Find out more about other diseases starting with the letter “Y”: Juvenile parkinsonism; Juvenile absence epilepsy; Juvenile myoclonic epilepsy.
Not all diseases can be completely cured. We are talking, first of all, about those that arise due to genetic conditioning. It is especially sad when it comes to childhood diseases. But medicine does not stand still, and offers treatment options that allow you to maintain an acceptable quality of life for the baby. Such a rare disease as juvenile parkinsonism, although today cannot be completely cured, is successfully corrected by medical treatment.
What does it represent?
While “classic” Parkinson’s disease can appear for a variety of reasons, childhood parkinsonism always occurs due to failures in genetics. Scientists have found that it affects not only children, but also people under 25 years of age. Most often it attacks girls and young girls. If there are several cases in one family, the spread of the disease is considered sporadic.
The disease usually manifests itself at the end of the first decade of life, or at the beginning of the second. An earlier age of development of pathology is extremely rare (less than 1% of all cases).
Juvenile parkinsonism differs from the “adult” version of the disease in that even with a long illness, the patient retains reason and intellectual abilities. There is a complete absence of dementia or mental disorders.
There are cases of increased tendon reflex or other pyramidal symptoms.
Diagnosis and treatment of Parkinson's disease
True Parkinson's disease can be diagnosed based on the patient's appearance alone. Each person has his own unique movement patterns and gait, but all parkinsonians move the same way.
Management of patients with juvenile parkinsonism allows one to do without levodopa-containing drugs for several decades, but, unfortunately, when it is prescribed, especially unreasonably early, motor fluctuations and dyskinesias develop extremely early in such patients.
Young people with irrational therapy develop drug-induced dyskinesias and severe motor fluctuations much more often. They have a better prognosis for cognitive function and life expectancy than older patients and the elderly.
Neurologists at the Yusupov Hospital apply the same criteria to confirm the diagnosis of Parkinson's disease in young people as in older age groups.
Causes
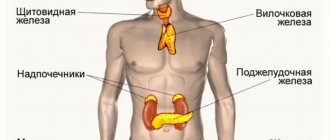
Juvenile parkinsonism is always genetically determined. There is a malfunction in the functioning of dopaminergic neurons, which should normally release dopamine. But due to a “breakdown” in the genes, this process becomes difficult or stops completely. This is the cause of external motor dysfunction. It should be taken into account that such a genetic error is inherited in an autosomal recessive manner.
It happens that both parents are healthy, but the damaged gene is present in their chain. That is, they transmit the possibility of illness to the born baby. In this case, in the future, symptoms of parkinsonism are found in no more than 25% of grown-up children. If there is a defect in the genome of only one parent, then the percentage of transmission of the disease to the offspring is practically reduced to zero.
Stages of diagnosing parkinsonism
According to the diagnostic criteria for PD (UK Parkinson's Disease Society Brain Bank, 1992), clinical diagnosis of PD is carried out in three stages:
- Stage 1. Diagnosis of parkinsonism syndrome
Hypokinesia and the presence of at least one of the following symptoms:
muscle rigidity; resting tremor 4-6 Hz; postural instability not associated with primary visual, proprioceptive, vestibular and cerebellar disorders;
- Stage 2. Criteria for excluding PD
A history of repeated strokes with stepwise progression of symptoms of parkinsonism, repeated traumatic brain injuries, significant encephalitis; treatment with drugs that can cause parkinsonism; oculogyric crises; presence of symptoms of cerebellar damage; early appearance of severe autonomic failure; long-term remission; supranuclear gaze palsy; family history of parkinsonism (more than 1 relative with a similar disease); early onset of severe dementia; Babinski's symptom; presence on MRI of signs of a cerebral tumor or open (communicating) hydrocephalus; lack of positive response to high doses of levodopa; contact with toxic substances that cause parkinsonism;
- Stage 3. Supporting criteria
At least 3 signs of the following must be present: resting tremor, unilateral onset of the disease, persistent asymmetry with more pronounced symptoms on the side of the body on which the disease began, progressive course of the disease, good response to treatment with levodopa, maintenance of the effect of therapy for 5 years or more , severe dyskinesia induced by levodopa, long-term course of the disease (10 years or more).
Of course, family history is extremely important for the diagnosis of juvenile parkinsonism and of course it should be included in the criteria confirming the diagnosis; it is better to replace rest tremor with focal muscular dystonia. Juvenile parkinsonism is not characterized by dementia and unilateral onset. To confirm the diagnosis of idiopathic parkinsonism, which includes three forms: juvenile, early-onset parkinsonism and Parkinson's disease, innovative research methods are used, which are performed on modern equipment. Functional neuroimaging methods are used (positron emission tomography, single-photon emission computed tomography, proton magnetic resonance spectroscopy).
Classification
Juvenile parkinsonism in most cases is accompanied by three manifestations: hypokinesia, tremor and muscle rigidity. Depending on how this triad is composed, the following types of disease can be distinguished:
- trembling;
- trembling-rigid;
- rigid-trembling;
- akinetic-rigid;
- mixed.
In the first case, there is a small amplitude trembling of the head, jaw and tongue. Tremor is also present in the limbs. The trembling does not stop either at rest or in motion. At the same time, due to stress or a small emotional outburst, the rate of trembling increases significantly. Normal motor activity is also maintained, and muscle tone is within normal limits.
In tremor-rigid parkinsonism, the disease manifests itself by the appearance of tremor. Over time, the picture is complemented by a disorder of muscle tone, and hypertonicity may occur. Bradykinesia is absent or not clearly expressed.
The rigid-tremorous “variant” of the disease always begins with a sharp increase in muscle tone in the upper and lower extremities. Only then is tremor observed. Due to hypertonicity, the limbs take a forced position (flexion), then hypokinesia is expressed.
With akinetic-rigid parkinsonism, hypokinesia with increased muscle tone is observed. There is no trembling, as well as involuntary movements.
If features of each of the listed types of disease are present simultaneously, we are talking about mixed juvenile parkinsonism.
Parkinsonism in childhood and the role of neuronutrition
Parkinsonism is a neurological syndrome characterized by rhythmic muscle tremors, rigidity of movements, a mincing gait, a bent body position and a mask-like face; caused by damage to the basal ganglia of various origins (at any age). Parkinsonism is a progressive degenerative disease of the central nervous system (CNS). In classical neurology, parkinsonism is usually considered as a condition characteristic primarily of adult individuals. Pediatric neurologists periodically have to deal with several types of parkinsonism that occur before the age of 18 years. The literature reports the following variants of the disease in children: symptomatic parkinsonism, postencephalitic parkinsonism, parkinsonism with whooping cough, parkinson-like syndrome, as the main manifestation of viral encephalitis caused by the Epstein-Barr virus; generalized dystonia with onset in childhood; juvenile parkinsonism in combination with tourettism, hemiballismus with pantothenate kinase deficiency (Hallervorden-Spatz syndrome); parkinsonism among carriers of Gaucher disease, DOPA-dependent dystonia (Segawa disease), parkinsonism with mutational changes in lysosomal protein cerebrosidase; infantile dystonia-parkinsonism associated with homozygous loss-of-functions mutations in the gene encoding the dopamine transporter [1].
Classification
There are Parkinson's disease, that is, primary (idiopathic) parkinsonism; secondary parkinsonism (post-encephalitic, post-traumatic, vascular, drug-induced, etc.), as well as parkinsonism syndrome in degenerative and hereditary diseases of the central nervous system. The latter are relatively numerous.
The genetic classification considers the following forms of parkinsonism: Parkinson's disease with Lewy bodies; juvenile parkinsonism; Hunt's juvenile parkinsonism; familial Parkinson's disease type 1a.
For pediatric neurologists, two more conditions related to parkinsonism syndromes are important - infantile dystonia-parkinsonism and Segawa's disease. There are two variants of the latter (with autosomal dominant and autosomal recessive types of inheritance) [2].
Etiology and pathogenesis
In the development of parkinsonism, heredity (genetic predisposition), severe and repeated traumatic brain injuries, the influence of toxins, viruses, bacteria, viral-bacterial and viral-viral associations, etc. are important. According to KM Powers et al. (2009), epidemiological studies suggest that nutritional factors influence the etiology of parkinsonism [3].
Atherosclerotic changes in cerebral vessels, which are relevant in Parkinson's disease in adults, are usually not of great importance in children and adolescents.
Viral and viral-bacterial infections can lead to postencephalitic parkinsonism.
With a history of head trauma, the likelihood of developing parkinsonism increases by 4 times, and among individuals with a traumatic brain injury requiring hospitalization, by 8 times.
Cases of drug-induced parkinsonism predominantly relate to antipsychotic drugs, which cause a decrease in dopaminergic activity. Dopamine agonists may also cause symptoms of Parkinson's disease (by increasing the sensitivity of DOPA receptors).
Disturbances in tryptophan metabolism due to dopamine deficiency in the substantia nigra of the brain contribute to the development of Parkinson's disease. In parkinsonism, there is a decrease in the activity of tyrosine hydroxylase and DOPA decarboxylase.
RM Adibhatla and JF Hatcher (2008) emphasize that the development of parkinsonism is partly due to lipid peroxidation due to activation of phospholipases [4].
Pathogenetically, in parkinsonism, the death of dopaminergic neurons occurs in the substantia nigra, locus coeruleus, as well as in other dopamine-containing areas; At the same time, there is a decrease in the content of dopamine in the caudate nucleus and putamen.
Genetic aspects
In a quarter of cases, patients with parkinsonism have a complicated history. Defective genes that influence parkinsonism include PARK2 (Parkin), PARK3, PARK4, PARK6 (PINK 1), PARK7 (DJ-1), PARK8, PARK10, PARK11, SNCA, LRRK2, UCHL1, SNCAIP, GBA, NR4A2, CYP2D6.
The OMIM database of human genes and genetic diseases (Online Mendelian Inheritance in Man) presents the following variants of parkinsonism: late-onset Parkinson's disease (#168600); Parkinson's disease 1 autosomal dominant (#169601); Parkinson's disease 2 autosomal recessive juvenile (#600116); Parkinson's disease 4 autosomal dominant (#605543); Parkinson's disease 6 autosomal recessive with early onset (#605909); Parkinson's disease 7 autosomal recessive with early onset (#606324); Parkinson's disease 8 autosomal dominant (#607060). There is information about the casuistically rare Parkinson's disease 3 (OMIM #602404), Parkinson's disease 5 (caused by mutations in the UCHL1 gene, OMIM #191342), Parkinson's disease 12, associated with the X chromosome (OMIM #305557). There is Charcot-Marie-Tooth disease with ptosis and parkinsonism (OMIM No. 118301), described by R. Tandan et al. (1990) [1, 2, 5].
For DOPA-dependent dystonia (Segawa's disease) in the OMIM database, category #128230 is intended. The variant of the disease with an autosomal dominant type of inheritance is its equivalent and is associated with a mutation in the human GTP cyclohydrolase I (GCH1) gene. The described enzyme is involved in the conversion of guanosine triphosphate (GTP) to tetrahydrobiopterin (cofactor of tyrosine hydrolase, an enzyme involved in the control of dopamine synthesis). The autosomal recessive variant of Segawa disease (OMIM #605407) is characterized by the presence of the 11 p15.5 gene locus [6].
Clinical manifestations and diagnosis
The classic model of parkinsonism is Parkinson's disease (idiopathic parkinsonism). It is characterized by a symptom complex that includes tremor, rigidity and stiffness of muscles, hypo- and/or akinesia (due to small amplitude and “stiffness” of movements), disorders of muscle reflexes, hypomimia, autonomic and mental disorders, etc.
The earliest manifestations of parkinsonism in childhood include dystonia of the lower extremities or involuntary muscle contractions. Other early symptoms of parkinsonism in children include bradykinesia, tremors and muscle rigidity. As the disease progresses, children may develop problems with balance, dysarthria, and an inability to fully control facial expressions [1].
As in adult patients, children with parkinsonism may experience involuntary flexion of the feet and lower legs. The result of lower limb dystonia is gait disturbances. Unilateral or bilateral slowness of movement in one or more limbs (bradykinesia) results in the child's inability to complete rapid, repetitive movements and may be an early indication of bradykinesia.
In children, rigidity of the upper and/or lower extremities makes it difficult to move freely. Some children with stiff limbs assume unnatural postures, pressing their arms tightly against their body while walking.
In juvenile parkinsonism, patients may have uncontrollable tremors (rhythmic movements that affect one to several parts of the body—the arms, neck, vocal cords, head, torso, or lower extremities).
Additional signs of parkinsonism in children and adolescents may include difficulty balancing and maintaining proper body position. Some children experience hypomimia and dysarthria. Oculogyric crises occur in postencephalitic parkinsonism and consist of fixation of the gaze upward for several minutes to hours (sometimes the head is thrown back) [1].
Segawa's disease (DOPA-dependent dystonia) is a congenital, slowly progressive form of dystonia, combined with signs of parkinsonism. The disease manifests itself before the age of 10 years in children with local dystonia (the symptom complex of rigid-hypokinetic syndrome predominates: increased plastic tone, varying in different muscle groups; pathological postural attitudes, etc.) [6]. Then, over several years, the disease gradually spreads to other parts of the body. Symptoms fluctuate throughout the day. As indicated by M. Yu. Bobylova et al. (2009), the main clinical manifestations of Segawa’s disease can be represented by three groups of disorders: pyramidal (spastic paraparesis, foot clonus, hyperreflexia, pathological foot reflexes, contractures of the knee joints); extrapyramidal (fluctuating dystonia, bradykinesia, tremor, chorea, masked face, torticollis), mental/behavioral (emotional disorders, spatial representation disorders, learning difficulties) [7]. With DOPA-dependent dystonia, additional symptoms occur, such as scoliosis, so-called “horse foot”, dysarthria and sleep disorders. Segawa's disease must be differentiated from various forms of torsion dystonia, Wilson-Konovalov disease, cerebral palsy, and other residual conditions.
Juvenile parkinsonism. A special form of primary parkinsonism, but occurring among children (described in patients < 10 years of age). Characterized by classic symptoms of Parkinson's disease in the absence of dementia. Pathomorphological features of juvenile parkinsonism include neuronal degeneration and demyelination in the dense part of the substantia nigra and locus coeruleus (Lewy bodies are absent).
Hunt's juvenile parkinsonism. Differs from juvenile parkinsonism. Occurs in children and adolescents and is characterized by a slow progression. With juvenile Hunt's parkinsonism, patients have all the classic symptoms of parkinsonism.
Dystonia-parkinsonism syndrome with sudden onset was described in a 15-year-old girl by WB Dobyns et al. (1993) [8]. Subsequently, it turned out that the disease can debut at different ages (the youngest patient described in the literature fell ill at the age of 4 years). The disease is characterized by the sudden onset of dystonia with parkinsonism (primary bradykinesia and postural instability); a clear rostra-caudal gradient of involvement in the pathological process (face > arm > leg); bulbar lesions; lack of adequate response to L-DOPA therapy. The period of development of signs of parkinsonism can range from a few minutes to 30 days. The disease is often preceded by hyperthermia (or fever), stress or alcohol abuse (in adolescents). The described symptoms often become stationary (without further improvement); Sometimes there are repeated episodes of sudden worsening of all manifestations. The possibility of anxiety, depression and seizures has been reported. The age at the onset of the disease varies from 4 to 55 years. The diagnosis of dystonia-parkinsonism syndrome with sudden onset is established on the basis of clinical data. Molecular genetic testing is now available to identify the ATP1A3 gene (associated with sudden-onset dystonia-parkinsonism).
Prevention
Most recommendations for the prevention of parkinsonism relate to primary (idiopathic) parkinsonism, but there is reason to believe that these recommendations are also valid for other forms of parkinsonism.
American researchers indicate that daily consumption of coffee (1 cup per day) strengthens the blood-brain barrier and protects the brain from the harmful effects of cholesterol. The lower likelihood of parkinsonism with coffee consumption is thought to be due to caffeine's blockade of A2A adenosine receptors, which regulate the release of glutamate, which damages motor neurons. The GRIN2A gene (encoding the epsilon-1 subunit of NMDA receptors), which determines the preventive effect of coffee (and experimental drugs similar to it in action) in parkinsonism, has been discovered.
Reducing the consumption of milk and milk-based products may reduce the risk of developing parkinsonism. This is indicated by H. Chen et al. (2007), who noted a moderate (statistically significant) increase in the risk of Parkinson’s disease among individuals who regularly and relatively heavily consumed dairy products [9].
Since there are known cases of the development of parkinsonism after suffering from whooping cough, timely vaccination against this decreed childhood infection is necessary.
In case of dystonia-parkinsonism with sudden onset, psychological stress, excessive physical activity, hyperthermia, alcohol (an antinutrient), and digoxin drugs (presumably) should be avoided.
Treatment
Since dopamine does not penetrate the blood-brain barrier, drugs that are its precursors (DOPA derivatives: levodopa, Madopar, Nacom) are used in the treatment of parkinsonism. To suppress dopamine inactivation, MAO inhibitors (Deprenyl, Nailamide, Pyrazidol, etc.) are used [1].
Treatment for early-onset parkinsonism may differ from that for adult patients. In particular, levodopa is less widely used (due to the side effects of the drug and the advisability of its use at an older age) [1].
For dystonia-parkinsonism with sudden onset, benzodiazepines are used in high doses, and standard treatment for seizures is carried out. Drug correction of depression, anxiety and dysphagia is indicated. Physiotherapy and orthopedic treatment are provided to prevent contractures of the upper and lower extremities [10].
In the treatment of Segawa's disease, levodopa is used in relatively low doses (10–25 mg/kg/day), usually leading to a clear improvement in the patient's condition 2–4 days after the start of therapy. M. Yu. Bobylova et al. (2009) indicate that the average therapeutic dose is 375 mg of levodopa and 37.5 mg of carbidopa [7].
Nutritional and neurodietological aspects of parkinsonism
Dysphagia is a common manifestation of parkinsonism [11–13]. To correct it in childhood, dietary methods include additional culinary food processing (grinding, homogenization), as well as the principles of clinical nutrition (including enteral and parenteral nutrition and gastrostomy).
In Parkinsonism, nutritional disorders such as obesity and malnutrition deserve attention. Excess body weight aggravates the underlying manifestations of the disease, but it is not entirely clear whether the metabolic syndrome associated with obesity has an adverse effect on the symptoms of parkinsonism, or whether the disease itself contributes to the development of obesity. Equally significant in parkinsonism is malnutrition. H. Chen et al. (2003), G. Wang et al. (2010) note the phenomenon of weight loss in parkinsonism, revealing a direct correlation between the severity of parkinsonism and the duration of the disease [14, 15].
Enteral nutrition is widely used to provide the necessary nutrients to patients with parkinsonism, when it is not possible to introduce the required amount of nutrients and energy orally. Tube feeding is also used for dysphagia and/or nutritional disorders. There is evidence that with enteral nutrition in patients with parkinsonism taking levodopa, control over disease symptoms may be impaired, which is associated with an undesirable interaction between the protein component of the tube mixtures and the antiparkinsonian drug. The need to use total parenteral nutrition in parksinsonism rarely occurs, as does the installation of a gastrostomy tube [10].
It is recommended to eat more fruits and vegetables (sources of vitamins and minerals), as well as some berries (in particular, cherries, cherries and barberries). All vegetables and fruits should be consumed primarily fresh (raw).
Excessive fat consumption is a risk factor for the development of parkinsonism at any age. The predominance of total fat and saturated fat in the diets of patients with parkinsonism is indicated by H. Chen et al. (2003), recommending the replacement of animal and saturated fats with polyunsaturated and vegetable fats [16]. The protective effect of unsaturated fatty acids in Parkinson's disease was described by LM de Lau et al. (2005) [17]. According to JK Morris et al. (2010), manifestations of parkinsonism (neurodegeneration) worsen when consuming a high-fat diet [18]. Y. Miyake et al. (2010) do not rule out that the condition of patients with parkinsonism worsens with increased dietary intake of arachidonic acid [19].
It is interesting that low dietary intake of cholesterol contributes to the development and worsening of Parkinson's disease (in male patients). The unfavorable effect of low cholesterol intake is especially often realized when there is a high intake of iron from food [2]. Based on the possible role of iron in neuronal damage in Parkinson’s disease, CW Levenson (2003) suggests the need to limit this microelement in the diet (to prevent a decrease in dopamine levels in the central nervous system and reduce motor disorders) [20].
Certain dietary excitotoxins (aspartate, monosodium glutamate, hydrolyzed vegetable protein, cysteine) can lead to the development of parkinsonism or worsen its manifestations, and therefore it is recommended to avoid products (industrial production) containing them.
Low protein intake allows optimization of ongoing drug treatment for parkinsonism (L-DOPA), which has been known for a number of years [21–23]. L. Haglin and B. Selander (2000) report the use of a “protein redistribution” diet, based on the fact that certain amino acids can compete with L-DOPA in the intestine and at the level of the blood-brain barrier, that is, limiting dietary protein in the diet potentially allows normalize fluctuations of motor dysfunction in parkinsonism [24]. E. Sereda et al. (2010) confirm the effectiveness of this approach to nutrition in parkinsonism and recommend the use of specialized low-protein foods used in the treatment of patients with chronic renal failure [25].
Vitamin C is an antioxidant that slows the progression of the disease and allows you to delay the initiation of pharmacotherapy. To cover the increased needs for ascorbic acid in patients with parkinsonism, its consumption at a dose of 3000–6000 mg/day is recommended [26].
According to SM Zhang et al. (2002), consumption of tocopherol in high doses has a beneficial effect on the manifestations of parkinsonism (implementation of the antioxidant properties of the vitamin) [26]. Depending on the age of the patients, they are advised to take vitamin E in doses of 200 IU/day (or 400 IU every other day).
The use of B vitamins is considered especially important in parkinsonism. Since the production of dopamine depends on adequate intake of this vitamin, it is recommended to take pyridoxine 50–75 mg 3 times a day (with meals). Pyridoxine should not be taken if levodopa is prescribed.
Vitamin B2 (riboflavin) deficiency in parkinsonism contributes to the development of depression, causes neuronal damage and induces a decrease in the level of neurotransmitters. In this regard, it is recommended to take riboflavin in doses of up to 50 mg 3 times a day (with food). Vitamin B3 (niacin) helps maintain the immune system and is also a means of preventing depression and irritability (prescribed in doses of up to 50 mg 3 times a day, with meals).
The role of vitamin D supplementation in the correction of parkinsonism manifestations cannot be ruled out; this was reported by ML Evatt et al. (2011) [27].
Of the mineral substances in parkinsonism, calcium (anti-osteoporosis effect), magnesium (provides neuromuscular functions), potassium (ensures adequate transmission of nerve impulses/muscle contractions) and sulfur (antioxidant) deserve special attention.
Coenzyme Q10 promotes increased production of cellular energy, slows down the death of brain neurons and the progression of the disease. Coenzyme A acts synergistically with coenzyme Q10, balancing metabolism, reducing depression and fatigue, and increasing vitality.
Consumption of caffeine in moderate doses has a positive effect on the neurological status in various forms of parkinsonism, but in childhood this central nervous system stimulant can act as an antinutrient.
The use of hyperketogenic diets in the treatment of parkinsonism was reported by TB Vanitallie et al. (2005), emphasizing the effectiveness of ketones in normalizing the activity of the complex I defect in parkinsonism [28]. M. Gasior et al. (2006), B. Cheng et al. (2009) confirm the positive role of ketogenic diets (KD) in parkinsonism (neuroprotective and “disease-modifying” properties) [29, 30].
The use of phytochemicals is reviewed by R. Pal et al. (2011) [31]. For parkinsonism, it is recommended to use the following edible plants to detoxify the liver: burdock, dandelion, ginger, milk thistle; to stimulate the thymus and lymphatic system: cayenne, goldenseal, mullein, Eleutherococcus senticosus, yarrow; for blood cleansing: hawthorn, red clover, sarsaparilla, licorice. Yellow sorrel is used to detoxify the blood and liver. Black cohosh, catnip, passionflower, skull cap and valerian root have anti-stress and neurotrophic effects.
P. Rojas et al. (2009) used the dietary supplement EGb761 (Ginkgo biloba extract) for Parkinson’s disease, which was accompanied by normalization of copper homeostasis and its content in various brain structures [32].
Thus, the role of nutrition in parkinsonism should not be ignored. The described nutritional aspects of parkinsonism indicate the relevance of the neuronutritional approach to this pathology.
Literature
- Koller WC Treatment of early Parkinson's disease // Neurology. 2002, v. 58, s. 79–86.
- Segawa M. Segawa disease // Brain Nerve. 2008, v. 60, p. 5–11.
- Powers KM et al. Dietary fats, cholesterol and iron as risk factors for Parkinson's disease // Parkinsonism Relat. Discord. 2009, v. 15, p. 47–52.
- Adibhatla RM, Hatcher JF Altered lipid metabolism in brain injury and disorders. Subcell // Biochem. 2008, v. 49, p. 241–68.
- Tandan R. et al. Benign autosomal dominant syndrome of neuronal Charcot-Marie-Tooth disease, ptosis, parkinsonism, and dementia // Neurology. 1990, v. 40, s. 773–779.
- Segawa M. et al. Hereditary progressive dystonia with marked diurnal fluctuation // Adv. Neurol. 1976, v. 14, p. 215–33.
- Bobylova M.Yu. et al. Dopa-dependent dystonia (Segawa's disease) // J. neurol. psychiatry. 2009, v. 109, no. 8, p. 73–76.
- Dobyns WB et al. Rapid-onset dystonia-parkinsonism // Neurology. 1993, v. 43, s. 2596–2602.
- Chen H. et al. Consumption of dairy products and risk of Parkinson's disease // Am. J. Epidemiol. 2007, v. 165, p. 998-10-06.
- Deanne KH et al. Non-pharmacological therapies for dysphagia in Parkinson's disease // Cochrane Database Syst. Rev. 2001, 1: CD002816.
- Potulska A. et al. Swallowing disorders in Parkinson's disease // Parkinsonism Relat. Discord. 2003, v. 9, p. 349–353.
- Miller N. et al. Hard to swallow: dysphagia in Parkinson's disease // Age Ageing. 2006, v. 35, p. 614–618.
- Michou E., Hamdy S. Dysphagia in Parkinson's disease: a therapeutic challenge? // Expert Rev. Neurother. 2010, v. 10, p. 875–878.
- Chen H. et al. Weight loss in Parkinson's disease // Ann. Neurol. 2003, v. 53, pp. 676–679.
- Wang G. et al. Malnutrition and associated factors in Chinese patients with Parkinson's disease: results from a pilot investigation // Parkisonism Relat. Discord. 2010, v. 16, p. 119–23.
- Chen H. et al. Dietary intakes of fat and risk of Parkinson's disease // Am. J. Epidemiol. 2003, v. 157, p. 1007–1014.
- De Lau LM et al. Dietary fatty acids and the risk of Parkinson disease: the Rotterdam study // Neurology. 2005, v. 64. S. 2040–2045.
- Morris JK et al. Neurodegeneration in an animal model of Parkinson's disease is exacerbated by a high-fat diet // Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, No. 299 (4), R1082–1090.
- Miyake Y. et al. Dietary fat intake and risk of Parkinson's disease: a case-control study in Japan // J. Neurol. Sci. 2010, v. 288, p. 117–122.
- Levenson CW Iron and Parkinson's disease: chelators to the rescue? // Nutr. Rev. 2003, v. 61, p. 311–313.
- Barichella M. et al. Special low-protein foods ameliorate postprandial off in patients with advanced Parkinson's disease // Mov. Discord. 2006, v. 21, p. 1682–1687.
- Gao X. et al. Prospective study of dietary pattern and risk of Parkinson disease // Am. J. Clin. Nutr. 2007, v. 86, p. 1486–1494.
- Gaenslen A. et al. Nutrition and the risk for Parkinson's disease: review of the literature // J. Neural. Transm. 2008, v. 115, p. 703–713.
- Haglin L., Selander B. Diet in Parkinson's disease // Tidsskr. Nor. Laegeforen. 2000. v. 120, p. 576–578.
- Sereda E. et al. Controlled-protein dietary regimens for Parkinson's disease // Nutr. Neurosci. 2010, v. 13, p. 29–32.
- Zhang SM et al. Intakes of vitamins E and C, carotenoids, vitamin supplements, and PD risk // Neurology. 2002, v. 59, pp. 1161–1169.
- Evatt ML et al. High prevalence of hypovitaminosis D status in patients with early Parkinson disease // Arch. Neurol. 2011, v. 68, p. 314–319.
- Vanitallie TB et al. Treatment of Parkinson's disease with diet-induced hyperketonemia: a feasibility study // Neurology. 2005, v. 64, s. 728–730.
- Gasior M. et al. Neuroprotective and disease-modifying effects of the ketogenic diet. Behav // Pharmacol. 2006, v. 17, p. 431–439.
- Cheng B. et al. Ketogenic diet protects dopaminergic neurons against 6-OHDA neurotoxicity via up-regulating gluthataione in a rat model of Parkinson's disease // Brain Res. 2009, No. 1286, p. 25–31.
- Pal R. et al. Nitrosative stress-induced Parkinsonian Lewy-like aggregates prevented through phytochemical analog intervention // Biochem. Biophys. Res. Commun. 2011, v. 404, p. 324–329.
- Rojas P. et al. Effect of EGb761 supplementation on the content of copper in mouse brain in an animal model of Parkinson's disease // Nutrition. 2009, v. 25, p. 482–485.
V. M. Studenikin, Doctor of Medical Sciences, Professor V. I. Shelkovsky, Candidate of Medical Sciences S. Sh. Tursunkhuzhaeva N. G. Zvonkova, Candidate of Medical Sciences
FSBI NTsZD RAMS, Moscow
Contact information for authors for correspondence
Symptomatic picture
Most often, the disease manifests itself clearly after 10 and before 25 years of age. Symptoms develop bilaterally, which distinguishes juvenile parkinsonism from known Parkinson's disease. A delay or other disruption in motor skills appears, and gesticulation worsens. Facial expressions may be weakened, and in general, the motor amplitude when performing everyday activities and movements decreases.
If previously the child could easily fasten a button or lace his shoes, then after the manifestation of the disease these actions cause great difficulty.
In general, the child becomes slower, movements become “poorer”, becoming more constrained.
The gait becomes “senile”: the patient shuffles, taking small steps. Synchronicity in the movement of arms and legs when walking disappears.
Then speech disorders arise. Some people's speech becomes angular, while others may experience a sharp slowdown in the rate at which they pronounce words.
Any muscle tension causes trembling in the head and limbs. The tremor persists even at rest. Most affected children have muscle rigidity. Due to constant muscle tension (hypertonicity), arms and legs can bend, taking a static forced position.
Symptoms may become more or less severe during the day. So, after sleep, the symptoms practically disappear, and then in the evening they increase again. Dystonic symptoms may manifest themselves - most often in the feet.
Juvenile parkinsonism is characterized by preservation of intellectual abilities and normal functioning of the cognitive sphere. Mental development is carried out according to age norms.
Diagnostics
MRI of the brain
- Cost: 14,000 rub.
More details
First, the doctor collects anamnesis. The patient is asked the following questions:
- How long ago did the symptoms first appear and how quickly did they progress?
- Does the tremor get worse at rest?
- Are there hereditary prerequisites for the development of the disease?
- Does the patient work in industries with increased toxic hazards?
- Is the patient taking medications that increase the risk of developing parkinsonism?
- Have there been severe episodes of infectious disease in the recent past?
- Were there any head injuries?
Then the doctor conducts a standard neurological examination for such complaints: assesses gait, muscle tone, tremor pattern, etc.
The next stage is a pharmacological test. It consists of prescribing a drug based on dopamine or similar substances to the patient. If you have parkinsonism, this helps reduce symptoms.
Often a consultation with a psychologist is required to assess the cognitive and emotional sphere. Typically, standard tests and questionnaires are used for this.
The diagnosis can be confirmed with an MRI - the examination will show pathological areas in the area responsible for muscle tone and coordination. These highlighted areas show dead neurons. MRI can also confirm or exclude a tumor.
Diagnostics ends with a diagnosis, according to which treatment is prescribed.
Modern diagnostic measures
It is important to detect the disease in time, so at the first signs of pathology you should consult a doctor. Usually the diagnosis is made during the first examination by a neurologist. A competent doctor will immediately note bradykinesia, increased muscle tone and tremor. The tendon reflex will then be tested. In childhood parkinsonism it is also significantly increased. The child must be placed in a special position to check the so-called pyramidal signs (Babinsky reflexes).
Next, electrophysiological examinations are carried out:
- EEG;
- electromyography.
Based on the results of these procedures, this diagnosis is confirmed. Usually the picture is expressed by a decrease in the bioelectrical activity of the cerebral hemispheres. This suppression is especially pronounced in akinetic-rigid juvenile parkinsonism.
An MRI is also required. But, as a rule, with such a disease, no serious changes are visible. Such an examination is prescribed in order to exclude some “counter” diseases of the central nervous system. Only late changes can be recorded on tomography:
- on the caudal nucleus;
- on the globus pallidus;
- black substance.
These changes are already considered basal and manifest themselves at critical stages of the disease.
To find out how dopamine synthesis proceeds and how difficult it is, the patient is referred to a functional neuroimaging procedure. To do this, a special substance is injected, which should normally concentrate in a special area of the brain.
Additionally carried out:
- PET-CT brain;
- SPECT;
- MR spectroscopy.
Since the disease occurs for genetic reasons, the child is sent for examination to a geneticist. The specialist identifies the specific gene in which there is a malfunction, and also finds out the percentage of its heritability in the future.
The doctor also needs to distinguish juvenile parkinsonism from that of the secondary type. It occurs as a result of drug addiction or a malfunction in the endocrine system.
Parkinson's disease in children
Parkinson's disease is not “illness of people of advanced age,” as it is commonly believed. It manifests itself in three-dimensional paralysis, associated with changes in the brain. This pathology is considered to be chronic and there are only rare episodes when it is possible to effectively overcome it.
The causes of Parkinson's disease in children are the same as in adults:
- Infectious illness with further complications on the brain;
- Trauma to the brain;
- Gostri otruennia;
- Systemic illness, swelling, blood ailments;
- Spadkov's skill;
- Damage to the nervous system.
In fact, the symptoms of Parkinson's disease in children are practically not comparable to those of older people. Ale presence and special features.
Symptomatic illness in children begins to manifest itself as a result of dystonia of the lower limbs, as soon as normal walking becomes difficult. There is also an increase in behavior in the Rukhs. You can throw one of the ends or throw the whole body. Children with this pathology cannot completely relax when walking, so it appears that the child is cold.
Well, the three-fold ending is the most important and important symptom of parkinsonism. This kind of hat can be extended not only to the ends, but also to the head, toulub. Most of the time you feel good in the state of peace. Before speaking, this may still be the cause of unclear speech.
Signs of Parkinson's disease in a child are not to speak of 100% illness. To confirm the diagnosis, it is necessary to contact a child neurologist. After examination and a number of necessary investigations, it will be possible to accurately say about the presence of pathology in the child’s body.
The following procedures may be necessary:
- Ultrasound and Doppler examination of the vessels of the neck and cerebrum;
- X-ray examination of the cervical region of the ridge;
- Computer tomography of the brain;
- Rheoencephalography of the head and spine.
The treatment of Parkinson's disease in most cases extends throughout the life of the patient and involves a complex nature. Drug therapy in young adults tends to be more progressive, which reduces symptoms and reduces the level of healthy neurons. In addition, children are susceptible to the development of confusion, which is why mental health problems are often absent when they grow up.
Who asks nutritionists what mothers can do with children with Parkinson's disease? Unfortunately, there is no clear answer to this diet. So, there are a lot of known episodes when girls with such a pathology were chewed and healthy children were taken away. Or we can more accurately recommend a doctor who treats parkinsonism after the patient has been completely restrained.
As a method of prevention, to avoid the development of Parkinson's disease, take it as a priority to regularly see a neurologist together with your baby. Carefully treat all illnesses in the early stages of their development and follow the path of health. This will help minimize the chances of developing parkinsonism.
Well, if you have any doubts, immediately contact a neurologist at the Weekend Clinic !
! I wish you good health!