Cognitive processes
There are three types of cognitive impairment after a stroke:
- Damage to one of the cognitive functions: memory (amnesia), the ability to perform any actions (apraxia), impairment of visual, auditory, tactile perception (agnosia).
- Violation of several functions that generally do not affect social adaptation.
- Multiple injuries that lead to social maladaptation: impaired attention, memory, volitional processes. In this case, post-stroke dementia is diagnosed. In older people with dementia, household activity decreases and self-care skills are lost. This category of patients is at risk of recurrent stroke.
The first and second variants of the disorder can be corrected due to the plasticity of the brain: damaged functions are compensated by functions that remain intact.
Rehabilitation of older people with post-stroke dementia includes sessions with psychologists. With the help of special exercises, patients develop auditory and visual memory, the ability to concentrate, and solve logical problems. The recovery process is accompanied by drug therapy.
Rehabilitation after a stroke at home
After overcoming the acute period in the hospital, a rehabilitation period begins for a pensioner with a stroke. Relatives need to decide where it is better for an elderly person to undergo a recovery course: at home or in a rehabilitation center.
You may also be interested in the article: How to obtain patronage for an elderly person
If the family has decided to independently care for the patient after a stroke, they need to follow the recommendations of the attending physician and maintain constant contact with specialized specialists: a psychologist, a neurologist, a speech therapist.
At home, a separate place is assigned to a bedridden patient after a stroke. The bed is equipped with an anti-decubitus mattress. A small table is placed nearby, on which essential items are placed: a bottle of water, care products, a table lamp.
Specialists can come to the home 1-2 times a week, work with the patient and teach home methods of conducting developmental activities. The rest of the time, family members carry out the recommended exercises with the pensioner for 10-20 minutes several times a day. During weekly visits, specialists monitor the dynamics of changes, make additions and adjustments.
Motor abilities are restored using a complex of therapeutic exercises. Before performing the exercises, it is advisable for the patient to take a shower or bath to warm up the body. If there are contraindications to taking a bath or other difficulties, the affected areas are warmed with a heating pad. The muscles will be more flexible and there will be no pain.
Examples of gymnastic exercises:
- pulling up while lying on your back, holding the headboard of the bed;
- eye movements left and right, up and down with closed and open eyelids;
- alternately raising the right and left arms and legs;
- bending the knee and grabbing the shin with the hand;
- joint movements of healthy and motionless limbs to the right and left with a rubber ring put on them.
When carrying out therapeutic exercises, the pensioner’s condition is closely monitored. He shouldn't get tired. If such signs are observed, it means that the amount of stress does not correspond to the physical strength of the patient. We need to make an adjustment: reduce the pace and number of exercises.
Speech is restored by memorizing poetry and tongue twisters. At the initial stage, simple children's poems are chosen, which are easier for a pensioner to recite after a stroke. Gradually more complex material is selected.
Looking at family photographs can activate the process of remembering, since it is easier for the patient to recall the past in his memory. An elderly person remembers acquaintances and friends in the images, then the events associated with them. He tries to pronounce the names of the places he has visited, the objects he sees in the images.
Scientists believe that singing has a beneficial effect on people who have suffered a stroke. If they hear singing, sing together with loved ones, speech activity will be restored faster.
For rehabilitation to be successful, an elderly person should not be in a social “vacuum”: you constantly need to communicate with him, talk, ask questions, even if at first he cannot answer them. In this way, the patient’s desire to speak is stimulated, he remembers words and their meaning.
Chess, checkers, and dominoes are used to develop thinking abilities. In a family, even a small child can take part in restoring the health of a grandfather or grandmother by putting together puzzles, mosaics, or playing a board game.
A separate issue is the organization of nutrition for an elderly person after a stroke.
Excluded from use:
- alcoholic drinks;
- fatty and spicy foods;
- coffee, strong tea;
- sweets.
It is advisable to add to the diet:
- drink liquid of at least 1.5 liters. per day;
- increase consumption of fruits and vegetables;
- eat whole grains;
- replace sweets with dried fruits.
Food should consist of useful substances and be easily digestible so that the body is not overloaded.
It is useful to cook boiled vegetables, dishes from lean fish and meat, and porridge with low-fat milk. If there are paresis and problems with swallowing, the patient is fed through a tube with ready-made nutritional mixtures. As soon as the opportunity arises, you need to take the patient for a walk. Staying in the fresh air is good for brain activity, the body receives oxygen and vitamin D, and appetite appears.
You may also be interested in the article: How to choose a private facility for the elderly
The moral atmosphere in the house is of great importance. Patients who receive family support recover faster. If they experience hostility from others or rudeness, the healing process is slowed down. There is no need to criticize and laugh at clumsiness and awkwardness. Only with encouragement will an elderly person develop a strong desire to overcome the disease.
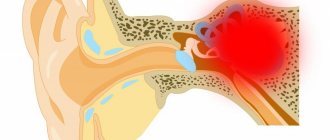
Early complications of stroke
The most serious consequences are caused by a stroke on the left side of the brain, since in most people it is more developed. Depending on the affected hemisphere, the opposite side of the body suffers - with a stroke on the right side of the brain, the consequences affect the left side of the body, and vice versa.
Most often, an attack occurs in the first half of the day or before waking up.
At an early stage, headaches, numbness of the face and limbs, and speech disorders may be noted. Vision deteriorates, an arm or leg or both limbs do not work. The consequences for the patient at first are as follows:
Advertising:
| Sign | Meaning |
| High blood pressure | The body's attempt to restore blood circulation can lead to brain swelling and recurrent stroke. |
| Temperature rise | Bad symptom, increases risk of death by 1/3 |
| Inhibition of reactions | Damage to the corresponding brain centers on the right or left side |
| Convulsions | More typical for hemorrhagic stroke |
| Rapid paralysis | The larger the affected area, the higher the risk of loss of motor functions |
Already in the first hours after the attack, a person often becomes deaf, loses vision, and an arm or leg becomes paralyzed. Memory is lost completely or partially. Speech impairments are more typical for left-sided lesions. If a large part of the brain is attacked, coma occurs. The best prognosis for emerging from a coma is for people with preserved reflexes, including swallowing, who remain in this state for no more than an hour. Also, at an early stage, a serious consequence is cerebral edema - swelling of its glial tissue due to soaking in fluid.
Recovery in a boarding house
Rehabilitation of an elderly person after a stroke at home requires the full-time employment of one of the relatives for the next six months. While the patient is bedridden, he cannot be left at home alone for two reasons: he is helpless and it is necessary to deal with him several times a day. The volume of care is so large and multidirectional that soon the caregiver himself will need support and replacement.
In boarding houses for the elderly, professionals are involved in the rehabilitation of patients. Special equipment is used for treatment. An individual program is developed for each patient. Restoration methods that have been developed over the years produce positive results within a month.
Late consequences of the disease
The timeliness of assistance plays a big role in the quality of subsequent rehabilitation, but adverse consequences are observed after almost every case of the disease. Only 10% of people recover completely; the rest experience varying degrees of disability.
Hemorrhagic stroke always has the most serious complications.
Brain hemorrhage in the future threatens complete or partial paralysis and severe mental disorders. A person may lose vision, speech becomes slow, there are difficulties with pronunciation, perception, and adequate assessment of the situation. Many people lose their memory, become depressed or become aggressive. A person's mental abilities decline. Often occur:
Advertising:
- epileptic seizures;
- pain in different areas of the body;
- mood changes;
- uncontrolled excretion of urine and feces.
An ischemic stroke causes the death of neurons in the right or left side of the brain. This provokes weakness of the legs and arms, unsteadiness of gait or paralysis, deterioration of motor skills and movements of the facial muscles. Patients forget the past, have poor orientation in time and space, and cannot clearly pronounce words. In severe cases, reflexes are disrupted - for example, the act of swallowing, and a person can choke even on water.
Rehabilitation therapy
After stabilization of the pathological condition and improvement, the patient is prescribed restorative drug treatment, a course of massage and physical therapy, physiotherapeutic procedures, dietary nutrition and adherence to a daily routine. To regain speech, regular classes with a speech therapist-defectologist are necessary.
They use drugs to normalize the functions of the nervous system - Cerebrolysin, Glycine, Piracetam and a complex of vitamins and minerals. If depression and sleep disorders occur, antidepressants are indicated.
Repeated stroke
One of the most serious consequences is the tendency to have another stroke. The second and subsequent attacks determine the prognosis, because it is even more difficult to recover from them. How long the life expectancy will be depends on the effectiveness of preventing a second attack within a month of the first. The statistics are as follows:
- in the first year the pathology recurs in 5-20%;
- in the first three years, recurrent stroke occurs in 40%.
Advertising:
Relapse is more often observed in old age, with untimely hospitalization, poor care, and stress. The disease also recurs in people with serious chronic diseases - diabetes, hypertension and others. In the long-term stage, the attack may occur again if the patient continues to smoke, forgets to take medications for thrombosis, to lower cholesterol and blood pressure.
Stages of treatment
If signs of a stroke are detected during or after binge drinking, first aid is as follows:
- call an emergency ambulance;
- avoid further drinking of alcohol;
- calm the victim and limit his movements by placing him in bed until the doctors arrive.
To preserve the integrity of the clinical picture, it is prohibited to give any medications, force someone to drink water, or bring a person to his senses by braking or patting the cheeks. The condition of an acute stroke poses a threat to a person’s life and requires immediate medical, sometimes resuscitation, care.
Content:
- Symptoms of alcoholic stroke
- Causes
- Stages of treatment
- Staying in hospital
- Rehabilitation therapy
- Forecasts
Alcoholism causes multiple diseases of internal organs. One of the frequently observed pathologies is impaired cerebral circulation against the background of high blood pressure caused by prolonged alcohol abuse. Alcoholic hemorrhagic stroke occurs after heavy drinking or during a period of alcoholic excess. From the moment the first signs appear, the patient’s condition may improve for some time, but without timely treatment, a sharp deterioration soon follows. Therefore, it is extremely important to recognize the disease in time and literally immediately seek medical help.
What are the features of a left hemisphere stroke?
As we said above, the left hemisphere of the brain controls the right half of the human body. If the left hemisphere of the brain is damaged, paresis (paralysis) of the right limbs will be noted.
The left hemisphere also controls speech (for all right-handers and half of left-handers, and for the other half of left-handers, the center of speech is located in the right hemisphere of the brain), memory and cognitive functions, so during a stroke the patient may have problems with speech, he will lose memory, and mood swings, behavior will change - he will become slow and cautious.
How does the disease manifest? Symptoms of a stroke
Signs of a stroke usually appear suddenly. It can be:
- sudden loss of consciousness;
- numbness and paralysis of a part of the body;
- partial loss of vision;
- double vision;
- difficulty speaking or impaired understanding;
- loss of coordination, balance, dizziness.
Symptoms of a hemorrhagic stroke often include headache and vomiting.
The first signs and symptoms of a stroke may appear against the background of increased blood pressure. In some patients, the development of the disease is preceded by transient ischemic attacks - a temporary disturbance of blood circulation and brain function. Therefore, it is important to notice the first signs of a stroke, such as weakness in one of the limbs, impaired facial expressions, short-term difficulty speaking, and temporary blindness in one eye. Timely medical care can prevent the development of a stroke.
Types by development mechanism
The first type is ischemic
. Of the total number, it accounts for 70–85% of cases. Caused by obstruction of blood flow to one part of the brain. The most common cause is a blood clot.
The second type is hemorrhagic
. It accounts for 20–25% of cases. It is caused by rupture of the walls of blood vessels, which causes intracerebral hemorrhage.
The third type is subarachnoid
. Under the influence of non-traumatic impact, a vessel passing along the surface of the brain ruptures. Because of this, hemorrhage begins in the cavity located between the pia mater and the arachnoid membrane. This species accounts for approximately 5%.
The fourth type is spinal
. Occurs in less than 1% of total cases. When it occurs, blood circulation through the spinal arteries is stopped or disrupted. Divided into ischemic and hemorrhagic.
Staying in hospital
A mandatory condition for treating stroke after heavy drinking is complete abstinence from any alcoholic beverages.
Treatment includes emergency prehospital care and inpatient therapy until vital signs, neurological status and hemodynamics are stabilized. Next, a period of rehabilitation is required.
The following groups of drugs are used in the hospital:
- antihypertensive drugs to normalize blood pressure;
- anticoagulants to reduce blood clotting, reduce the risk of formation and dissolution of existing clots;
- medications to normalize neurological status and vascular drugs to improve blood circulation and nutrition of the brain;
- antioxidants to relieve post-ischemic oxidative stress.
Treatment of alcoholic stroke is long-term, the prognosis is individual in each specific case.
General cerebral symptoms
This group of symptoms includes: disturbances in the level of consciousness, headache, nausea, vomiting, dizziness, convulsions. General cerebral symptoms are characteristic signs of increased intracranial pressure with subarachnoid or intracerebral hemorrhage, extensive cerebral infarction.
Criteria for clear consciousness:
the patient is awake, correctly assesses the environment, is oriented in time, place, situation and his own personality.
There are quantitative (unproductive) and qualitative (productive) forms of disturbance of the level of consciousness.
Quantitative (“depression of consciousness”) forms include: stunning
(superficial and deep),
stupor, coma
(first, second and third degree). Currently, it is generally accepted to use assessments of the degree of depression of consciousness - the Glasgow scale.
Stunning (moderate, deep) - characterized by impaired attention, loss of coherence of thoughts or actions. When stunned, the patient is awake, but he is lethargic, drowsy, quickly becomes exhausted and falls asleep.
Stupor - the patient opens his eyes only after exposure to a strong stimulus (loud sound, pain, strong smell, etc.) The reaction to verbal instructions is weak or absent, there is no speech production. At the same time, targeted and local defensive reactions remain intact.
Coma is a complete loss of consciousness; we cannot awaken the patient. Superficial coma (first degree) - it is impossible to wake the patient, he reacts to painful stimuli with simple, erratic movements, there is no opening of the eyes to any irritation. Vital functions are not depressed.
Deep coma (second degree) - the patient does not respond with motor reactions to painful stimuli. Most reflexes are suppressed, but breathing and hemodynamics are still not there.
Atonic coma (third degree) is the complete absence of the patient’s response even to very strong painful stimulation. Muscle atony, areflexia, impaired or absent breathing, depression of cardiac activity may be observed.
Qualitative changes in consciousness consist in the fact that the patient is awake, but productive contact with him is difficult or impossible due to severe psychotic disorders. Examples of such conditions are dementia, delirium, twilight state of consciousness and a number of others. Psychomotor agitation is often observed.
Headache is most typical for hemorrhagic forms of stroke. For example, with subarachnoid hemorrhage, the headache is very intense, unusual in nature, appears like a “blow” to the head, and there may be a feeling of heat, pulsation, or a hot wave inside the head.
Convulsive seizures (tonic, tonic-clonic, clonic-tonic, generalized or local) are often observed at the onset of a stroke (primarily hemorrhagic).
Dizziness, nausea, and vomiting are not symptoms specific to acute stroke, but are often the leading reason for seeking medical help at “03” services or a clinic. In addition, like other general cerebral symptoms, they indicate the need for emergency symptomatic therapy.
Main risk factors for stroke
| Uncorrectable risk factors | Adjustable risk factors |
| Age | Hypertension |
| History of stroke or stroke | Diabetes |
| Stroke or myocardial infarction from blood relatives | Atrial fibrillation |
| Migraine | Smoking |
| Gender (men are larger than women) | Hypercholesterolemia |
| Ethnicity | Thrombosis factors |
| Constriction of carotid or vertebral Arteries | Excessive alcohol consumption |
| Psycho-emotional overload. | Excessive salt intake |
Focal symptoms
1. Unilateral (right or left) motor disorders in the limbs in the form of paresis (decreased muscle strength) or paralysis (complete lack of movement in the limb) are the most common symptoms of stroke. Test. You can identify paresis in the following way: ask the patient to hold his arms outstretched forward for a few seconds; the affected arm will drop faster. In case of complete paralysis, the patient will not be able to hold his hand in front of him at all.
2. Speech disorders (dysarthria, aphasia). In the case of aphasia, both the understanding of addressed speech (the patient will not comply with requests and commands) and his own speech production may be impaired - the patient cannot construct his own speech. Dysarthria is manifested by unclear, “blurred” speech, there is a feeling of “porridge in the mouth”, the patient’s perception of the addressed speech does not suffer. Test. To identify the presence of speech disorders, ask the patient to say his name or say a simple phrase.
3. Facial asymmetry (smoothness of the nasolabial fold). Test. It is necessary to ask the patient to smile or show teeth and gums.
4. Unilateral (in the arm and/or leg) sensitivity disorders (hypoesthesia) – there is a feeling as if the patient was “lying down” on his limb; he may not feel touching it. Test. To identify sensory disorders, it is necessary to apply injections to symmetrical areas of the limbs on the right and left. If there are sensory disorders, the patient will not feel the injections on one side or feel them significantly weakened.
5. Oculomotor disorders. Paresis of gaze to the side may occur (restriction of movements of the eyeballs), up to a forced tonic rotation of the eyeballs. An ominous symptom is anisocoria (different pupil sizes), which usually occurs due to dislocation of the brain (in this case, due to superior - temporotentorial - herniation). Test. To check gaze paresis, it is necessary to ask the patient to follow an object moving horizontally and illuminate the pupils with a flashlight to compare their sizes and photoreaction.
6. With a stroke, there may be other focal symptoms - hemianopsia (loss of half the visual fields), dysphagia (swallowing disorders) and others.