More useful information about other diseases starting with the letter “K” here: Causalgia, Brain cyst, Cluster headache, Tick-borne encephalitis, Kozhevnikov epilepsy, Colloid cyst of the third ventricle, Coma, Compressive myelopathy, Balo concentric sclerosis, Radicular syndrome, Corticobasal degeneration, Craniovertebral anomalies, Craniospinal tumor, Craniopharyngioma, Myasthenia gravis crises, Hemorrhage into the ventricles of the brain.
What does hemorrhage into the ventricles of the brain mean?
Hemorrhage into the ventricles of the brain is a disease that is one of the forms of malfunction of the circulatory system of the brain. The presented disease is most often diagnosed in modern medicine. Neurologists say that the disease is caused by arterial hypertension (the treatment of which has been neglected for a long time), bad habits (smoking, alcoholic beverages, drugs) and the use of pharmacological agents that can lead to poor blood clotting. To establish a conclusion, the doctor conducts a detailed conversation with the patient, finds out existing complaints and problems, and also prescribes a certain list of tests for a final affirmative diagnosis. Therapeutic treatment helps eliminate the formed edema, stabilize lung function and normalize blood pressure.
Diagnostics
A doctor may suspect a brain hemorrhage based on typical symptoms, especially if they are associated with injury or other risk factors.
But the gold standard for diagnosis is brain CT. On the first day after the onset of hemorrhage, the data will be most accurate, even more significant than with MRI. On tomograms, fresh hematomas are clearly visible; the doctor can determine their exact location, size and shape. In addition, he immediately assesses how damaged the brain structures, membranes and cerebrospinal fluid circulation system are. If hemorrhage is detected after 3 days or more, an MRI will be more accurate. It will better identify a hematoma in which the blood already has oxidized, partially disintegrating hemoglobin.
If these are young people without hypertension, they may be prescribed angiography of cerebral vessels. Additionally, an ECG, chest X-ray, blood tests for electrolyte levels, PTT with APTT (coagulation indices) are performed.
Brief information
In neurology, a similar disease of hemorrhagic type is classified as stroke. The anomaly has different names. According to surveys and average statistical information received from practicing doctors, the described deviation from the norm ranks first in the number of deaths of patients around the globe. Based on publicly available information, such a process can cause death within 48 hours of onset in 60% of cases. The risk increases significantly during the recovery period after a stroke. People who survive a critical attack have a 90% chance of bleeding.
Basically, the largest number of recorded pathologies is observed in the population of retirement age, whose age has exceeded the mark of 50 years. However, in addition to this, danger threatens not only people with arterial hypertension, but also any other abnormalities that have absolutely nothing to do with the level of pressure.
Types of hemorrhage
The compilation of classes of the described disease was created in the late 90s, as a result of which the list was included in international medical documents on the classification of diseases. Based on the source in the form of ICD-10, the presented pathological process is divided into several forms:
- Subependymal (SEC).
- SEC with damage to the extreme parts.
- SEC with progression to areas and substance of the brain.
In addition, there are additional differences between IVH, which differ in location:
- Changes in the lateral structures - begins from nearby soft cavities and manifests itself as a gradual filling of the entire volume with further leakage into other areas. In the case of the formation of a surplus, the size of the main organ begins to increase, as a result of which symptoms of a neurological nature progress (if only one object is filled, the specialists’ prognosis is positive, since this process is similar to a parenchymal disorder).
- Location in the third ventricle - the medial zones of parenchymal disorders become the culprit.
- The focus of inflammation in the 4th lobe originates from the dorsal perimeter of the brainstem or cerebellum.
Degrees of intraventricular hemorrhage in adults
For the diagnosis of nosology, a full-term baby is prescribed three clinical and instrumental methods - CT, ultrasound, MRI.
The degree of intraventricular bleeding according to ultrasound results:
- Subepindymal bleeding of no more than ten percent of the tissue volume - the first stage;
- Filling of the ventricle with blood by 40-50% is the second stage;
- Periventricular hemorrhage over 50% of the volume is the third stage.
Some classifications include grade IV, in which extensive ventricular filling with parenchymal hemorrhage is observed.
Magnetic resonance and computed tomography of children reveals ventriculomegaly and intracerebral infarctions. In inflammatory processes, examination of the cerebrospinal fluid can reveal a violation of the composition of the cerebrospinal fluid.
Degrees of ventriculomegaly:
- Lightweight;
- Moderate;
- Heavy.
The expansion of the ventricle in the first stage reaches 1 cm. In severe cases, ventriculomegaly is more than 1.5 cm.
A favorable prognosis is observed in the first degree of pathology, when the process spreads throughout the germinal matrix. Surgical treatment is rarely performed, since conservative medications can eliminate the consequences.
In the third degree, cerebral edema and ventriculomegaly develop. According to some scientists, an intracerebral hematoma is a continuation of hemorrhage in the lateral ventricles.
X-ray grades of IVH:
- The first degree is the accumulation of blood under the ventricular lining without penetration;
- IVH of the second degree - blood penetrates into the ventricular space, but the cavity does not expand;
- Filling more than half of the lumen – third degree;
- Spread of blood beyond the ventricular space with extensive permeation, damage to the nerve sheaths - fourth radiological degree.
Stages of hemorrhagic permeation of the brain in premature infants:
- Destruction of the wall of the third ventricle with perifocal massive hemorrhage, filling of the ventricular space, necrotic changes in the brain parenchyma;
- Migration of blood from the lateral ventricle with filling the cavity of the third ventricle, increasing the volume of the brain;
- The predominance of parenchymal foci near the visual thalamus, followed by a rapid increase in symptoms with damage to the intrathecal cavities, anterior and posterior horn;
- Filling the lateral ventricle exclusively;
- Extensive intracerebral hemorrhages with displacement of the brain stem, development of contralateral hydrocephalus;
- Bleeding in the third ventricle, thalamus;
- Hemorrhagic permeation of the cerebellum extending into the third ventricular space. Has a high mortality rate.
Morphological classification of stages of intracerebral hemorrhage:
- Subepindeminal;
- Intraventricular-subepindeminal;
- Periventricular-intraventricular-subepindeminal.
The latter option is characterized by damage to the trunk, increased intracranial pressure, and impaired respiratory activity.
Main factors of appearance and symptoms
There are two stages of bleeding - primary and secondary. PIH is associated with arterial problems in the body or amyloidosis in the cerebral vessels, so they are diagnosed in rare situations. Based on some data, such an anomaly occurs once in 300 patients. The second version of FFM is formed due to the incorrect use of certain medications (for example, antiplatelet substances or fibrinolytic drugs), the presence of a neoplasm capable of breakthrough, or cancerous tumors.
With such an illness, the patient experiences a rapid increase in depression of thinking. Usually, a coma appears after a stroke in the first hours. Only with a gradual progression of the disease and, most importantly, a minimum amount of fluid released, the consciousness of the individual remains stable for a long time and decreases gradually.
Often, bleeding occurs along with:
- meningeal manifestations and gag reflexes.
- Extreme sweating.
- Trembling, similar in nature to chills.
- Change in skin color.
- Abnormal accumulations of blood cells in the vascular ducts, occurring in the face, torso, arms and legs.
- An initial decrease in body temperature, and as a result a rapid jump reaching above 40 degrees.
A typical symptom of such a disorder in the body is a decrease in the tone of muscle tissue, which manifests itself in the form of hormetonic syndrome or an irreversible stage of coma. In the first method, an attack of increased muscle activity in the inflamed area begins. This symptom appears due to external conditions. In the second, deformations develop exclusively in the extensor layers. The patient takes a supine position and arches his back, while tilting his head. The upper limbs are clasped and the forearms are facing inward. Also, it may be accompanied by paresis in the opposite extremities from the pathology, the formation of reflexes in the tendons, the presence of anomalies and lack of action in the abdominal region, disruption of the performance of the pelvic region and its organs.
During the disease, which is localized in the third compartment, difficulties arise in breathing and in the functioning of the circulatory system, and hormetonia syndrome has a bilateral effect. With a deviation located in the fourth ventricle, hiccups and problems with swallowing saliva are caused, uncontrolled movements are not observed, and signs of hormetonia are less noticeable. If the described process continues for a long time in a patient, then an increase in the amount of fluid begins, which provokes an increase in VD, swelling and compression of the nerve areas responsible for the life support of the entire body. The supplement favors disorders of the heart and vascular system.
Hemorrhagic stroke (hypertensive intracerebral hemorrhage)
Department of Emergency Neurosurgery > Diseases
Hemorrhagic stroke (hypertensive intracerebral hemorrhage) is a polyetiological nosological form characterized primarily by parenchymal hemorrhage.
Treatment of patients with hemorrhagic stroke is an important social, medical and economic problem. Hemorrhagic stroke accounts for 8-20% of all patients with acute cerebrovascular accidents. The incidence of hemorrhagic stroke is 10-35 per 100,000 population and increases with age. This disease is characterized by the highest mortality and disability among all subgroups of acute cerebrovascular accidents. Mortality during the first month after hemorrhage is 30-60%, and 2/3 of surviving patients remain disabled.
Etiology and pathogenesis of hemorrhagic stroke
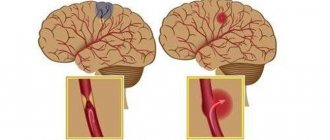
The main cause of hemorrhagic stroke is hypertension and associated microangiopathy. Long-term arterial hypertension contributes to the formation of lipohyalinosis, and subsequently fibrinoid necrosis of the walls of perforating arteries, characterized by the absence of anastomoses with other vessels (Fig. 1). With an increase in blood pressure, the walls of these vessels rupture with the formation of hematomas (putamenal, cerebellar, subcortical) or hemorrhagic impregnation of the thalamic and stem parts of the brain with blood components through pathologically altered vascular walls. Such hemorrhages are called hypertensive (primary).
Much less frequently, the causes of intracerebral hemorrhages (secondary) are ruptures of vascular malformations, vasculopathy, hemorrhages in a tumor, and bleeding disorders.
After intracerebral hemorrhage, blood flow in the perihematomal area is reduced, but due to reduced metabolism it does not suffer from ischemia. The breakdown products of hemorrhage cause the development of cytotactic, and after disruption of the blood-brain barrier, vasogenic edema. An inflammatory reaction, apoptosis and necrosis of nervous tissue develops in the perihematomal area. The formation of perihematomal edema increases compression and dislocation of the brain.
Clinical picture and diagnosis of hemorrhagic stroke
Hypertensive intracerebral hemorrhages are characterized by an acute course of the disease, the presence of cerebral, meningeal, focal, and dislocation symptoms. The clinical picture of the disease is determined primarily by the localization of the hemorrhagic stroke. Most often, hypertensive hematomas are located in the putamen (55%), less often subcortically (15%), in the optic thalamus (10%), cerebellum (10%), and brain stem (10%).
Methods for instrumental diagnosis of hemorrhagic stroke: X-ray computed tomography, magnetic resonance imaging, cerebral angiography, recording of acoustic brainstem evoked potentials, electrocardiography, echocardiography.
Cerebral angiography is performed to exclude an aneurysm or vascular malformation in young patients (under 45 years old), in the absence of a history of arterial hypertension, in the presence of basal subarachnoid hemorrhage and in subcortical localization of the hematoma.
Surgical treatment of hemorrhagic stroke
Goals of surgical treatment:
- reduction of mass effect
- reduction of local and general intracranial pressure
- reducing the release of neurotoxic substances from the hematoma.
Objectives of surgical treatment:
- Maximum complete removal of blood clots
- Minimal damage to surrounding brain parenchyma.
Surgery is necessary if the patient has:
- subcortical or putamenal hemorrhage with a volume of more than 20-30 cm3. or with a diameter of more than 3 cm, leading to brain dislocation and severe neurological deficit;
- cerebellar hematoma with a volume of more than 10-15 cm3, leading to compression of the brain stem and/or occlusive hydrocephalus;
- hematoma of the thalamus, accompanied by hemotamponade of the lateral ventricles and occlusive hydrocephalus.
The advisability of surgical intervention is discussed for:
- thalamic hematoma with a volume of more than 10 ml, accompanied by neurological deficit;
- pontine hematoma, accompanied by severe neurological deficit.
To treat hypertensive hemorrhages, open surgery by craniotomy, puncture operations (aspiration and local fibrinolysis, endoscopic aspiration of the hematoma and their combination) and drainage of the cerebral ventricles are used. Open surgical treatment is currently used in no more than 25% of patients. It is indicated when the hematoma is located close to the surface of the brain. In this case, the intervention does not cause additional trauma to the patient’s brain. In case of deep hemorrhages in the cerebral hemispheres or in the cerebellum, open intervention has to be resorted to as a life-saving operation in patients in serious condition.
In the majority of patients - about 75% - low-traumatic puncture operations are used to evacuate hematomas. An instrument with a diameter of 2-7 mm is inserted into the hematoma through a small trepanation hole and it is aspirated simultaneously or over time through a special catheter or endoscope. The accuracy of the instrument entering the hematoma is ensured by modern navigation systems (ultrasonic, electromagnetic or infrared). Computer tomograms of the patient are loaded into the navigation station, a virtual model of the location of the hemorrhage is built, and during the operation the surgeon can observe in real time the location of the hematoma and the surgical instrument relative to each other.
Rice. Image from the navigation station screen. The upper left square is a real image of the operation progress from the endoscope. The remaining three squares display a virtual picture of the location of the endoscope (blue line) relative to the hematoma (circled in lilac) at the stage of pointing the instrument at the target.
With the development of occlusive hydrocephalus, drainage of the ventricles of the brain is performed. If the ventricles are tamponed with blood clots and drainage alone does not lead to regression of cerebral hydrops, then it is supplemented by local fibrinolysis of blood clots. The most modern methods of hemorrhagic stroke surgery include video endoscopic. Neuroendoscopes allow, both under visual control and under the virtual control of a navigation station, to carry out low-traumatic removal of even large-sized hemorrhages.
Contraindications to surgical treatment.
Absolute:
- disturbance of wakefulness to coma;
- unstable hemodynamics.
Relative:
- severe somatic pathology (coagulopathy, diabetes mellitus, cardiopulmonary and renal failure in the decompensation stage);
- high, uncorrectable blood pressure;
- age of patients over 70-75 years
Over the past 30 years, every year at the Research Institute of Emergency Medicine named after. N.V. Sklifosovsky operates on more than 35–50 patients with hemorrhagic stroke. To remove hematomas, microsurgical and endoscopic methods and various neuronavigation systems are used. Conducting a timely comprehensive examination and neurosurgical treatment allows us to achieve a good outcome of the disease in most patients and postoperative mortality of less than 20%. Employees of the neurosurgery clinic regularly organize master classes on the surgical treatment of hemorrhagic stroke. They speak at national and international conferences with the results of their research.
Diagnostic techniques
To establish a correct conclusion, experts will need to conduct an evaluative check of the person’s medical history, that is, find out the presence of blood diseases, previous hemorrhagic strokes, what medications the patient took that contributed to poor clotting, etc. In addition, doctors conduct a standard examination and prescribe additional tests to create a full picture.
You need to understand that if an anomaly is likely to develop, you should urgently go to the nearest medical center to provide professional clinical care. Also, experts do not exclude the possibility that the patient will have to undergo resuscitation measures on the way to the hospital. In the inpatient building, doctors write out directions for the following procedures:
- MRI scan or computed tomogram, depending on the presence of contraindications.
- Donation of blood cells for analysis, during which there will be a report on the number of platelets in the body.
- Coagulogram examination.
- Electrocardiogram.
- Check blood pressure readings.
If doctors do not have the opportunity to perform magnetic resonance or computer diagnostics on a person due to a coma, then echo-encephalography is prescribed. At certain points, it may be necessary to perform a lumbar puncture in order to distinguish hemorrhage, which provokes the entry of fluid into the spinal substance, from an ischemic stroke.
Is there a way to prevent intracerebral hematoma?
Typically, preventive measures to prevent intracerebral hematoma are reduced to the maximum exclusion of the factors that provoke it (especially with a potential predisposition to hemorrhagic stroke). Therefore, the doctor may recommend to the patient:
- control of blood and intracranial pressure
- giving up bad habits (in particular, smoking and alcohol abuse)
- relaxation practice (to successfully overcome stress)
- moderate exercise and walking
It is important to remember that intracerebral hematoma is a very insidious pathology due to its consequences. That is why it is so important for the patient to visit a modern clinic in a timely manner for proper diagnosis and treatment.
Experienced medical specialists are always ready to come to your aid at the slightest suspicion of this disease! Don't waste your precious time and be healthy!
Treatment Options
The first point for medical staff is the prompt provision of first emergency aid and the immediate implementation of basic level treatment - stabilization of the functions of the heart and lungs, as well as monitoring of blood pressure levels and regulation of the constant flow of internal processes of the body.
In addition, doctors prescribe therapy to get rid of symptoms: intravenous injections that have an anticonvulsant effect, as well as help resolve swelling and normalize blood pressure (in addition, a drug can be used to stop vomiting). To fully stop bleeding, a treatment plan is currently being developed by the most qualified scientists. The pathogenic option involves maintaining optimal blood pressure levels and pumping out excess blood through surgery. Such procedures include:
- The use of agents that have a neurotrophic effect and increase metabolism.
- Taking antioxidants (including vitamin E) and substances that block calcium ducts.
The surgical procedure is selected on an individual basis.