Frontotemporal dementia is a neurodegenerative disease accompanied by progressive behavioral and personality disorders. Over time, especially without properly selected treatment, a person completely loses the ability to have full productive contact with others (total dementia). The pathology develops against the background of degenerative changes in the frontal and anterior temporal lobes of the brain. To date, there are no treatment protocols or medications that can be used to cure a person suffering from frontotemporal dementia (FTD), however, doctors at the Leto Mental Health Center will individually select drug therapy that can slow down the progression of severe symptoms.
Classification
In accordance with modern standards of psychotherapy, several forms of frontal dementia are distinguished:
- behavioral with a predominance of personality disorders (occurs most often);
- agrammatic (semantic);
- logopenic (however, according to some experts, this option is rather one of the atypical varieties of Alzheimer's disease).
Atrophy may affect the temporal, frontal, or frontotemporal regions of the brain. The location of the focus is another criterion for determining the form of the disease.
Clinical picture
The disease begins between 45 and 70 years , there are no cases of frontotemporal dementia in adolescents (if similar symptoms are present in younger people, a more thorough diagnosis is required, since either hereditary mental illnesses or disorders due to organic brain damage are likely). Symptoms develop gradually.
In the early stages, personality changes predominate, the severity of which depends on the exact localization of the neurodegenerative process. With dementia of the frontal type, the following gradually develop:
- inactivity;
- lethargy;
- absence of external emotional manifestations;
- indifference to everything that happens around;
- reduction and simplification of mental activity,
- slowing, distortion of speech (up to loss of the ability to speak),
- lack of movement, recumbent lifestyle.
When the pathological process is localized in the orbital cortex, the following prevail in the clinical picture:
- loss of sense of tact and distance;
- loss of moral attitudes and principles;
- impulsiveness of actions;
- gross impairments of the cognitive spectrum (the ability to abstract thinking, planning, and performing multi-stage actions is lost), but at the same time memory and orientation in space and the environment are preserved.
Atrophy of the temporal lobes is accompanied by stereotypies - meaningless, illogical repetitions of phrases or individual words, movements, for example, stomping, clapping, rubbing the skin, scratching, pursing lips, smacking, etc. Sometimes obsessive counting appears: the patient constantly counts the number of steps, steps, etc. passed.
In addition, there is a clearly pathological tendency towards cleanliness, which sometimes takes the form of a phobia. Another form of stereotypy is the strictest adherence to an established daily routine, the change of which causes real panic in a person.
In addition, FTD is accompanied by:
- asthenic symptoms (weakness, fatigue, headaches, insomnia);
- movement disorders, muscle rigidity;
- formation of delusional ideas;
- speech disorders (and in 60% of patients they are noted at the initial stage of pathology).
One of the key symptoms is the early loss of the ability to understand and empathize with others' emotions. A person ceases to be interested in the feelings and experiences of those around him (including close people), he is indifferent to the grief of others, which is why the patient usually ends up in social isolation.
Changes in eating behavior are also characteristic. Frontotemporal dementia is typically characterized by an addiction to sweets, or to foods of a strictly specific color, shape, or with a specific smell.
The feeling of satiety is lost. In later stages of FTD, the patient may strive to taste any objects, including those that are clearly inedible.
Is it possible to cure
The prognosis for frontal lobe dementia depends on the rate of development of degenerative changes. In the early stages of the disease, patients do not have serious disorders and disorders, so complex therapy is effective in their treatment.
With complete degradation of personality, problems appear with orientation in space, expression of thoughts, and self-care, so the patient needs the help of experienced neurologists and loved ones. In the later stages, the muscles atrophy, so the patient is forced to lead a sedentary, recumbent lifestyle. Late-stage frontal lobe dementia can cause secondary diseases.
The lifespan of patients with severe dementia can reach 15 years with adequate therapy. If symptoms of the disease are detected, it is important to consult a neurologist. Specialists at the Yusupov Hospital select modern therapy methods for patients that allow them to maintain the intellectual and physical activity of patients and improve their quality of life.
Diagnostics
Some symptoms of frontotemporal dementia (delusions, sexual disinhibition, etc.) are typical for other mental illnesses, in particular schizophrenia and Alzheimer's disease. Therefore, doctors at the Leto clinic adhere to the principles of step-by-step diagnosis, excluding all possible diagnoses.
The examination includes the following stages:
- Collection of family history (if necessary, we study outpatient records of the patient’s relatives who have been identified with mental disorders);
- Careful study of the clinical picture. The doctor asks loved ones in great detail about how the disease began, what signs appeared in the first place, how exactly the patient behaves, and how mental and behavioral disorders manifest themselves.
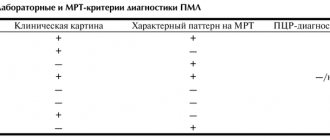
- Instrumental research. A brain tomography is required. CT, MRI and PET-CT (considered the most informative) clearly show signs of selective atrophy.
Causes
Frontotemporal dementia is a gradually developing, steadily progressing degenerative pathological process in brain tissue, leading to degradation with the collapse of speech, mainly spoken aloud. The average age of patients is 53–60 years, but the disease can begin earlier or later; men get sick more often than women.
It is believed that the disease is based on a hereditary mutation of genes in the region of chromosome 17. In some cases, chromosomes 9, 14 and 3 were found to be involved. There have been numerous cases of familial cases of morbidity. Families are known in which other forms of hereditary degenerative diseases were observed.
Important. External influences (injuries, illnesses) have a provoking role and aggravate the course of frontotemporal dementia, this is especially true for children and adolescents. If a child is developmentally delayed, cannot cope with the school curriculum, or has behavioral characteristics, it is worth contacting a child neurologist or psychiatrist.
Temporofrontal dementia is not uncommon in adolescents and children. The cause of the disease is burdened heredity, and trigger factors are traumatic brain injuries, neuroinfections, etc.
Cost of services
| CONSULTATIONS OF SPECIALISTS | |
| Initial consultation with a psychiatrist (60 min.) | 6,000 rub. |
| Repeated consultation | 5,000 rub. |
| Consultation with a psychiatrist-narcologist (60 min.) | 5,000 rub. |
| Consultation with a psychologist | 3,500 rub. |
| Consultation with Gromova E.V. (50 minutes) | 12,000 rub. |
| PSYCHOTHERAPY | |
| Psychotherapy (session) | 7,000 rub. |
| Psychotherapy (5 sessions) | 30,000 rub. |
| Psychotherapy (10 sessions) | 60,000 rub. |
| Group psychotherapy (3-7 people) | 3,500 rub. |
| Psychotherapy session with E.V. Gromova (50 minutes) | 12,000 rub. |
| TREATMENT IN A HOSPITAL | |
| Ward for 4 persons | 10,000 rub./day |
| Ward for 3 persons | 13,000 rub./day |
| Ward 1 bed VIP | 23,000 rub./day |
| Individual post | 5,000 rub. |
| PETE | 15,000 rub./day |
This list does not contain all prices for services provided by our clinic. The full price list can be found on the “Prices” , or by calling: 8(969)060-93-93. Initial consultation is FREE!
Treatment of frontotemporal dementia in honey
Therapy mainly comes down to the prescription of general strengthening drugs. These are multivitamin complexes, nootropics, means for normalizing metabolism, cardio- and neuroprotectors. However, the medications listed can only support the functioning of internal organs and systems, and, by and large, do not affect the symptoms of FTD.
The peculiarities of the clinical picture of the disease and the risk of rapid development of total dementia forces doctors to use all the medicinal resources of modern psychiatry and neurology. Thus, according to research, in frontotemporal dementia, drugs used to treat Alzheimer's disease (cholinesterase inhibitors and NDMA antagonists) have a good result.
To correct behavioral disorders the following is prescribed:
- antidepressants (preference is given to drugs from the group of selective serotonin reuptake inhibitors): indicated for anxiety, depression, obsessive disorders;
- neuroliptics and valproates: used for aggressiveness, psychomotor agitation.
Since patients quickly lose the ability to self-care and perform basic daily duties, we offer treatment in a hospital, where patients are provided with round-the-clock care and supervision by qualified medical personnel.
To make an appointment and additional consultation, call us by phone 8(969)060-93-93.
Introduction
The term frontotemporal dementia (FTD) is currently used as an umbrella name for a group of neurodegenerative diseases consisting of three main clinical types: behavioral variant FTD (B-FTD) and primary progressive aphasia (PPA), which includes two aphasics. variants of FTD: semantic (S-PPA) (semantic dementia) and PPA with decreased speech fluency (agrammatic variant of PPA - A-PPA).
Clinical manifestations characteristic of FTD are often present in three other neurodegenerative diseases with severe movement disorders: corticobasal degeneration (CBD), progressive supranuclear palsy (PSP), and amyotrophic lateral sclerosis (ALS) [1]. Despite the wide range of clinical manifestations, the above diseases are usually referred to under the umbrella term frontotemporal lobar degeneration (FTLD) because their clinical types often share common neuromorphological substrates.
The clinical picture of FTD is defined by progressive behavioral disturbances, executive function disorders, and severe speech deficits. FTD is a common type of dementia, especially in presenile patients. The onset of the first symptoms of the disease usually occurs before age 60, and the average survival time from diagnosis varies from 3 to 10 years. The prevalence of FTD is 15 per 100,000 population aged 45 to 65 years, which is similar to the prevalence of Alzheimer's disease (AD) in this age group [2]. FTD can mimic various mental disorders (for example, major depressive disorder, bipolar affective disorder, schizophrenia, obsessive-compulsive disorder, borderline personality disorder, etc.) due to the presence of severe behavioral disturbances and an early age of onset, which often leads to incorrect diagnosis and , as a consequence, incorrect therapeutic tactics.
The underlying neuromorphological features of FTD determine the clinical phenotype, which is characterized by selective neurodegeneration of the frontal and temporal cortex. Depending on the primary localization of atrophy, clinical manifestations are dominated by either behavioral or speech disorders. Genetic predisposition is an important risk factor for FTD. A common feature of FTD is the accumulation of certain neuronal proteins. Of these, the most important are τ-protein associated with microtubules (Microtubule-associated protein tau - MART), transactive DNA-binding protein (Transactiveresponse DNA-binding protein 43 kDa - TDP-43), RNA-binding protein (Tumor associated protein fused in sarcoma -FUS). A family history of dementia is noted in 40% of cases of FTD, although a clear autosomal dominant pattern of inheritance is found in only 10% of cases [3]. It has been shown that mutations in the C 9 orf 72
,
MAPT
and
GRN
account for approximately 60% of all cases of hereditary FTD [4]. Conducting a genetic study is considered necessary in the presence of a hereditary burden in patients with dementia, primarily in autosomal dominant neurological diseases such as FTD, AD, parkinsonism, ALS, myopathies and psychoses of late age [4, 5].
Recent advances in clinical practice, neuroimaging studies and molecular genetic discoveries, having significantly increased the accuracy of FTD diagnosis, make it possible to differentiate clinical variants of the disease and distinguish them from other mental disorders. As our understanding of the molecular genetic basis of FTD improves, new rational treatments are emerging [6].
This review examines currently available treatments for FTD, discusses recent advances in FTD that have led to improvements and developments in therapeutic modalities, and examines the results of recently completed and ongoing clinical trials. The feasibility of using non-pharmacological methods of FTD is considered.
Therapeutic aspects of studying FTD
Pharmacological strategies
There have been significantly fewer studies aimed at finding therapeutic agents for the treatment of FTD than for BA. According to the Internet resource www.clinicaltrials.gov, provided by the American National Library of Medicine, an assessment of 293,985 clinical trials (data as of January 2021) conducted in 207 countries and 50 US states revealed that they have been or are being conducted there are currently 150 pharmacological and non-pharmacological trials in FTD, while in AD there are 2021.
To date, the US Food and Drug Administration (FDA) has not approved any drug indicated for use in FTD [7]. Currently, only a few pharmacological approaches are offered (not formally validated or recommended for the treatment of FTD), in particular the symptomatic use of antidepressants, antipsychotics, cholinesterase inhibitors and memantine.
A systematic search of 4 major databases (PubMed, Medline, Psych INFO and Cochrane) showed that in recent years there have been only 9 randomized, controlled, double-blind clinical trials examining the effectiveness of different drugs in the treatment of patients with FTD. Among them, 2 studies were aimed at studying the effectiveness of paroxetine, an antidepressant from the group of selective serotonin reuptake inhibitors (SSRIs); 1 - antidepressant trazodone, 2 - stimulants: methylphenidate and dextroamphetamine. Only 1 study examined the use of the acetylcholinesterase (AChE) inhibitor galantamine. In 2 studies, the effectiveness of the antagonist N-methyl-D-aspartate memantine was revealed. An attempt has also been made to administer the neuropeptide drug oxytocin to patients with FTD. Analysis of the results showed that SSRIs, trazodone and amphetamines may be effective in reducing the severity of some behavioral symptoms, but none of these drugs affects the cognitive functioning of patients [8].
S. Lopez-Pousa et al. [9] conducted an observational study that included 1092 patients with asthma and 64 patients with FTD. Analysis of the therapy showed that 43.8% of patients with FTD were treated with antidementia drugs, 31.3% with antipsychotics, 1.6% with antiparkinsonian drugs, and 53.1% of patients took antidepressants. The researchers concluded that there is a discrepancy between clinical practice and therapeutic recommendations based on clinical evidence. However, according to the authors, this does not mean that these types of therapy are ineffective. It has been confirmed [10–14] that the use of antidepressants and antipsychotics mainly improves behavioral symptoms of FTD, such as irritability, agitation, symptoms of depression and eating disorders.
AChE
inhibitors AChE inhibitors, which have been successfully used in the treatment of AD, have been widely studied for the treatment of cognitive impairment in patients with FTD, but all of them turned out to be ineffective. In particular, the drug donepezil, which was taken by 24 patients with FTD in a 6-month open-label study [15], caused a worsening of FTD symptoms, and in 4 patients, an increase in behavioral symptoms. Discontinuation of the drug resulted in a decrease in behavioral disorders.
The effectiveness of rivastigmine was studied in a 12-month open-label study in patients with FTD. The study results showed that the drug contributed to a small improvement in the severity of behavioral problems, as assessed by the neuropsychiatric questionnaire NPI, and, in particular, a decrease in the burden on caregivers. However, the use of rivastigmine did not prevent the increase in cognitive impairment [16].
Treatment with the third most commonly used AChE inhibitor, galantamine, was used in 36 patients with P-FTD and PPA in an 8-week placebo-controlled followed by an 18-week open-label study [17]. According to the results of the study, in patients with PPA, speech functions remained stable during treatment, which was regarded as a trend toward effectiveness. However, the authors suggested that perhaps these patients had a speech therapy form of PPA that is very similar to BA. The therapeutic effect on behavioral disorders when taking galantamine has not been established.
According to some authors [16–18], the use of AChE inhibitors in patients with FTD can increase behavioral disorders and impaired motor functions, which is why the use of drugs in this group in FTD is not recommended.
Given previous evidence of the positive therapeutic effects of the drug memantine, which has a therapeutic indication for the treatment of moderate to severe AD, in relation to cognitive abilities and overall functioning, several studies have been conducted to determine the therapeutic effectiveness of memantine in patients with FTD.
In an open study by M. Swanberg [19], some patients with FTD who received memantine showed an improvement in the overall assessment of non-cognitive disorders (according to the NPI questionnaire), mainly due to a decrease in apathy, agitation and anxiety. In the same observation, memantine therapy was well tolerated in patients with FTD. However, the results of a multicenter, randomized, double-blind, placebo-controlled study [20], in which patients with FTD took memantine at a daily dose of 20 mg or placebo for 26 weeks, did not confirm the effectiveness of the drug in FTD. However, improvements were shown in a number of indicators on the NPI questionnaire and on the CGI-C Clinical Global Impression scale, which did not reach the level of statistical significance [20].
An open-label pilot study [21] of the therapeutic effects of memantine in 17 patients with FTD assessed the metabolic activity of the frontal and temporal lobes of the brain using positron emission tomography (PET) with 18F-FDG (18F-fluorodeoxyglucose), as well as behavioral disorders using special scales. After 6 months of memantine therapy, an increase in metabolic activity was found in the left orbitofrontal cortex in 5 patients with S-PPA. In addition, a delayed increase in metabolism of the left and right insula and left anterior cingulate cortex was noted. In the right anterior cingulate gyrus, metabolic activity increased at the beginning of therapy, and its indicators continued to improve further by the 6th month of therapy. However, behavioral disturbance scores assessed by the FBI Frontal Behavioral Symptom Questionnaire worsened by 43.3%. The increase in cortical metabolic activity in patients with S-PPA persisted for 6 months. The authors concluded that an appropriate double-blind, placebo-controlled study was necessary.
A meta-analysis of scientific publications [22] on the use of memantine in patients with FTD in two placebo-controlled studies showed that the performance of 130 patients with FTD treated with the drug, when assessed on a number of tests and scales, such as the Mini-Mental State Examination MMSE, The NPI, the Zarit ZBI Burden Inventory, improved compared with patients receiving placebo, but the differences did not reach statistical significance. The authors believe that memantine may be useful in the treatment of patients with FTD, but emphasize that there are limitations in extrapolating the results obtained in the treatment of patients with AD to the treatment of patients with FTD and recognize the need for further randomized, double-blind, placebo-controlled studies involving a larger number of patients .
Among antidepressants, SSRIs have been mainly used to treat FTD. In 2004, M. Ikeda et al. [23] reported the results of a 12-week open-label study in which 60 patients with P-FTD and S-PPA were treated with fluvoxamine. Changes in behavioral and other psychopathological symptoms were assessed using the NPI questionnaire [24]. According to the data obtained, fluvoxamine significantly reduced behavioral symptoms in patients with FTD, especially behavioral stereotypies, but assessments of cognitive function on the MMSE scale [25] did not change.
The serotonin reuptake antagonist drug trazodone, a thiazolopyridine derivative, was used in a randomized, double-blind, placebo-controlled crossover study [26] in 31 patients with behavioral symptoms of FTD assessed by the NPI questionnaire. During treatment with trazodone, behavioral disorders, especially eating disorders, as well as agitation, irritability, symptoms of depression and dysphoria decreased significantly. In the period after discontinuation of the drug, a stable improvement (from mild to moderate) in the clinical manifestations of the disease was noted, however, assessments of cognitive function on the MMSE scale did not change.
Two clinical trials [27, 28] assessed the effectiveness of paroxetine, a selective inhibitor of 5-hydroxytryptamine (5-HT) and serotonin reuptake by serotonergic neurons, in patients with FTD. The first study [27], which included 16 patients with FTD, was an open-label, randomized, non-controlled, non-crossover study. Group 1 included 8 patients who were prescribed paroxetine 20 mg/day, 8 patients of group 2 received piracetam 1200 mg/day. After 14 months of therapy, patients in group 1 (paroxetine) showed a significant decrease in the manifestations of behavioral disorders. In addition, a reduction in stress among caregivers was noted. Another randomized, double-blind, placebo-controlled crossover study [28] involved 10 patients with FTD who received paroxetine for 12 weeks with a gradual increase (by 10 mg per week) to 40 mg/day. The authors did not find a significant improvement in the patients’ condition on behavioral scales; only some psychological indicators (for example, in the training model of pattern recognition) showed positive dynamics. Undesirable side effects were observed when taking paroxetine at a dose of 40 mg/day, in which the patient's condition looked like tryptophan depletion. The discrepancies in the results of these two clinical studies are most likely due to different procedures and study designs, as well as differences in the dosage of the drug used. The dose of paroxetine 40 mg/day was considered too high for patients with FTD. The optimal dose of the drug, maintaining a balance between the therapeutic effect and the absence of side effects, was 20 mg/day.
In the group of antipsychotic drugs, atypical neuroleptics have attracted the most attention from researchers. According to some authors [12, 29], antipsychotics, such as aripiprazole and olanzapine, can improve the clinical condition of patients with FTD by influencing behavioral disorders and irritability. The administration of quetiapine in a number of cases showed a decrease in agitation in patients with P-FTD [30], however, in a double-blind crossover study [31], no positive changes were noted in 8 patients (according to the NPI questionnaire). It is emphasized that these drugs can also cause side effects such as drowsiness, weight gain, and symptoms of parkinsonism. In addition, they increase the likelihood of extrapyramidal side effects, which limits their therapeutic use.
There is extremely inconclusive information about the advisability of using antiepileptic drugs with normothimic effects, such as valproic acid derivatives, topiramate, carbamazepine, in patients with FTD to relieve behavioral and affective disorders, especially since reports of their therapeutic effects are limited to isolated cases [30, 32].
In the work of S. Jesso et al. [33] used the neuropeptide drug oxytocin at a dose of 24 IU in 20 patients with P-FTD in a double-blind, placebo-controlled, randomized study with a crossover design.
The purpose of the study was to evaluate the effect of a single dose of intranasal oxytocin on behavioral and emotional disorders. 8 hours and 1 week after drug administration, patients receiving oxytocin were examined using the NPI questionnaire. There was a significant improvement in NPI scores compared to both the placebo group and baseline scores. Oxytocin has been suggested as a potentially promising candidate for the symptomatic treatment of patients with P-FTD. The need for further study of this neuropeptide in the treatment of FTD is substantiated.
One of the latest clinical studies conducted in patients with FTD [34] concerned the determination of the safety and tolerability of 3 dosages of intranasal oxytocin (24, 48, 72 IU) in parallel groups of patients (23 patients with P-FTD, 3 with S-PPA). using a regimen of increasing the dose of the drug administered 2 times a day for 1 week. The study results showed that oxytocin in 3 doses was safe and well tolerated by patients. However, the authors believe that a longer multicenter study is required to determine the therapeutic effectiveness of long-term administration of intranasal oxytocin in FTD [34].
The aim of 8 clinical trials was to examine the effect of psychostimulants on symptoms of apathy in dementia. Methylphenidate and dextroamphetamine were prescribed to patients with FTD. The potential benefit of treating apathetic disorders with psychostimulants was noted, but the need for a thorough assessment of the physical condition of each patient was emphasized due to the possibility of developing adverse somatic reactions in the form of increased blood pressure and the development of tachycardia. No less importance was attached to the risk of irritability, agitation and psychosis [35].
Recent scientific advances in understanding the pathobiological processes of FTD have identified several new potential therapeutic targets and targets for the development and creation of new effective disease-modifying drugs. Thus, the discovery of the fact that pathological τ-protein spreads transsynaptically in a prion-like manner to other regions of the brain along cortical associative pathways has caused increased interest in the possibility of using antibodies to prevent transneuronal spread of pathological proteins. The authors of this idea hope in the future to find a way to prevent the disease in this way [36–38]. Other possible therapeutic approaches associated with tauopathies are based on testing the effectiveness of τ-aggregation inhibitors with methylene blue derivatives and microtubular stabilizers as drugs (for example, TPI 287), as well as the development of τ-vaccines using monoclonal τ- antibodies (MTA). [39].
Because neurodegeneration in progranulin mutation carriers is associated with progranulin haploinsufficiency and decreased serum progranulin concentrations, modern researchers are attempting to inhibit the development of neurodegeneration in progranulin mutation carriers using molecules such as the histone deacetylase inhibitor hydroxamic acid suberoylanilide, which enhances or increases progranulin transcription. Researchers' attention has been drawn to the fact that alkalizine compounds, such as chloroquine, bepridil and amiodarone, stimulate the production of progranulin, and vacuolar ATPase inhibitors increase the intracellular and secreted concentration of progranulin [40, 41]. These discoveries provide the basis for the development of new directions of research in the field of FTD therapy.
In 2015, information appeared about a clinical trial of the effectiveness of nimodipine (NCT01835665) [42], but the results of this study have not yet been published.
New potential therapeutic targets and targets for the development and creation of new effective disease-modified drugs, clinical trials of which are currently being conducted or prepared for trials according to the Internet resource www.clinicaltrials.gov, are presented in the table.
New potential therapeutic targets and targets for the development of effective disease-modified drugs for the treatment of FTD
An analysis of studies in the field of FTD treatment allows us to state the insignificant effectiveness of certain drugs, such as memantine in relation to the manifestations of dementia and SSRIs in relation to the behavioral symptoms of the disease. However, advances in neuroscience create prospects for the development of gene technologies for the treatment of FTD and, possibly, for preventing the development of this severe form of neurodegenerative pathology in relatives.
In recent domestic publications, there have been very few works devoted to the treatment of patients with FTD. One of the latest works, published in 2021 [43], provides an analysis of the authors’ own experience in the use of SSRI antidepressants and atypical antipsychotics in patients with FTD with non-cognitive mental disorders. The author noted that an 8-week course of therapy with citalopram and quetiapine in patients with FTD reduces aggression, irritability, aberrant motor behavior and euphoria, and also improves night sleep. It is emphasized that both drugs had little effect on anxiety-depressive symptoms and apathy. In addition, during treatment with quetiapine, patients became less disinhibited; when taking citalopram, the severity of eating disorders decreased [43].
Non-pharmacological therapeutic strategies
Non-pharmacological approaches to the treatment of FTD have become increasingly important in recent years as the preferred intervention prior to pharmacological therapy, which may aggravate medical comorbidities in older patients with FTD. The main goal of non-pharmacological interventions is to prevent antisocial and addictive behavior, alleviate symptoms of the disease and reduce the suffering of people caring for such patients. Behavioral and cognitive disorders in patients with FTD often lead to severe stress for both patients' relatives and health care workers due to the fact that such patients can be dangerous to themselves and to others. Non-pharmacological strategies rely on patient involvement in environmental, behavioral and exercise interventions [44].
S. Cheng et al. [45] showed that exercise in patients with dementia improved cognitive functioning, mood and overall physical health and should be recommended to all patients who are able to perform it.
Ecological approaches to the management of patients with FTD aim to reduce irritability, aggressiveness, and anxiety from the array of daily stimuli that arise from the patient's difficulty processing information. These techniques include reducing noise levels, limiting stimulating activities, simplifying social influences by limiting interactions with small groups, and facilitating the elimination of complex daily activities that can confuse and therefore excite patients. Particular attention should be paid to the use of hearing aids and optimization of sensory stimulation to limit patient discomfort. It is believed that the use of play techniques or previous hobbies may reduce disinhibition and inappropriate behavior. M. Ikeda et al. [46] noted that the inclusion of former (pre-morbid) hobbies and previously favorite games into the lives of patients reduced antisocial behavior and disinhibition in patients with FTD.
According to a number of authors (www.theaftd.org), to ease the burden of caring for patients with FTD, it is advisable to conduct educational work among relatives of patients. Caring for patients with FTD, and especially those with behavioral problems, may require more careful monitoring to prevent alcohol abuse, excessive weight gain due to eating disorders, and possible medical complications due to the dangerous placement of inedible objects and substances in the mouth. The misjudgment and impulsiveness of patients with FTD leads to the need to restrict their access to bank accounts to prevent financial fraud or reckless purchases. Behavioral problems in patients with FTD, such as lack of empathy and interpersonal communication, can be particularly challenging for caregivers, as these symptoms can increase feelings of isolation. Social support from relatives and other caregivers is very important. The Association for FTD Patients and Their Families (www.theaftd.org), founded in 2005, offers assistance to anyone in need of information about FTD, promotes and funds research into diagnosis, treatment and care, and provides various services. types of assistance: legal, social, educational and educational. And although the association’s website is aimed at the English-speaking population, familiarization with its activities may be useful in our country.