In this article we will tell you:
- Types of nystagmus
- Physiological nystagmus
- Pathological nystagmus
- Reasons for the development of nystagmus
- Symptoms of nystagmus
- Prevention and treatment of ocular nystagmus
The human eyeball is in constant motion. We can squint, raise up, or, conversely, lower our eyes at any time. Such movements are voluntary - that is, they depend on our desire, on those impulses that the brain transmits to the muscles at the behest of our consciousness.
However, there are also movements that occur involuntarily. Some of them are considered normal, part of a reflex, and do not interfere with us in everyday life. Others are pathological in nature and indicate the development of a particular disease. A clear illustration of these processes is nystagmus of the eyeball - repeatedly repeated oscillatory movements of the human eyes, which can be either a sign of illness or an absolutely normal phenomenon.
The name "nystagmus" comes from the ancient Greek word νυσταγμός - drowsiness
. This is explained by the fact that in a dream the eyes also make involuntary movements.
This pathology is quite common: for example, according to statistics, congenital nystagmus is diagnosed in 20-40% of children with poor vision.
About physiological and pathological visual nystagmus, factors of its development, types, symptoms, signs of nystagmus and treatment methods - in our article.
Types of nystagmus
Experts distinguish physiological and pathological types of nystagmus.
Physiological nystagmus
A variant of the norm, the body’s response to a change in head position or external stimuli. Eye movement during physiological nystagmus is caused by reflexes.
Physiological nystagmus is divided into vestibular (labyrinthine) and optokinetic. As the name implies, vestibular nystagmus of the pupils appears due to irritation of the human vestibular apparatus: exposure to the structures of the labyrinth with current, low or high temperatures, as well as during rotation of the body along the vertical axis. In addition, the labyrinthine type of nystagmus can occur if a person looks away to the side as far as possible: the eye muscles quickly tire, causing characteristic twitching.
Optokinetic nystagmus occurs when a person watches objects moving in one direction at a constant speed. With such observation, the gaze is directed most of the time in the direction of movement, but sometimes it “jumps” to the opposite direction.
Pathological nystagmus
Pathological nystagmus is a sign of the development of a particular disease. It can be congenital or acquired.
Congenital nystagmus appears soon after the baby is born. Acquired - during life due to exposure to various pathological factors on the body. Acquired nystagmus is usually divided into vestibular and neurogenic, depending on the lesions in which area it is caused.
If we talk about differences in the direction of movements, we can distinguish vertical, horizontal and rotatory types of pathological nystagmus. With vertical, the eyeballs move up and down, with horizontal - along the sides, with rotatory - in a circle and diagonally. The most common of these is horizontal nystagmus (up to 18% of the total number of cases). The rarest ones are oblique and circular.
Directions of eyeball movement during nystagmus
According to clinical manifestations, pathological nystagmus is divided into:
- jerky. Eye movements with this type resemble rhythmic jolts, and if the eye moves quickly in the direction of the jolt, then in the opposite direction it moves more slowly. Push-like nystagmus can be left- or right-sided, depending on which direction the push is directed.
- pendulum-shaped. The eyeballs move like a pendulum, as if swinging in one direction or the other.
- mixed. This type of nystagmus combines both jerking and pendulum movements.
- associated. Characterized by coordinated movement of the eyeballs.
- dissociated - when the eyes move uncoordinated, not matching in direction and amplitude.
In addition, nystagmus can be installational - when there are short, insignificant amplitude twitches of the apples when looking to the side (the reason for this is most often a failure in muscle coordination), and spontaneous, which is characterized by longer, more pronounced “jumps”.
Conditions resembling nystagmus
Nystagmus may resemble eye movement disorders such as:
- convulsive twitching of the eyeballs with a characteristic rectangular signal (small jerky movements away from the point of fixation and back)
- trembling of the eyeballs (horizontal pulsating vibrations)
- opsoclonus (frequent saccadic oscillations)
- myokymia of the superior oblique muscle (monocular rotatory-vertical movements)
- ocular bobbing (ocular bobbing - rapid deviation of the eyeballs downward with a slow return to the top)
- periodic movements of the eyeballs in a horizontal direction with a change in the direction of deviation every few seconds
Visual disturbances and movements of the eyeballs are a signal of danger, the recognition of which greatly increases the knowledge of a neurologist and neurosurgeon. A neurologist or neurosurgeon who is alert to such visible signals that the eye can send will not only recognize and differentiate them from each other, but will also understand their clinical significance.
Reasons for the development of nystagmus
Anomalies of intrauterine development, trauma during childbirth, disorders - including genetic ones - of visual acuity, transparency of the media of the eyeball, changes in the fundus, pathological processes in the optic nerve, retinal dystrophy, albinism can cause congenital nystagmus.
The causes of acquired nystagmus include:
- brain diseases (oncological formations, strokes, multiple sclerosis);
- malfunctions of the vestibular apparatus;
- poisoning, intoxication (medicinal, narcotic, alcohol);
- head injuries (with damage to the occipital region, optic nerves);
- refractive errors (myopia, farsightedness);
- strabismus;
- diseases with impaired media transparency (mature cataract, etc.).
Diagnosis of nystagmus
For every child who is suspected of having a disease, diagnostics will help confirm or refute the diagnosis. But making this very diagnosis is not as simple as it seems. It was already mentioned above that the disease can be not only manifest, but also latent, which means that in some cases it is simply impossible to determine its presence without special diagnostic procedures.
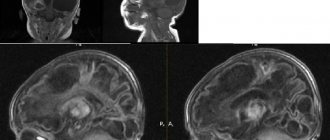
Among other studies, computer diagnostics, assessment of the state of the capabilities of the visual apparatus, and assessment of visual acuity indicators are carried out. In order to implement an integrated approach to the problem, the ophthalmologist invites a neurologist for a joint examination, and both doctors decide on the advisability of involving related specialists depending on the results of the examination. Diagnostics may include procedures such as electroencephalography, echo-encephalography, magnetic resonance imaging.
These studies are aimed at recording the biopotentials of the cortical visual analyzer, preserving the functional abilities of the optic nerve and visualizing the brain structures responsible at all stages for transmitting the visual impulse and regulating its processing.
Symptoms of nystagmus
In addition to a general decrease in visual acuity, patients with pathological nystagmus complain of:
- the feeling that the world around you is moving;
- difficulty fixing the gaze on the object in question, a feeling of trembling, image displacement;
- the appearance of neutral zones. Neutral zones are head positions in which eye movements are not so intense. Often a person begins to hold his head in a certain position so as not to feel the “jumping” so much.
Symptoms worsen under stress and fatigue.
Treatment of nystagmus
The treatment strategy directly depends on the severity of symptoms and specifically the forms of nystagmus. To treat nystagmus the following is used:
- Conservative therapy . It is used when clinical manifestations progress against the background of central vestibulopathy. The most commonly used are neurotropic drugs from the anticonvulsant group, as well as antiepileptic drugs.
- Surgical intervention . Surgical intervention is used to form eye positions relative to the resting point, by restoring the physiological position. To do this, the structural features of the extraocular muscles are influenced.
Symptomatic treatment is mainly aimed at spectacle or contact vision correction. Experts recommend the use of contact lenses, since when the eye moves, the lens moves synchronously with the eye.
In individual cases, Botox injections are performed into the orbital cavity to limit small and frequent eye movements.
Prognosis and prevention
With proper treatment and compliance with doctor's orders, the prognosis for the restoration of visual functions is very favorable. Corrective therapy of the underlying disease ensures elimination of the clinical manifestations of the pathology. But specific, preventative prevention has not currently been developed. Nonspecific preventive measures include timely diagnosis and treatment of brain pathologies, treatment of the vestibular system and, specifically, the organs of vision.
When detecting involuntary eye movements in a patient who has taken anticonvulsants or sleeping pills, it is necessary to adjust the dosage of the drugs.
Classification
Due to the cause of its appearance, nystagmus is divided into:
Physiological:
- installation,
- vestibular,
- optokinetic.
Pathological (spontaneous) nystagmus:
- fixation (ocular),
- professional,
- labyrinthine,
- neurogenic.
What is the difference between physiological and pathological nystagmus?
According to the time of appearance, this disease is divided into:
Congenital:
- optic,
- latent,
- sternocleidomatous
Acquired:
- central,
- peripheral.
There are also types divided according to the directions of movement of the eyeballs :
- Horizontal nystagmus - oscillatory movements from side to side;
- Vertical nystagmus - vertical oscillatory movements;
- Diagonal - diagonal oscillatory movements;
- Rotatory (rotational) - circular movements.
Types of nystagmus according to the nature of pupil movement
By nature of oscillations:
- pendulum movement;
- jerking movement;
- mixed.
According to the difference in vibrations in one or two eyes:
- Friendly (both eyes move the same way);
- Dissociated (movement varies);
- Monocular (nystagmic movement of one eye).
Also divided according to the amplitude of oscillations :
- Small-caliber (span - five degrees);
- Medium-caliber (span - from five to fifteen degrees);
- Large-caliber (span - above fifteen degrees).
Physiological
This type can appear in healthy people as a reaction to various nervous stimuli and has its own division:
Installation
These are short-term vibrations of the eyeball in the form of shocks, when looking at the extreme position in any direction (horizontally - 30 degrees, vertically - 20 degrees).
This type does not relate to pathologies of the vestibular apparatus, but appears when the motor muscles of the eye cannot cope with their work under strong tension.
Important! This type may foreshadow a chronic disease - dyscirculatory encephalopathy. The installation type of nystagmus itself does not need to be treated, but it is necessary to monitor its development; if it is present, be sure to mention it when examined by a doctor.
Installation nystagmus
Vestibular
Vestibular nystagmus manifests itself in the form of jerks when the vestibular apparatus is irritated when rotational or caloric stimulation occurs.
Rotational movements of the head and body cause angular acceleration, stimulating the semicircular canals. Caloric stimulation is the irritation of the inner ear when water enters it.
- If the vestibular apparatus is damaged, a rotatory type may occur.
- With pathology in the inner ear or brain, spontaneous nystagmus appears.
Optokinetic
This variety also consists of vibrations of the eyeballs in the form of tremors that appear when the eyes follow rapidly flashing objects. These movements are performed by both eyes at once at the same speed in the direction of the observed objects and are accompanied by rapid jumps of the pupils in the opposite direction.
Development of a method for treating congenital optical nystagmus and evaluation of its effectiveness
optic nystagmus and evaluation of it's efficacy VI Dolzhich, SV Yakovenko, IS Malyutina Rostov State Medical University “Eximer” clinic, Rostov-on-Don Purpose: to find the pathogenic basis of treatment method of congenital nystagmus and to evaluate it's efficacy. Materials and methods: 54 patients (108 eyes) with optic nystagmus at the age of 6-14 years old were examined. To evaluate ophthalmologic and neurophysiologic indices we took group of healthy children (n = 10) of the same age. Ophthalmologic examination included: visometry, refractometry with cycloplegia and usual accommodation tone, ophthalmometry, echo biometry, ophthalmoscopy and electrophysiological examination. Foe treatment of those patients we used instenon and glycin and also training in “Ambliocor”. Results: Refractometry showed the prevalence of hypermetropic refraction with astigmatic component. Electrophysiological data showed that the decrease in vision mainly depends on the decrease in functional activity of the central part of visual analyzer and pathways. It was found out that there is a decrease of vision in all children with congenital nystagmus (n = 108). After the treatment electrophysiological indices and visual acuity increased. Conclusion: Thus, the method of combined treatment of nystagmus not only allows to improve visual functions but also to reach improvement of cortical and subcortical relations, mental faculties and adaptation abilities of the child.
Congenital optical nystagmus has a complex pathogenesis and, as a rule, is accompanied by a significant decrease in vision. In schools for the visually impaired, children with congenital optical nystagmus make up from 20 to 40% in different regions of Russia [3,5]. Some authors consider amblyopia to be the direct mechanism of vision loss with optical nystagmus and recommend appropriate treatment [2,3,5]. Other authors point to the role of changes in cortical-subcortical relationships in the mechanism of vision loss in children with nystagmus [4,7]. Considering the medical and social significance of congenital optical nystagmus, caused by a decrease in professional adaptation, the quality of life of young patients, the development of new treatment methods and improving vision in this category of patients is an urgent task in neuro-ophthalmology. The purpose of this work was to provide a pathogenetic substantiation of the method of treating congenital optical nystagmus and to evaluate its effectiveness. Material and methods. 54 patients (108 eyes) aged 6 to 14 years with optical nystagmus were examined. To assess ophthalmological and neurophysiological parameters, a group of children (n = 10) of a similar age who were ophthalmologically and somatically healthy was examined. The ophthalmological examination included: visometry using standard methods with and without correction, refractometry under conditions of cycloplegia and habitual accommodation tone, ophthalmometry, echobiometry, and ophthalmoscopy. Electrophysiological studies: determination of the threshold of electrical sensitivity of the retina (RES), electrical lability of the optic nerve (EL); study of frequency-contrast sensitivity using the Zebra computer program using spatial gratings of various frequencies, achromatic and color gratings presented on a computer monitor; study of visual evoked cortical potentials (VECP). An in-depth study of the bioelectrical activity of the cerebral cortex was carried out by electroencephalography (EEG) with determination of the amplitude, index and frequency of the main groups of waves with localization of the maximum electrical activity of the alpha rhythm. Results and discussion. Ophthalmological examination methods showed that all children in the main group with congenital nystagmus (n = 108) had reduced visual acuity. Refractometry revealed a predominance of the frequency of hypermetropic refraction with an astigmatic component (Table 1). The data in Table 1 shows that in older children, visual acuity below 0.1 is 9.6% less common than in the younger age group. This is due to previous treatment, including neuroprotectors and vitamins. However, all patients in the main group had visual acuity no higher than 0.3 with correction. Biomicroscopically, the presence of signs of dysgenesis in the form of membrane persistens and embryotoxon was established in 30 eyes (27.8%). Optical media are transparent. Ophthalmoscopically, in 64.8% of cases, pallor of the optic nerve head was detected without signs of prominence, with unclear boundaries. In 35.2% of cases, the fundus was without pathology. In patients of the main group, the nystagmus was pendulum-shaped, of medium amplitude in 74% (80 eyes). In other cases - rotational. The study of electrophysiological parameters made it possible to establish a number of differences in patients with nystagmus compared with data from the control group (Table 2). The data in Table 2 show that the EC threshold in children with nystagmus is significantly higher by 5% in patients aged 6–9 years. In the older age group, the retinal EC threshold did not change significantly (p > 0.05). The EL threshold of the optic nerve was significantly reduced by 28% in young children with nystagmus and by 27.1% in older children. These data allow us to conclude that in congenital nystagmus, retinal electrogenesis is slightly reduced and suppression of conduction along the visual pathways to the cortical center predominates. The study of flashes and the pattern of PVCPs showed that in patients with optical nystagmus there is a depletion of the component composition of PVCPs, a significant and significant (p < 0.05) decrease in the amplitude of the P100 component to 6.3 ± 0.24 μV and a significant (p < 0.05) ) increase in latency to 127.0 ± 2.7 ms. In the control group, the P100 amplitude was 9.8 ± 0.18 μV, the latent period was 101.3 ± 0.58 ms. The P200 component is weakly expressed or absent altogether. Data analysis indicates a low degree of maturity of higher visual centers in children with optical nystagmus. When studying frequency-contrast sensitivity, there was a moderate decrease in the overall level of contrast sensitivity, a decrease or complete loss of the high-frequency region. In all patients, the shape of the curve differed from the norm. A decrease in sensitivity in the region of high spatial frequencies indicates damage to the visual analyzer at the level of the midbrain and cortex [4,6,7]. EEG data are of significant importance in the study of neurophysiological mechanisms in the pathogenesis of optical nystagmus in children. We have found that in children with nystagmus with low visual acuity, 2 types of electroencephalogram (EEG) are recorded, in contrast to the control group of the same age: 1) hypersynchronous EEG with a high irregular alpha rhythm with an amplitude of up to 100 μV and higher in combination with high amplitude slow waves and 2) disorganized EEG with a low irregular alpha rhythm with an amplitude of up to 30 μV and a predominance of slow waves - delta and theta. Both types of EEG confirm the presence of an immature cortex, its low bioelectrical activity with a predominance of activity in the diencephalic region in hypersynchronous EEG, which confirms the pathology of the central part of the visual analyzer in children and adolescents with optical nystagmus. Children in the control group aged 6 to 9 years were characterized by registration of an organized alpha rhythm with an amplitude of 50–58 μV (average 53.3 ± 0.62 μV) in combination with slow waves - delta and theta, the focus of maximum electrical activity was recorded in the occipital region. In children from 10 to 14 years old, slow waves were not detected on the EEG; the amplitude of the alpha rhythm was significantly (p < 0.05) higher than in younger children, averaging 58.1 ± 0.54 μV. The results obtained were typical for organized EEG. A comparative assessment of EPI data showed that in the mechanism of vision loss the leading role belongs to a decrease in the functional activity of the central part of the visual analyzer and pathways. In this regard, we have developed a complex treatment regimen aimed at correcting the identified changes. We chose the drugs instenon and glycine as the medicinal component. The choice of drugs is determined by their pharmacological action [8]. The drug instenon contains 50 mg etamivan, 20 mg hexobendine dihydrochloride, 60 mg etophylline. The combination of components provides an activating effect on the limbic and reticular formation of the brain stem, which leads to adequate functioning of the neural components of the cortex and subcortical-stem structures, mainly due to etamivan. Hexobendine, which is part of the drug, improves cerebral blood flow, stimulates neuronal metabolism, and restores synaptic connections. In this case, the absence of the so-called “steal syndrome” observed when prescribing other vasotropic drugs is very important. Etophylline – stimulates subcortical formations, centers of autonomic regulation. In children with optical nystagmus in combination with disorganized low-amplitude EEG, instenon causes a state of cortical activation. The drug glycine is a non-essential amino acid, a central mediator of inhibitory action; improves metabolic processes in brain tissue, increases mental performance. In children with optical nystagmus, in combination with hypersynchronous EEG, glycine causes a state of cortical relaxation. Treatment was carried out against the background of carefully selected spectacle or contact correction. In addition, the technology of the method for treating nystagmus additionally includes the Amblyokor - 01 hardware complex, which allows influencing the cortical part of the visual analyzer in the form of training the parameters of the bioelectrical activity of the cortical-subcortical parts of the visual analyzer in a given direction [1]. We propose that in patients with congenital optical nystagmus, set the mode on the Amblyokor - 01 hardware complex, taking into account the initial EEG. Treatment was carried out as follows: initially, an EEG is recorded on an electroencephalograph and, taking into account the amplitude of the alpha rhythm of the EEG, drug treatment is prescribed: in the presence of a disorganized low-amplitude EEG, when the amplitude of the alpha rhythm is below 30 μV or is not determined at all, instenon is prescribed per os, 1 tablet 2 times per day every day for 2 weeks, and when recording a high-amplitude hypersynchronous EEG with an alpha rhythm amplitude of 100 µV and above, glycine is prescribed 1 tablet 100 mg sublingually 2 times a day every day for 2 weeks, after which video training is carried out using the Amblyokor - 01 device 2 weeks, while continuing to take previously prescribed medications. The mode of influence depends on the EEG data: with a disorganized low-amplitude EEG, the mode is “relaxation”; with a high-amplitude hypersynchronous EEG, the mode is “activation”. Daily monitoring for 2 weeks promotes the development of a conditioned reflex aimed at correcting the bioenergetics of the cerebral cortex in a given direction, which is normalized by ongoing differentiated drug therapy aimed at strengthening in disorganized low-amplitude EEG and relaxation in high-amplitude hypersynchronous EEG. As a result of the treatment, there was an increase in visual acuity and an improvement in EPI parameters (Table 3). The data in Table 3 shows that after complex treatment, visual acuity increased to 0.4 - 0.5 in 20 - 22.9% of cases, and low visual acuity (below 0.1) increased to 0.1 - 0.2 in 21 .7% in the younger age group and 18.7% in the older age group. The pathogenetic orientation of the proposed method is confirmed by an improvement in the EL threshold of the optic nerve by 16.2% in the younger age group, by 17% in the older age group and EEG data. In 38 children (70.4%), when recording an EEG, organized alpha activity was noted with an increase in the amplitude of the alpha rhythm in the range of 54 - 56 μV, with the focus of maximum electrical activity localized in the occipital lobe of the cerebral cortex. Thus, the proposed method of increasing visual functions in children with optical nystagmus (application No. 2005132147/14), taking into account the characteristics of the initial EEG and its drug correction, allows, with the help of training on the Amblyokor - 01 hardware complex, not only to increase visual functions, but also achieve improvement of cortical-subcortical relationships, increase mental abilities and behavioral adaptation of a child with optical nystagmus, which in general can be described as improving the quality of life of this category of patients.
The article was accepted for publication on September 12, 2006.
Literature 1. Avdeeva A.A., Mikhailenok E.L., Moshetova L.K. Video-computer vision correction in the treatment of eye diseases // Methodological recommendations. RMAPO. – M., 2000. – P. 1 – 5. 2. Avetisov E.S., Smolyaninova I.L., Shapovalov. S.L. and others. New possibilities for improving visual functions with nystagmus // Vestn. ophthalmol. – 1979. – No. 3. – P. 26 – 32. 3. Avetisov E.S. System of measures to improve visual functions with nystagmus // Methodological recommendations of the Moscow Research Institute of Eye Diseases named after. Helmholtz. – M., 1980. – P. 13. 4. Dolzhich G.I., Shcherbakova E.M. The role of neurophysiological mechanisms in the pathogenesis of optical nystagmus // Vestn. ophthalmol. – 2002. – T. 118, No. 6. – P. 19 – 21. 5. Proskurina O. V. Accommodative ability of the eyes in patients with optical nystagmus and the possibility of its restoration: Dis. E cand. honey. Sci. – M., 1994. – 178 p. 6. Shelepin Yu.B., Kolesnikova L.N., Levkovich Yu.I. Visocontrastometry. Measuring spatial transfer functions of the visual system. – L.: Nauka, 1985. 7. Shcherbakova E.M. The state of visual functions in children with optical nystagmus, taking into account neurophysiological characteristics: Dis. E cand. honey. Sci. – R., 2000. – 111 p. 8. Register of Medicines of Russia. - Doctor. M., – 1999. – P.342, 448.
Acquired
This is a pathology of the oculomotor system, which can manifest itself at any age, with:
- various injuries, disorders and tumors in the brain.
- alcohol and drug addiction;
- excess of drugs in the body.
The acquired appearance is divided into the following types:
Central
Occurs with serious damage to the central nervous system:
- various malignant formations;
- stroke;
- damage to the cerebellum or brain stem.
In its background there may be:
- dizziness;
- pain in the head;
- flashes in the eyes;
- different pupil sizes.
Peripheral (vestibular)
Acquired pathological peripheral nystagmus is spontaneous and manifests itself in cases of lesions of the vestibular apparatus. Physiological vestibular nystagmus is a reflex of a healthy person.
Signs:
- horizontal;
- accompanied by dizziness and nausea;
- the patient may not hear and lose balance.
It lasts for a few days and then goes away. Vestibular nystagmus manifests itself only when one of the two vestibular nuclei is affected; if both are affected, there is no vibration of the eyeballs.
↑ Spasmus nutans
The nature of the disturbances in head and eye movements in this disorder resembles those in neurogenic nystagmus and atypical VIN.
The diagnosis is made retrospectively; imitation of this condition by a number of diseases, in particular nystagmus in chiasmal glioma, cannot be ruled out. The disorder appears at an early age (from 1 month to 2 years) and disappears spontaneously.
- Asymmetrical pendular nystagmus. Nystagmus in one eye may have a greater amplitude and even a different direction compared to the other eye. This is usually the first symptom that parents notice.
- Shaking head. It can have a horizontal, vertical or complex direction; there are often pauses in movements.
- Forced position of the head.
To clarify the diagnosis, a neurological examination is necessary, and a CT scan may be required.
Causes
Unstable eye movements can appear in a person both from the first days of life and in adulthood. The reasons for this are as follows:
- Genetic predisposition (occurs with hereditary diseases: Leber's amaurosis, partial albinism);
- Consequences of unfavorable birth, premature birth, trauma at birth;
- Various injuries and diseases of the brain: injuries, tumors, disruptions in the blood circulation of the brain, Arnold-Chiari malformation, hydrocephalus, various lesions of the myelin component of the brain and spinal cord, which controls rapid transmission along nerve fibers.
- Disorders of the vestibular system: internal otitis, acute vestibular dysfunction, benign tumor - neuroma.
- Various severe refractive errors (myopia, hypermetropia, astigmatism). If this disorder is corrected, the disease usually stops.
- Poisoning with drugs (barbiturates, benzodiazepines), drugs, alcoholic beverages.
Childhood nystagmus
As a rule, childhood nystagmus does not appear immediately. The fact is that a newborn baby’s eyes cannot yet focus, so instability in the position of the eyeballs cannot be classified as nystagmus. If by the age of one month the child does not fix his gaze, for example, on a bright toy, a specialist may advise diagnosing the presence of nystagmus.
Up to a year of age, ophthalmologists and neurologists only observe the presence of eye fluctuations, since they can be temporary and go away when the child grows up. Treatment of nystagmus in children is prescribed only with an accurate diagnosis.
Medicines
Photo: slavikap.livejournal.com
Neurotropic drugs are divided into two main groups:
- Drugs that affect afferent innervation, through which nerve impulses are transmitted from internal organs and tissues to the central nervous system;
- Means that affect efferent innervation, through which excitation is transmitted from the central nervous system to internal organs and tissues.
The choice of a specific drug depends on the form of nystagmus and the cause of its occurrence.
Vasodilators include drugs whose mechanism of action is to relax the smooth muscles of blood vessels, which leads to the expansion of their lumen. Myotropic drugs act directly on the muscular elements of the vascular wall. Neurotropic drugs achieve a vasodilating effect due to their influence on the nervous regulation of blood vessel tone.
Vitamin-mineral complexes contain all the vitamins and minerals necessary for the normal functioning of the body. When choosing a vitamin-mineral complex, it is worth considering the gender, age and health status of the patient.