A pathological condition that is accompanied by a decrease in the size, volume and weight of an entire organ or its individual sections with a gradual cessation of functioning is called atrophy.
This disease can affect various organs and tissues, in particular muscles, brain, limbs, retina, and skin. Atrophy can develop as a result of disease and also as part of the natural aging process. In this regard, senile and pathological atrophy are distinguished.
Classification of jaw atrophy and bone tissue phenotypes
Depending on the position of the jaw, there are two groups that characterize the atrophic state of the upper and lower jaws:
- According to Schroeder for the top row. There are three types of upper jaws with missing teeth, resulting in thinning bone tissue:
- The jaw tubercles are very noticeable. These gaps can be filled with prosthetic implants because the physical abnormalities are not noticeable. The palate is deep, and the bend of the mucosa is quite large.
- The alveolar processes are not clearly defined. The depth of the sky is average. Prosthetics are possible, but their fixation may deteriorate after muscle tissue overstrain.
- The bone at the base of the jaw is seriously destroyed. The ridges and tubercles of the alveoli are smooth, and the palate is transformed into a flat shape. The fold of the mucous membrane becomes at the level of the palate and does not hold its shape well. As a result of pathology, prosthetic structures cannot be secured.
- According to Keller for the bottom row:
- The alveolar elements are slightly smoothed, but are visible throughout the entire jaw. At the beginning of the alveolar ridge, muscle tissue and a fold of mucous membrane are attached. Installation of the prosthesis is not difficult.
- The ridge becomes noticeable and takes on a sharper shape. The muscles are attached to the crest. In most cases, the implant causes discomfort and pain.
- It is often observed in people who have undergone early removal of lateral teeth. The alveoli around the molars and premolars become thinner. In the central part, the bone tissue does not lose volume. Creating artificial teeth is possible, but there is a possibility of the implant slipping when chewing.
- In the area of the frontal incisors, a pronounced atrophic process is observed, while the lateral dentition remains preserved. Fixation of the prosthesis cannot be done, because the likelihood of its displacement increases.
Treatment
It is necessary to begin treatment by eliminating the underlying disease that provoked the appearance of the atrophic process. If sclerotic lesions and atrophy are not very advanced, it is possible to fully or partially restore the functions and structures of the affected organ or part thereof. However, deep atrophic lesions cannot be treated or corrected.
The specifics of treatment are influenced by the severity, form, duration of the disease, as well as the patient’s age and individual tolerance to medications. In each case, the doctor selects treatment methods individually. As a rule, long-term medication, physiotherapy and symptomatic treatment are prescribed. The course of treatment should not be interrupted and should be repeated regularly, taking into account the recommendations of the attending physician.
Implantation for jaw bone atrophy
Several techniques are used to quickly restore the dentition. For example, installation of bridges or removable dentures. However, these methods cannot restore the required load on the bone, since the gums or healthy teeth are loaded.
Implantation helps relieve pressure on the bone and prevent further thinning.
In advanced cases, when the atrophy of the jaw bone tissue is significant, restoration of the bone structure is used before implantation. Various techniques are used, for example, sinus lifting, separation of the alveolar process, and the introduction of artificial tissue. Six months after the operation, implants are inserted. As a result, bone density and volume are preserved.
Implantation with immediate loading is considered a new technique. Special materials are installed not in the alveolar process, but in the basal part of the jaw. Thanks to this, the bone is immediately loaded, and the metabolism is not disrupted. Suitable only if three or more teeth in a row are missing.
1.General information
Neurodegenerative diseases remain one of the most acute, pressing, and to this day far from being solved problems in neurology. This term combines pathological processes with the development of which the “working” tissue of the central and/or peripheral nervous system degenerates, loses its original structure, decreases in volume and gradually dies (respectively, degeneration, atrophy, necrosis). Normally, such tissue is formed by neurons (nerve cells), their processes (axons and dendrites) and a complex cross network of points of electrochemical contact between them (synapses). Several regulatory systems function in the human body; To put it simply, we can say that hormones control the functioning of internal organs, enzymes are responsible for processing nutrients, etc., but the highest level of control of all processes occurring in the body belongs to neural tissue. This becomes most obvious in the example of the phenomenon that we are accustomed to call the crown of evolution - the human psyche, including such phenomena as consciousness and abstract thinking. However, the “sphere of responsibility” of biological neural networks is by no means limited to the higher functions of the cerebral cortex. And the activity of the endocrine glands, and the coordination of motor (motor) acts, and the entire vast spectrum of sensations available to humans, and a huge number of unconditional, independent of consciousness reflexes - ensuring optimal automatic response and, accordingly, survival in the surrounding world - are controlled and controlled by the brain and spinal cord (CNS) and relatively autonomous peripheral neural ganglia. Therefore, degeneration and atrophy of neural tissue in any area is a process that is always catastrophic for the body.
Neurodegenerative diseases are characterized by a relatively slow pace of development (5-20 years) and towards the terminal stage, as a rule, are accompanied by total dementia - loss of intelligence, memory, personality, basic skills, contact with others. The insurmountable complexity of such diseases today is that some of them are hereditary, chromosomal in nature; others are polyetiological processes, i.e. In all likelihood, many factors are simultaneously involved in their “launch” and development, and not all of them have been identified and studied to date. The most well-known and widespread neurodegenerative processes include Alzheimer’s, Pick’s, Parkinson’s diseases, corticobasal degeneration, etc.
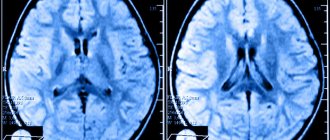
This same group of diseases includes a rare pathology characterized by degeneration of brain neurons in those zones and on such a scale that simultaneously affects several functional systems of the body, which is emphasized by the diagnostic term “multiple system atrophy” (orally “Shay-Drager syndrome” ). The disease is widespread in the world at a level of about 5 people per 100,000 population. In contrast to the similar diseases listed above, which are traditionally (and not entirely correctly) perceived as purely “senile”, multiple system atrophy is diagnosed in people over 50 years of age in only a little more than half of the cases; the other half falls on other age categories.
A must read! Help with treatment and hospitalization!
Types and degrees of jaw bone atrophy
Deformation of the jaw bone develops with different intensity:
- I degree. At the beginning of the disease, it is eliminated by prosthetics. The implant performs its function, the blood supply is not disrupted.
- II degree. The clinical picture is intensifying. The mucous membrane of the jaw begins to shrink. Dental prosthetics are possible, but additional treatment is required before this can be done.
- III degree. The contour of the bone tissue is smoothed both on the inside of the mouth and on the side of the chin.
When selecting a treatment method, this characteristic of the development of pathology should be taken into account. Bone tissue decreases not only in height, but also in width. The bone becomes short and thin.
What is vaginal atrophy?
Vaginal atrophy (also called atrophic vaginitis or colpitis) is a condition in which the vaginal lining becomes drier and thinner. Most often occurs during menopause, a “lifestyle change” due to a decrease in the level of the hormone estrogen. Hormones are produced, stored and secreted by the endocrine system, a network of glands and organs. Women need estrogens for good health, especially during childbearing years. When menopause occurs around age 50, the ovaries produce fewer hormones and the woman stops having periods. But the condition of vaginal atrophy also occurs in young women when their estrogen levels are disturbed.
The mechanism of development of atrophic changes in the walls of the vagina
The vaginal mucosa is a stratified squamous epithelium, which before menopause is moist and thick with wrinkles. During menopause, when estrogen levels decrease, this epithelium becomes thinner. Fewer epithelial cells result in less cell shedding in the vagina (see diagram). When epithelial cells slough off and die, they release glycogen, which is hydrolyzed to glucose. Glucose, in turn, is broken down into lactic acid by lactobacilli, normal inhabitants of a healthy vagina. Without this cascade, vaginal pH rises, leading to loss of lactobacilli and overgrowth of other bacteria, including group B streptococci, staphylococci, coliforms, and diphtheroids. These bacteria can cause symptomatic vaginal infections and inflammation. This results in itching, burning and pain during sex, among other symptoms, and includes urinary tract infections (UTIs) and frequent urination. Recently, the term “vaginal atrophy” has been proposed to be replaced by the new term “genitourinary menopausal syndrome.” It involves not only vaginal but also urinary symptoms, which can be caused by low estrogen.
Who is at risk for vulvovaginal atrophy?
Women aged 50 years and older during menopause are most susceptible to vaginal atrophy. Other reasons that increase your likelihood of developing it include:
- Lack of sexual intercourse.
- Decreased ovarian function due to chemotherapy or radiation.
- Immune disorders.
- Medicines with antiestrogenic properties.
- Ovariectomy (removal of the ovaries).
- Postpartum estrogen loss.
- Breast-feeding.
Causes of atrophy
During menopause, your body produces less estrogen. Without estrogen, the lining of your intimate area may become thinner and less elastic. The vaginal canal may also narrow and shorten. Low amounts of estrogen reduce the amount of normal vaginal fluids. It also changes vulvovaginal acid balance.
Women who have just given birth and are breastfeeding also experience a decrease in estrogen levels. These symptoms also occur in patients who have had their ovaries removed or who are taking certain medications (such as aromatase inhibitors for breast cancer). And the first sign of mucosal atrophy is usually insufficient vaginal moisture.
Risk factors
There are two main factors that can increase your chances of vaginal atrophy:
- Smoking. It restricts blood flow, including in the vaginal area. Also reduces the natural amount of estrogen in your body.
- No vaginal birth. Those who have not had a vaginal birth are more likely to have these problems than those who have.
Clinical manifestations
Symptoms of vaginal wall atrophy may include:
- Vaginal dryness.
- Burning and/or itching in the vagina.
- Dyspareunia (pain during sex).
- Vaginal discharge is usually yellow in color.
- Spotting and spotting
- Bleeding from the vagina after sex.
- Itching of the vulva (desire to scratch between the legs).
- Feeling of pressure in the perineum.
Signs of atrophic changes in the urinary tract:
- Desire to wash yourself more often.
- Pain when going to the toilet.
- Urinary tract infections (UTIs).
- More acts of urination.
- Stress urinary incontinence.
- Painful urination (dysuria).
- Blood in the urine (hematuria).
- Burning when urinating.
The first symptom is usually a lack of lubrication during intercourse. Over time, persistent vaginal dryness may occur. Thinning of the epithelial lining can also cause itching, tenderness, and stinging pain in the vaginal and vulvar areas, which in turn can further contribute to dyspareunia. Spotting may also occur due to small tears in the vaginal epithelium. Women with genitourinary menopause syndrome may report a thin yellow or gray watery discharge without much itching or odor.
Photo 1. Microphotographs of superficial and intermediate cells (left) and atrophic cells (right). (Pap test, original magnification x20).
Photo of a normal smear and with atrophy of the vaginal mucosa
Diagnostic methods
A gynecologist can diagnose vaginal atrophy based on symptoms and a gynecological examination, which will show what the vagina looks like. This will help you know if you have reached menopause. Classic signs of vulvulvaginal atrophy during a pelvic examination include:
• Shortened or narrowed vagina. • Dryness, redness and swelling. • Loss of skin elasticity. • Whitish discoloration of the mucous membrane. • Rare pubic hair. • Bulge along the back wall of the vagina. • Skin diseases of the vulva (dermatoses). • Lesions of the vulva and/or redness of the vulva (erythema). • Bladder sagging in the vagina. • Changes in the external urethral meatus. • Minor cracks (tears) at the vaginal opening.
What tests need to be taken:
- Oncocytology of the cervix.
- General urine analysis.
- Ultrasound of the pelvic organs.
- Serum hormone test.
- Vaginal pH test.
- Microscopy for flora (see the entire catalog of analyzes).
Table 1. “Difference between vulvovaginal atrophy and other pathology of the intimate area.”
| Lichen planus | Painful red plaques or erosions, sometimes with white lacy edges or purple edges; may spread to the vagina |
| Lichen sclerosus of the vulva | Hypopigmented, wrinkled, wax-like tissue with confluent ivory and pink plaques, often in a butterfly or figure-eight pattern, enclosing the labia majora, minora and clitoral hood and extending around the anus; may lead to labial agglutination |
| Contact dermatitis | Redness, swelling and itching, sometimes with blistering and painful bright red swelling |
| Lichen simplex chronicus (hyperkeratosis) | Thick, lichen-like skin, often erythematous, caused by prolonged rubbing or scratching |
| Intraepithelial neoplasm of the vulva | Red, white or dark raised or eroded lesions, multifocal |
| Vulvar cancer | More often it is an ulcer with a raised or thickened edge |
| Extramammary Paget's disease | Brick-red scaly eczematoid plaque with a sharply defined border and sometimes rough surface |
Jaw bone atrophy with age
One of the factors influencing the defect is age-related changes. As a rule, in patients over 60 years of age, atrophy is a common process. This is explained by the fact that the lack of minerals and cell nutrition affects metabolism and teeth fall out. The blood supply to bone tissue is disrupted and the required amount of oxygen is not supplied. This causes a change in pressure on the bone.
Causes
Atrophy is an acquired process in which tissues and organs dry out.
For general atrophy, the provoking factors are:
- oncological diseases;
- lack of nutrients;
- hypothalamic lesions;
- infectious diseases that occur over a long period of time;
- endocrine disorders.
The causes of local atrophy include:
- radiation exposure;
- pressure on an organ or part thereof;
- stress on muscles, limitation of physical activity;
- severe intoxication of the body due to serious infections;
- long-term use of hormonal drugs;
- innervation;
- circulatory disorders due to ischemic lesions of arteries and veins;
- heredity;
- dyshormonal disorders.
Jaw bone atrophy after tooth extraction
The most common cause of the disease is the loss of a tooth or dentition. A few months after extraction, if prosthetics are untimely, the process of reducing the jawbone begins due to pressure on the alveolar process. Within a year, the deformation can reach its maximum.
The consequences of bone tissue deficiency are expressed in the deterioration of speech, changes in the proportions of the face and its shape, and the appearance of severe wrinkles in the mouth area. At an advanced stage, patients experience displacement of the dentition, loss of opposite and/or adjacent teeth. Because of this, the likelihood of implantation failure increases.
Diagnostics
In each specific case, diagnostic measures vary. At the initial stage, for any type of atrophy, the attending physician prescribes a physical examination, including anamnesis, palpation, visual examination and other procedures. In all cases, laboratory testing is necessary. Subsequent diagnosis is different. For example, to detect organ atrophy, ultrasound diagnostics, MRI or CT, radiography, scintigraphy, fibrogastroduodenoscopy and other procedures are performed. The main diagnosis of muscle atrophy is biopsy and electromyography. Laboratory diagnostics consists of assessing certain indicators in biochemical and general blood tests.