General information
Motor disorders are a symptom that accompanies various neurological diseases. They are associated with damage to the motor departments of both the central and peripheral nervous systems, which leads to partial or complete impairment of movements. Paresis is a limitation of movement and a decrease in muscle strength. A more severe form is paralysis (or plegia), in which voluntary movements are completely absent.
We can say that motor excitation is transmitted along a “two-story” cortical-muscular pathway - from the brain to the muscles (pyramidal pathway). The top floor is the brain, from where the impulse is transmitted to the spinal cord. If this motor pathway is disrupted, central paralysis or paresis develops. Central movement disorders are characterized by weakness in the arms or legs, increased reflexes, and the gradual development of spasticity.
The lower level of the pathway includes the spinal cord, from which the impulse is transmitted to the nerves in the periphery, which provide muscle movement. If this motor pathway is disrupted, peripheral paralysis or paresis develops. Peripheral paresis and paralysis are sluggish due to developing muscle hypotonia and occur with muscle weakness and atrophy. Thus, motor disorders can be caused by lesions not only of the brain, but also of the spinal cord, as well as peripheral nerves, which for some reason stop transmitting impulses from the brain to the muscles. Central paralysis is characterized by muscle spasticity - muscle tension that occurs involuntarily. Spasticity is characteristic of cerebral palsy, multiple sclerosis , encephalomyelitis , traumatic brain injury , and stroke . Code for spastic paraparesis according to ICD 10 - G82.1
Prof. Dr. Jörg Müller
Neurology – Parkinson's, MS
Head of the Department of Neurology
Specialization
- Recognized international expert in Parkinson's disease, dystonia and tremor
- Neuromuscular diseases
- Multiple sclerosis
- Treatment using butolotoxin (dystonia, spasticity)
- Deep brain stimulation treatment
- Author of more than 70 scientific publications, is a member of international expert councils
Show doctor's personal profile
Pathogenesis
If we consider acquired motor disorders in trauma, then at the moment of exposure to traumatic force, direct damage to brain tissue develops. Compression, contusion of the parenchyma and circulatory disorders occur in it. The outcome of these pathological changes is necrosis , developing in the brain or spinal cord. At the same time, the mechanism of secondary damage is triggered - ischemia and inflammation. The necrotic focus gradually turns into a connective tissue scar, which is surrounded by post-traumatic cysts.
The consequences of brain damage are interruption of pathways at different levels, associated with necrosis and atrophy . With a spinal cord injury, control of the muscles innervated by segments below the level of injury is lost. The possibility of functional restoration depends on the restoration of conduction along the spinal cord. If the conductivity of the spinal cord is completely disrupted when it is interrupted, automation develops in those sections that are located below the interruption. In case of partial disruption of conductivity, there is the possibility of slow restoration of functions after elimination of edema , inflammation and circulatory disorders due to the remaining fibers.
The pathogenesis of cerebral palsy is different. Birth trauma is thought to result in asphyxia and brain damage. However, as a cause of cerebral palsy, birth trauma matters only in 5-10%. There are other and more significant mechanisms for the development of the disease: impaired brain formation, intrauterine damage to neurons, diseases that occur in the first week of life. Brain damage (ischemia or trauma) before the child’s age of three, which also causes motor disorders, cannot be ruled out.
Prof. Dr. Bettina Schmitz
Neurology – Epilepsy
Head of the Department of Neurology
Specialization
- Epilepsy
- Differential diagnosis of non-epileptic paroxysms
- Long-term EEG - video monitoring
- Medical and non-medical care for paroxysms and complications associated with epilepsy
- Member of the British Medical Association
- Instructor and member of the European Academy for the Study of Epilepsy (EUREPA)
- Member of the Commission on Psychobiology and the International League Against Epilepsy (ILAE)
- Psychoorganic syndrome, World Federation of Societies of Biological Psychiatry (WFSBP)
- Video consultation
Show doctor's personal profile
Classification
The following types of movement disorders are distinguished depending on their prevalence:
- Monoparesis (monoplegia) is muscle weakness or loss of movement in one limb and on one side.
- Paraparesis (paraplegia) is muscle weakness or loss of movement in two limbs (or both arms or both legs). Depending on this, in neurology there is paraparesis of the lower extremities or paraplegia of the lower extremities and, accordingly, paraparesis or paraplegia of the upper extremities (synonyms lower paraparesis/plegia and upper paraparesis/plegia).
- Hemiparesis (hemiplegia) is muscle weakness or loss of movement in the upper and lower limbs, but on one side. That is, hemiparesis and hemiplegia can be right-sided or left-sided.
- Diplegia is damage to both halves of the body.
- Triparesis (triplegia) is a disorder of movement of three limbs.
- Tetraparesis (tetraplegia) – in case of movement disorders in four limbs.
According to the level of damage to the nervous system, movement disorders are divided into:
- Peripheral.
- Central.
- Mixed.
According to the degree of severity, movement disorders are:
- Mild degree.
- Moderate.
- Deep.
- Complete paralysis.
According to muscle condition:
- Spastic paralysis (paresis) is a pathological muscle tension with weakness of movements that develops in the arm or leg.
- Flaccid paralysis (paresis) is a pronounced relaxation of the muscles, but their shortening does not occur. When peripheral motor neurons are damaged, peripheral paralysis develops - they are called flaccid paralysis.
The spastic form of paralysis with increased muscle tone indicates damage to the central motor neurons. Spasticity occurs in many diseases of the central nervous system: stroke , encephalitis , Strumpel's disease , traumatic brain injury , cerebral palsy, multiple sclerosis , spinal injury , brain tumors and , amyotrophic lateral sclerosis . Acute damage to central neurons first manifests as flaccid paralysis, and then increased muscle tone. Thus, with strokes, motor impairments of varying degrees develop and, along with a decrease in strength, muscle tone changes towards spasticity. Post-stroke spasticity develops in 68% of patients, affecting the arm and leg.
With spinal injury , multiple sclerosis and spinal stroke, lower spastic paraparesis appears. In multiple sclerosis and cerebral palsy, spasticity is accompanied by muscle pain and the development of contractures.
Spastic diplegia is a common form of cerebral palsy, the clinical picture of which is tetraparesis - all limbs are affected, but the legs are predominant. Movement disorders can vary from awkward movements in the limbs to severe paresis.
Spastic diplegia is called Little's disease . Identified in premature infants with intraventricular hemorrhage or leukomalacia . In mild cases of the disease, symptoms appear by six months, and in more severe cases, tetraparesis is noticeable from birth. With this pathology, children begin to sit up late, and when walking they make “dancing” movements, their legs cross and there is emphasis (on their toes). In children, bone growth is disrupted, spinal curvatures and joint contractures develop very early. This disease causes speech delay and speech impairment. There may be pathology of the cranial nerves, which manifests itself in strabismus and atrophy of the optic nerves , as well as hearing impairment.
Tetraplegia is associated with more severe damage to the cerebral hemispheres, brainstem, or cervical spinal cord. May be associated with congenital (cerebral palsy) or acquired diseases. Acquired forms develop after severe traumatic brain injury, hemorrhage, as a result of tumors of the brain or spinal cord, encephalitis, or complications of neurosurgical operations. Flaccid tetraparesis occurs with muscle weakness in the arms and legs. spastic tetraparesis develops (double hemiparesis or double hemiplegia), which in children is considered a form of cerebral palsy. Patients have constantly increased muscle tone and cannot relax them. Without treatment, complete loss of movement and motor skills occurs. Increased spasticity is accompanied by muscle pain. Spasticity is also noted in the neck and tongue, so such children cannot speak (the tongue does not obey them). There is also mental retardation.
Strumpel's disease
Strumpel's spastic paraplegia is a hereditary disease that is caused by degenerative changes in the motor neurons of the spinal cord. Motor neurons enter the pyramidal tract, which begins in the cerebral cortex and ends with mononeurons in the spinal cord. Wikipedia clarifies that a feature of the disease is progressive spasticity and gait disturbance. For an unknown reason, the transport of proteins and lipids, which are necessary to maintain the structure of the cell, is disrupted in motor neuron cells. This disease is not a form of cerebral palsy, although it manifests itself as spastic diplegia .
The initial signs of Strumpel's disease appear at 10-15 years of age, but there are cases of the disease developing from early childhood. Characteristically symmetrical lesions of the legs. Patients are concerned about fatigue and stiffness in the legs, which appear after long walking or intense exercise. The leading cause is muscle spasticity and increased tendon reflexes. An increase in muscle tone causes the symptom of “crossed legs”, protective reflexes and bending of the legs at night appear. The later the disease appears, the more pronounced the spasticity and increased reflexes. Tendon contractures also develop (more so in the ankle joints). As the disease progresses, in the advanced stage, patients have difficulty walking, stumble and fall. There are no trophic disorders in the muscles (no atrophy), and there are also no dysfunctions of the pelvic organs.
Causes
Most movement disorders are caused by degenerative diseases, either congenital or acquired.
Paraparesis in adults and its causes
If congenital diseases ( adrenoleukodystorophy , which occurs with myeloneuropathy , Strumpel's disease ) and cerebral palsy are excluded, then most often paraparesis of the lower extremities is caused in adults by the following pathologies and conditions:
- Compression lesions (prolapsed intervertebral hernia , bone spines, thickened spinal ligaments that narrow the spinal canal and compress the spinal cord).
- Hepatic encephalopathy , in which spastic paraparesis is associated with the toxic effects of endotoxins.
- Injury to the spine and spinal cord, which leads to loss of movement and dysfunction of the pelvic organs. Spinal cord injuries very often lead to significant motor impairment and disability in patients.
- Tumors of the spinal cord.
- Infectious diseases ( encephalitis , Lyme disease , AIDS, neurosyphilis ).
- Autoimmune diseases ( systemic lupus erythematosus ).
- Epidural abscess.
- Vascular pathology of the spinal cord (epidural and subdural hemorrhages, blockage of the anterior spinal artery).
- Poisoning (medicines and alcohol).
Causes of central paresis:
- Traumatic brain injuries.
- Intervertebral hernia.
- Cerebral palsy.
- Strokes.
- Spinal cord injuries.
- Tumors (brain and spinal cord).
- Amyotrophic lateral sclerosis.
- Multiple sclerosis.
Symptoms and diagnosis of Strumpel's disease
Features of the clinical picture of the disease largely depend on the age at which its development began. Clinical signs primarily affect the lower extremities and worsen as they progress, up to complete loss of the ability to walk.
Among the most common and characteristic symptoms of Shtrumpel's disease, experts include:
- feeling of stiffness in the legs;
- increased muscle tone of the lower extremities;
- unsteadiness of gait;
- frequent falls;
- hyperreflexia of both legs;
- decreased muscle strength in the lower extremities;
- in the later stages of progression, muscle atrophy occurs;
- With the early onset of the disease, the child walks on tiptoes or lags behind peers in terms of developing walking skills.
In the diagnostic process, special attention is paid to the features of the clinical picture, the age at which the disease began, data from a general examination and the patient’s family history.
To make an accurate diagnosis and develop effective treatment tactics, our doctors perform a number of important studies:
- general clinical blood and urine tests;
- biochemical blood test;
- molecular genetic studies;
- magnetic resonance imaging of the spinal column in two projections;
- electroneuromyography;
- Evoked Potential Study.
It is also important to differentiate Strumpel’s disease from a number of other pathologies, including spinal cord tumors, amyotrophic lateral sclerosis, neurosyphilis and others.
Symptoms
Let's look at common motor dysfunctions.
Spastic diplegia
The most common form of cerebral palsy. The clinical picture shows spastic tetraparesis, that is, the function of the arms and legs is impaired, but the lower extremities are more affected. Patients have increased tone not only of the muscles of the arms and legs, but also of the body, as well as the tongue. Small children cannot sit or walk. The majority have pseudobulbar syndrome - articulation (articulate pronunciation), phonation (sound production), swallowing and chewing suffer. This form may be complicated by convulsive syndrome. Pathological attitudes are noted and a spastic gait with a cross is formed. Due to muscle tension, the patient has difficulty bending his legs at the knee joints and does not lift his legs off the floor.
Patients develop early deformities of the arms and legs, contractures , and curvature of the spine . High muscle tone causes pathological attitudes - crossing the legs and bending the knee joints. Characteristic poses develop: the triple flexion pose and the ballerina pose.
Children's intelligence is normal or reduced, and there may be hearing impairment. The degree of increased tone varies from mild to severe. Depending on this, some patients can walk independently, others with support, and others need to move in a wheelchair.
Spastic hemiparesis
With this form, the movements of the arms and legs on any one side of the body deteriorate. In the clinic it can manifest itself as left- or right-sided hemiparesis . At the same time, its expression is greater in the hand. This form is characterized by the fact that spasticity is more pronounced in the leg extensors and arm flexors. Therefore, the affected arm is bent at the elbow and brought to the body, the hand and fingers are also bent (the expression “the hand asks”) is used.
If we talk about cerebral palsy, then from birth the baby has a difference in movements in the arm and leg on the affected and healthy half. Limbs with paresis lag behind healthy ones in growth—the difference in their length is noticeable. The standing posture becomes incorrect and the foot is placed “on its toes”. Shortening the limb leads to poor posture and pelvic distortion.
When a child begins to walk confidently, he develops a hemiparetic gait. When walking, he “circles” a circle with the affected leg: it is extended at the knee joint and performs circular movements outward, and the torso deviates in the opposite direction. This bent position of the arm and leg, which makes circular movements when walking, is called Wernicke-Mann pose .
Hemiparetic gait occurs with lesions of the brain and spinal cord: strokes , abscesses , encephalitis , brain trauma , tumors , toxic injuries and hereditary degenerative processes. In patients, the muscles on the affected side are dense to the touch and their relief is sharply contoured. If several passive movements are performed in a limb in a row, then muscle tension decreases. When examining a patient, a “jackknife” symptom is often encountered - with passive movement in the elbow or knee joint, the patient feels muscle resistance, and then it decreases.
Inferior flaccid paraparesis
This form of motor dysfunction is associated with damage to peripheral neurons and is characterized by:
- decreased or complete loss of muscle tone;
- amyotrophy;
- degeneration of nerves;
- decrease or disappearance of reflexes;
- muscle degeneration.
Acute flaccid paresis was previously associated with polio , but after vaccines were created more than 50 years ago and thanks to mass immunization, the territory of the Russian Federation has been considered a polio-free zone since 2002. This movement disorder can be associated with many other causes and occurs as a symptom in many diseases:
- infectious lesions of peripheral nerves ( myelitis , polyneuropathy , mononeuropathy );
- traumatic neuropathies ;
- encephalomyelitis;
- spinal cord tumors in the thoracic spine;
- spinal cord injury in the cauda equina region;
- demyelinating diseases of the central nervous system;
- transient circulatory disorders of the spinal cord;
- botulism;
- hereditary metabolic diseases (HBD);
- heavy metal poisoning;
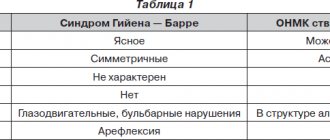
- Guillain-Barré syndrome (acute idiopathic polyneuritis - an autoimmune disease);
- toxic effect of drugs ( vincristine , isoniazid );
- the effect of muscle relaxants ;
- myasthenia gravis;
- botulism.
Patients initially develop weakness in the leg muscles, which progresses, and the patient cannot stand or move independently. Movement with great physical stress is possible only with the help of strangers or crutches. Patients cannot maintain an upright posture if their knee joints are not fixed. Attempts to maintain a vertical position lead to bending of the legs. All this leads to the fact that the patient has to stay in bed or in a wheelchair most of the time.
They change their position in bed due to tension in the muscles of the arms and shoulder girdle. Passive movements are performed by patients without muscle tension, but active movements are performed with difficulty, and their amplitude is very limited due to severe muscle weakness. Flaccid paralysis occurs with profound disturbances in muscle movement and trophism. The muscle tone is sharply reduced, the muscles are flabby and atrophic, so the foot acquires the pes equinus (horse foot) position - the foot hangs and is bent towards the sole, which makes walking very difficult.
In acute cases ( encephalomyelitis , acute flaccid paresis ), these phenomena appear within 7-10 days, and in chronic flaccid diseases, muscle weakness and paralysis develop gradually.
Tests and diagnostics
First of all, paresis and plegia are detected during a clinical examination. They are characterized by:
- decreased range of motion and muscle strength;
- changes in muscle tone;
- muscle wasting or atrophy;
- increased or decreased normal reflexes;
- fibrillation of the muscles of paretic limbs;
- the presence of pathological reflexes.
To clarify the diagnosis, patients are prescribed the following examinations:
- Echoencephalography of the brain - examination of the brain using ultrasound.
- Electroencephalography is a study of the electrical activity of the brain.
- X-ray contrast and radionuclide studies. With their help, the condition of the brain ventricles and subarachnoid space is assessed.
- Doppler ultrasound is a variant of the study of cerebral vessels.
- Electromyography. Allows you to identify changes in spinal cord motor neurons characteristic of neuropathies.
- Biopsy of the affected muscles with examination of the biopsy material.
- Cerebrospinal fluid puncture.
- CT scan.
- MRI of the brain.
Diet
Patients who do not have impaired swallowing can take regular food and sit on a common table. If a child can chew and swallow independently, his diet should consist of vegetables, fruits, eggs, nuts, meat, fish, cereals, but prepared food must be crushed (pureeed) to make it easy to swallow.
It is necessary to ensure that the diet contains a sufficient amount of protein products (meat, fish, cottage cheese, cheese and other dairy products, eggs) and complex carbohydrates, since rehabilitation treatment requires an increased supply of protein and energy. Fats must be present in the diet - butter and cold-pressed vegetable oils (olive, sesame, flaxseed).
Severe swallowing disorders require special nutrition adapted to the child’s characteristics, since problems with eating gradually lead to a deficiency of essential substances and energy. In such children, protein deficiency and energy deficiency progress. If swallowing continues, the child is additionally given formula through a tube (sipping method). Modern enteral nutrition is a mixture with an optimal composition of nutrients, vitamins, macro- and microelements.
There are dry mixtures ( Nutrien standard ), which need to be prepared by diluting with water, or ready-made mixtures - Nutrizon standard , Nutrien standard , Nutrizon energy and others. Children 3-5 years old with nutritional deficiencies are prescribed formulas for premature infants up to one year old. In severe cases, patients need special nutrition - enteral tube or parenteral.
Prevention
Considering that the main cause of paresis in children is cerebral palsy, its prevention includes:
- improving the health of adolescents and women of childbearing age;
- treatment of sexually transmitted infections when planning pregnancy;
- regular examinations and timely detection of pathology in pregnant women;
- timely diagnosis of coagulopathies in expectant mothers;
- prevention of premature birth;
- adequate obstetric care;
- proper resuscitation, adequate care and use of hypothermia in newborns, timely treatment of hyperbilirubinemia .
In adults, the following are important:
- prevention of injuries (traumatic brain injuries and spinal injuries);
- timely treatment of hypertension , which, if left untreated, is complicated by cerebral hemorrhage;
- exclusion of alcoholism and poisoning by alcohol substitutes.
Consequences and complications
With paralysis and paresis, complications arise from the musculoskeletal system:
- joint contractures;
- pathological attitudes;
- arthrosis;
- formation of vicious poses;
- muscle atrophy.
Joint contractures are secondary and their severity depends on the severity of the disease and the age of the patient. At first, contractures develop reflexively (from muscle contraction against the background of prolonged excitation), and then become permanent due to degenerative changes in the muscles, ligaments and tendons. The combination of various contractures forms a vicious posture in patients. Motor installations are manifested by a forced position of the limb due to excessively high muscle tone. An example of a propulsion system is the equinus position of the foot, which is formed due to the traction of the gastrocnemius and soleus muscles. With Little's disease, the patient often falls and therefore receives injuries (hematomas, fractures).
What is Strumpel's disease
Strumpell's disease, also known as familial spastic paraplegia, is a pathological process from the group of degenerative myelopathies. This disease is characterized by damage to the anterior and lateral columns of the spinal cord. In this case, the spinal structures are affected mainly in the lumbar spine, in more rare cases in the thoracic region.
This disease affects the pyramidal tracts of the spinal cord. As a result, the central nervous system is damaged, resulting in disorders of the musculoskeletal system. In the vast majority of cases, Strumpel's disease affects the lower extremities; the mechanism of its development is progressive paraparesis of the lower extremities. As the disease progresses, hypertonicity of the muscle structures of the lower extremities increases.
According to statistics, the manifestation of the disease occurs between the ages of 10 and 30 years. However, in a broad sense, the onset of Strumpel's disease is possible at any age from birth to 80 years. As for the causes of this pathology, we are talking about a genetic predisposition caused by gene mutations.
The classification of the pathological process is closely related to the reasons for its development and includes the following types of spastic paraplegia:
- autosomal dominant – the disease is observed in one of the parents, the risk of its development in the child is about 50%;
- autosomal recessive - both parents are carriers of the defective gene (only carriers), the risk of pathology in the child is about 25%;
- X-linked - only women are carriers of the defective gene, however, the disease develops in a male child.
Forecast
Functional recovery depends on the severity of the damage to the nervous system. In this regard, compensation of neurological disorders, partial compensation, or the formation of persistent syndromes are ultimately possible.
A quarter of patients move independently, while the rest cannot do without walkers or wheelchairs. With good treatment, children with paraplegia or hemiplegia survive to adulthood and live almost normal lives. The effectiveness of rehabilitation for spastic diplegia depends on how severe the motor impairment is and how much intelligence is preserved. If active rehabilitation has been carried out since early childhood, a person can acquire a profession. If mental abilities are preserved, then they are well adapted in social life. In the presence of epileptic seizures, the prognosis worsens.
With tetraplegia, accompanied by impaired swallowing and the need for feeding through a gastrostomy tube, life expectancy is sharply reduced. Hereditary diseases affecting the pyramidal system ( Strumpel's disease ) progress slowly and have a favorable prognosis for life. However, the ability of patients to work is limited at the onset of the disease, and is lost as it progresses.
Treatment of Strumpel's disease
A whole team of qualified doctors is involved in developing the optimal treatment plan. The choice of methods depends on a number of factors, taking into account the patient’s medical history, his age, the degree of disease progression, and the severity of symptoms. The treatment program for each patient is developed strictly individually, thanks to which it is possible to achieve high efficiency.
Conservative
Today, the main direction for Strumpel's disease is conservative therapy. In this case, there is no specific treatment; doctors’ actions are limited to relieving symptoms and improving the patient’s quality of life.
Thus, the main groups of drugs used are:
- muscle relaxants – reduce spasticity and relieve muscle spasms;
- tranquilizers - have a mechanism of action similar to muscle relaxants, promote muscle relaxation;
- injection of botulinum toxin into muscle structures.
Improvement in the patient's condition is also achieved through individually developed physical therapy programs, massage courses, and physiotherapy. In some cases, the patient is prescribed to wear auxiliary structures, such as orthoses.
Surgical
Surgical interventions aimed at treating Strumpel's disease are carried out only if there are appropriate indications. The most common reason for surgery is the occurrence of contractures. Surgical treatment is carried out with the involvement of specialists of the highest category, using innovative techniques and high-tech equipment.
List of sources
- Studenikin V. M., Shamansurov Sh. Sh. Neonatal neurology (collective monograph). M.: Medforum, 2014. 120–135.
- Semenova K. A. Restorative treatment of children with perinatal damage to the nervous system and cerebral palsy. M.: Codex, 2007.
- Nemkova S. A., Zavadenko N. N., Medvedev M. I. Modern principles of early diagnosis and complex treatment of perinatal lesions of the central nervous system and cerebral palsy. Toolkit. M., 2013. 76 p.
- Martynova, G.P. Acute flaccid paralysis in children. Diagnostic algorithms and management tactics - Methodological recommendations for pediatricians, infectious disease specialists and neurologists / Krasnoyarsk, 2013. - 48 p.
Prof. Dr. Bruno-Marcel Mackert
Neurology
Head of the Department of Neurology
Specialization
- Internationally recognized specialist in stroke, peripheral nervous system diseases and clinical electrophysiology
- Author of over 40 original publications
- Board of Directors of the Berlin Stroke Society (BSA)
- Member of the Board of Directors of the Berlin Center for Stroke Research (CSB)
Show doctor's personal profile