin relieve neuropathic pain in rats: synergy with dexamethasone // Pharmacology. 2006; 77:2:53-62. 11. Du X., Edelstein D., Brownlee M. Oral benfotiamine plus alfa-lipoic acid normalizes complication-causing pathways in type 1 diabetes // Diabetilogia. 2008; 51: 1930-1932. 12. Eckert M., Schejbal P. Therapy of neuropathies with a vitamin B combination. Symptomatic treatment of painful diseases of the peripheral nervous system with a combination preparation of thiamine, pyridoxine and cyanocobalamin // Fortschr Med. 1992; 110:29:544-548. 13. Fairfield KM, Fletcher RH Vitamins for chronic disease prevention in adults: scientific review // J Americ Medic Assoc. 2002; 287: 3116-3126. 14. Franca DS, Souza AL, Almeida KR, et al. B vitamins induce an antinoceceptive effect in the acetic acid and formaldehyde models of nociception in mice // Eur J Pharmacol. 2001; 421:3:157-164. 15. Granados-Soto V., Sánchez-Ramirez G., La-Torre MR et al. Effect of diclofenac on the antiallodinic activity of vitamin B12 in a neuropathic pain model in the rat // Proc West Pharmacol Soc. 2004; 47: 92-94. 16. Gibson A, Woodside JV, Young IS et al. Alcohol increases homocysteine and reduces B vitamin concentration in healthy male volunteers – a randomized, crossover intervention study // OJM. 2008; 101:11:881-887. 17. Greb A., Bitsch R. Comparative bioavailability of various thiamine derivatives after oral administration // Int J Clin Pharmacol Ther. 1998; 36: 216-221. 18. Hammes HP, Du X, Edelstein D et al. // Benfotiamine blocks three major pathways of hyperglycemic damage and prevents expirimental diabetic retinopathy // Nature Med. 2003; 9:1-6. 19. Haupt E. Doppelblinde, placecokontrollierte untersuchung zur klinischen wirksamkeit und vertuglichkeit von benfotiamin ankermann dragees bei diabetischen polyneuropathien // Kongreubericht. 1995; 32: 2. 20. Haupt E., Ledermann H., Köpcke W. Benfotiamine in the treatment of diabetic polyneuropathy – a three-week randomized, controlled pilot study (BEDIP study) // Int J Clin Pharmacol Ther. 2005; 43: 71-77. 21. Hung KL, Wang CC, Huang CY et al. Cyanocobalamin, vitamin B12, depresses glutamate release through inhibition of voltage-dependent Ca2+ influx in rat cerebrocortical nerve terminals // Eur J Pharmacol. 2009; 602: 2-3: 230-237. 22. Jurna I., Carrison KH, Kömen W. et al. Acute effects of vitamin B6 and fixed combinations of vitamin B1, B6 and B12 on nociceptive activity evoked in the rat thalamus: dose-response relationship and combinations with morphine and paracetamol // Klin Wochenschr. 1990; 68:2:129-135. 23. Jurna I. Analgesic and analgesia-potentiating action of B vitamins // Schmerz. 1998; 12:2:136-141. 24. Kasdan M., Janes C. Carpal tunnel syndrome and vitamin B6 // Plast Reconstr Surg. 1987; 79: 456-458. 25. Koike H., Ito S., Morozumi S. et al. Rapidly developing weakness mimicking Guillain-Barre syndrome in berybery neuropathy: two case reports // Nutrition. 2008; 24: 7-8: 776-780. 26. Ledermann H., Widey KD Behandlung der manifesten diabetichen polyneuropathie // Therapiewoche. 1989; 39: 1445-1449. 27. Li SF, Jacob J, Feng J et al. Vitamin deficiencies in acutely intoxicated patients in the ED // Am J Emerg Med. 2008; 26: 7: 792 -795. 28. Mauro GL, Martorana U, Cataldo P et al. Vitamin B in low back pain: a randomized, double-blind, placebo-controlled study // Eur Rev Med Pharmacol Sci. 2000; 4:3:53-58. 29. Mixcoatl-Zecuatl T., Quinonez-Bastidas GN, Caram-Salas NL et al. Synergistic antiallodinic interaction between gabapentin or carbamazepine and either benfotiamine or cyanocobalamin in neuropathic rats // Methods Find Exp Clin Pharmacol. 2008; 30: 431-441. 30. Mooney S, Leuendorf JE, Hendrickson C et al. Vitamin B6: a long known compound of surprising complexity // Molecules. 2009; 14: 1: 329-351. 31. Moallem SA, Hosseeinzaden H., Farahi S. A study of acute and chronic anti-nociceptive and anti-inflammatory effects of thiamine in mice // Iran Biomed J. 2008; 12:3:173-178. 32. Nakamura S., Li H., Adijiang A. et al. Pyridoxal phosphate prevents progression of diabetic nephropathy // Nephrol Dial Transplant. 2007; 22:8:2165-2174. 33. Nardin RA, Amic AN, Raynor EM Vitamin B(12) and methylmalonic acid levels in patients presenting with polyneuropathy // Muscle Nerve. 2007; 36:4:532-535. 34. Peters TJ, Kotowicz J, Nyka W. et al. Treatment of alcoholic polyneuropathy with vitamin B complex: a randomized controlled trial // Alcohol and Alcoholism. 2006; 41: 636-642. 35. Sánchez-Ramírez GM, Caram-Salas NL, Rocha-Gonzáles HI et al. Benfotiamine relieves inflamatory and neuropathic pain in rats // Eur J Pharmacol. 2006; 150: 1-2: 48-53. 36. Schreeb KH, Freudenthaler S, Vormfelde SV et al. Comparative bioavailability of two vitamin B1 preparations: benfotiamine and thiamine mononitrate // Eur J Clin Pharmacol. 1997; 52: 773-788. 37. Schmid U., Stopper H., Heidland A. et al. Benfotiamine exhibits direct antioxidant capacity and prevents induction of DNA damage in vitro // Diabetes Metab Res Rev. 2008; 24:5:371-377. 38. Song XS, Huang ZJ, Song XJ Thiamine suppressed thermal hyperalgesia, inhibits hyperexitability, and lessens alterations of sodium currents in injured, dorsal root ganglion neurons in rats // Anesthesiology. 2009; 110:2:387-400. 39. Stracke H., Lindermann A., Federlin K. A benfotiamine-vitamin B combination in the treatment of diabetic polyneuropathy // Exp Clin Endocrinol Diabetes. 1996; 104: 311-316. 40. Stracke H., Gaus W., Achenbach U. et al. Benfotiamine in diabetic polyneuropathy (BENDIP): results of a randomized, double blind, placebo-controlled clinical trial //Exp Clin Endocrinil Diabetes. 2008; 116:1-6. 41. Sun Y., Lai MS, Lu CJ Effectiveness of vitamin B12 on diabetic neuropathy: systematic review of clinical controlled trials // Acta Neurol Taiwan. 2005; 14:2:48-54. 42. Tafaei A., Siavash M., Majidi H. et al. Vitamin B(12) may more effective than nortriptyline in improving painful diabetic neuropathy // Int J Food Sci Nutr. Feb 2009; 12:1-6. 43. Victor M., Adams RD On the etiology of the alcoholic neurological diseases. With special references to the role of nutrition // Am J Clin Nutr. 1961; 9: 379-383. 44. Wang ZB, Gan Q., Rupert RL, Zeng YM, Song XJ Thiamine, pyridoxine, cyanocobalamin and their combinatuin inhibit thermal, but not mechanical hyperalgesia in rats with primary sensory neuron loss // Pain. 2005; 114: 266-277. 45. Woelk H., Lehrl S., Bitsch R. et al. Benfotiamine in treatment of alcoholic polyneuropathy: an 8-week randomized controlled study (BAP I STUDY) // Alcohol&Alcoholism. 1998; 33: 631-638. 46. Zambelis T., Karandreas N., Tzavellas E. et al. Large and small fiber neuropathy in chronic alcohol-dependent subject // J Periph Nerv Sys. 2005; 10: 375-38.
Nonsteroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs (NSAIDs) are first-line drugs in the treatment of back pain of any origin; we widely use diclofenac from this group of drugs. The advantages of this drug, as shown by our experience and data from a number of clinical studies, include well-pronounced anti-inflammatory and analgesic effects and a rapid onset of action. However, the use of NSAIDs can cause so-called class-side effects from the gastrointestinal tract and cardiovascular system, which are inherent to one degree or another in all drugs in this group. Therefore, in recent years, we often prescribe to patients the drug Neurodiclovit, which is a combination in one dosage form of diclofenac with neurotropic vitamins B1, B6 and B12, widely used in the treatment of back pain. This combination not only enhances the analgesic and anti-inflammatory effect of diclofenac, but also opens up the possibility of reducing its doses, and therefore reducing side effects, which are mostly dose-dependent.