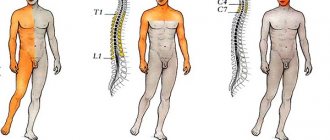
Manic syndrome (mania) is defined as a severe mental illness, which is characterized by a triad of defining symptoms - increased hyperexcited mood, motor activity and the presence of acceleration of thinking and speech function.
Often cycles with depressed mood. Thus, with bipolar affective disorder, 4 different periods appear, which are classified depending on the type and intensity of symptoms.
This mental illness affects approximately 1% of the adult population. There may be certain warning signs, but not always. The first symptoms indicating mania may occur as early as puberty or early adulthood.
Causes and etiology of the disease
To date, the exact cause of manic syndrome has not been determined.
Most often, a complex of factors is involved in the development of mania, which together form a picture of the disease. Most often, manic syndrome manifests itself as part of bipolar disorder (the so-called manic-depressive syndrome or psychosis), which is characterized by recurrence in the family history, so there is most likely a genetic predisposition to this disease.
In this regard, suggestions have been made regarding the existence of genes for bipolar disorder. However, if manic disorder were caused solely by genetic factors, then among identical twins, one of whom suffers from the disorder, the other twin would inevitably also be affected. But this fact has not been confirmed by medical research.
On the other hand, the likelihood of disease in such cases increases significantly.
Research shows that, as with other mental disorders, mania (and bipolar disorder) is the result of damage not to one gene, but to a combination of genes that, together with environmental factors (drugs and medications, surgery, physical illness, etc.) .) and cause the development of mania.
Risk factors
In addition to genetic predisposition, there are other factors that can cause a manic state. These include:
- strong emotions (shock, sadness, mental anguish, fear, etc.);
- physical and mental exhaustion;
- season;
- taking certain medications (antidepressants, corticosteroids, etc.);
- drug use (cocaine, hallucinogenic substances, opiates).
Emergency medical care for acute mental disorders with psychomotor agitation
Emergency medical care is required for acute (including suddenly developed) mental disorders (delusions, hallucinations, psychomotor agitation, etc.), accompanied by an incorrect assessment and interpretation of what is happening, ridiculous actions, when the patient’s actions become dangerous for himself and others. Such patients should be treated by psychiatrists, and specialized psychiatric teams are assigned to provide emergency care to them at large EMS stations. However, in sparsely populated (rural) areas there are no psychiatrists and psychiatric teams, and the emergency medical services doctor is often the first to meet such patients. In addition, he sometimes has to provide emergency psychiatric care when mental disorders develop in patients with various diseases of internal organs (for example, high fever, pneumonia, myocardial infarction, etc.).
Emergency therapeutic measures are indicated only for those patients whose condition poses a threat to themselves and others, primarily in the presence of agitation and aggressiveness, suicidal behavior of the patient, a state of altered consciousness, when the patient refuses to take food and liquid, his inability to self-care, and also with the development of severe side effects of psychopharmacotherapy.
Acute mental disorders are identified primarily during a conversation with the patient, during which the tactics for managing the patient are determined. The main objectives of such a conversation determine the rules of communication with patients with acute mental disorders:
- establishing initial contact;
- establishing a trusting relationship between doctor and patient;
- determining the diagnosis at the syndromic level;
- development of a medical care plan and further tactics.
Correct psychotherapeutic tactics carried out by medical staff in relation to a patient with acute psychosis can sometimes replace drug care and, in any case, be an extremely important addition to it. The main condition that the doctor must observe is not to lose “psychiatric vigilance” for a single minute, since the patient’s behavior can change sharply at any moment (there should be no objects around him that are suitable for attack or self-harm; he should not be allowed to approach window, etc.).
In addition to examining the patient's mental state, it is necessary to assess his somatic and neurological status. On the one hand, this is necessary in order not to miss somatoneurological pathology (including traumatic brain injury, other injuries and diseases), on the other hand, it can help confirm a psychiatric diagnosis (for example, identify physical exhaustion in depression) and correctly build an emergency treatment plan .
It should be remembered that any acute psychotic state, accompanied by disorganized behavior, agitation or suicidal tendencies, can pose a threat not only to the patient, but also to others. Consequently, organizational measures are required to ensure the safety of both patients and medical personnel. During the conversation and examination, it is necessary to remain alert. If the patient is aggressive, the room should not be locked. It is better to stand or sit next to the door (so that you can quickly leave the room), placing members of the emergency medical team (medic, driver), police officers, and, in their absence, relatives on both sides of the patient.
In the event of a call to the place of residence, if the patient has locked himself in a room or apartment, the doors to this room are opened only with the consent of relatives. If relatives do not give consent to forced access to the patient, despite his clearly pathological behavior, according to their description, this fact is recorded in the medical documentation and the call is transferred to the local psychiatrist at the psychoneurological dispensary. Upon receipt of consent, the doors are opened by the patient's relatives themselves or, at their request, by other persons, including police representatives and firefighters. Police officers are obliged to provide assistance to medical workers, providing safe conditions for examining the patient. When opening the apartments of single patients, the presence of police officers, as well as representatives of the housing office, is required for subsequent sealing of the doors. Pets of hospitalized single patients are handed over to police or housing office workers, and the fact of the transfer itself is certified by an act.
If called to the workplace, the patient is examined in the premises of the medical center, and if there is none, in the administrative premises, where the patient is deprived of the opportunity to offer armed resistance.
If a patient runs away at the sight of medical workers, chasing him down the street is unacceptable in order to avoid road accidents. The responsible EMS doctor is immediately informed about the fact of the patient’s escape, who must notify the police officers about the incident.
Despite the fact that a qualified assessment of the severity of symptoms can only be given by a psychiatrist, if necessary, emergency therapeutic measures are also carried out by other clinicians, including an emergency medical technician. The general strategy when providing emergency care to a patient with a mental disorder is to ensure the safety of the patient himself (which means preventing suicide or self-harm), as well as preventing possible harm to others and medical personnel (i.e. preventing aggression).
Emergency medical care for acute mental disorders includes pharmacotherapy, physical restraint (restraining the patient), delivery to an appointment with a psychiatrist, and, if necessary, to a hospital (depending on the availability of specialized psychiatric ambulance teams). If the patient requires assistance and hospitalization, the patient's consent should be obtained. At the same time, being overwhelmed by emotions and the lack of a critical attitude towards them on the part of the patient in some acute psychopathological conditions in some cases suggests the need to provide medical care, including hospitalization, without the patient’s consent.
In accordance with the Law of the Russian Federation “On psychiatric care and guarantees of the rights of citizens during its provision” (1992), hospitalization of a patient in a psychiatric hospital without his consent or without the consent of his legal representative can be carried out if the patient’s treatment or examination is possible only in inpatient conditions, and the mental disorder itself is severe and causes:
a) immediate danger to the patient himself or others;
b) helplessness of the patient, i.e. inability to independently satisfy basic life needs;
c) significant harm to the health of the patient himself due to a deterioration in his mental state if he is left without psychiatric help.
The initial psychiatric examination and decision on the issue of hospitalization of a patient in a psychiatric hospital is the exclusive competence of a psychiatrist (Law of the Russian Federation “On Psychiatric Care...”, 1992), accordingly, a patient requiring emergency psychiatric care must be immediately examined by a psychiatrist.
Thus, a doctor of the line EMS team, if there is an obvious need to provide emergency medical care to a patient and act in his interests in accordance with the Law of the Russian Federation “Fundamentals of Legislation of the Russian Federation on the Protection of Citizens’ Health” (1993), may violate the Law of the Russian Federation “On Psychiatric Care and Guarantees of Citizens’ Rights in its provision" (1992). The most accessible way out of this situation (in the absence of an on-site specialized psychiatric service in the region) is to deliver the patient by ambulance to an appointment with a psychiatrist at a psychoneurological dispensary, and at night - to the emergency room of a hospital. However, even transporting a patient to a psychiatrist (especially in cases of developed psychomotor agitation) requires certain knowledge and skills of an emergency medical technician.
The main task of drug therapy at the prehospital stage is not the treatment of the disease itself, but the drug “preparation” of the patient, which allows one to gain time before a consultation with a psychiatrist or before hospitalization in a psychiatric hospital. The main principle of providing assistance in acute psychopathological conditions is a syndromic or even symptomatic approach.
Adequate use of psychopharmacological agents allows for rapid control of almost all acute psychopathological conditions. It must be remembered that even with seemingly effective therapy, improvement may be unstable, and the patient's behavior may again become unpredictable at any time. Accordingly, if there are indications, temporary mechanical fixation should not be neglected, especially if emergency care is provided to a patient with strong motor agitation and a sharp decrease in his criticism of his behavior. A mandatory entry is made in the medical documentation about the forms and time of application of measures of physical restraint of the patient.
As practice shows, psychomotor agitation and aggressiveness constitute the main group among all mental disorders that require emergency care. Excitement is the most common reason for calling emergency services.
In an emergency setting, states of excitement are often encountered that develop against the background of acute neurological pathology (traumatic brain injury, acute cerebrovascular accidents), exogenous poisoning (for example, organophosphorus compounds), endogenous intoxication (including infections), acute therapeutic (for example, myocardial infarction) and surgical (for example, acute pathology in the abdominal cavity) diseases, emergency conditions accompanied by loss of consciousness (stupor, shallow coma), etc. In these cases, an incorrect assessment of the somatoneurological status may delay the necessary emergency therapeutic, surgical or other assistance.
Agitation is a complex pathological condition that includes speech, mental and motor components. It can develop against a background of delusions, hallucinations, mood disorders, and be accompanied by confusion, fear and anxiety. Excitement is one of the manifestations of the disease, its “nodal” point, in which features specific to each disease appear.
At the same time, the clinical and psychopathological uniqueness of this state in various diseases is preserved only to a certain extent: the increase in excitement erases the differences between its individual types, it can become chaotic, thinking can become incoherent, affect reaches maximum intensity. Excitation can lead to significant metabolic changes, and even secondary brain hypoxia, contribute to decompensation and the development of acute disorders of the cardiovascular, respiratory and other systems.
The following forms of psychomotor agitation are distinguished.
Hallucinatory-delusional arousal is characterized by an influx of visual (enemies, animals, monsters) or auditory (threatening, accusing “voices”) hallucinations and/or delusional ideas (usually persecution or influence). Hallucinatory-delusional arousal is observed in schizophrenia, epilepsy, organic brain diseases, involutional psychosis, delirium tremens (delirium tremens) and hallucinosis. In these cases, the behavior of patients depends on the nature of the hallucinatory-delusional experiences. Patients often talk with imaginary interlocutors (“voices”), answer their questions and conduct a lively dialogue. The patient sees danger to himself in everything around him and does not always understand the meaning of what is happening to him. Such patients are emotionally tense, wary, suspicious (can be angry), and they are not left for a minute with the feeling of a threat looming over them. This condition is accompanied by anxiety and fear. Patients see danger everywhere and believe that everyone around them is against them, this encourages patients to self-defense. In defense, they try to escape, attack others, and can even (this is rarely noted) make suicidal attempts to save themselves from suffering. A type of such agitation is a delirious state.
Catatonic agitation is manifested by prolonged or paroxysmal motor restlessness, often in the form of meaningless, monotonous (stereotypical) movements. Catatonic agitation is usually observed in schizophrenia or organic diseases of the brain. Such patients are characterized by negativism (active or passive opposition to others, including meaningless resistance to implementation or complete refusal to perform any actions and movements), verbalization (speech stereotypy, a tendency to monotonously repeat the same words and phrases, often completely meaningless), echolalia (repetition of phrases or words from the statements of others), echopraxia (repetition of movements), paramimia (inconsistency of facial reactions with emotional and intellectual experience). There are “silent” and impulsive catatonic excitation. “Mute” excitement is silent, chaotic, senseless, with violent resistance to others, often with aggression and/or auto-aggression. Impulsive excitement is characterized by unexpected, outwardly unmotivated actions of patients - they suddenly jump up, run somewhere, attack others with senseless rage (they can “freeze” in a stupor for a short time and become excited again).
Hebephrenic arousal has the following leading signs: extremely mannered, absurdly foolish behavior with actions of a paradoxical and pretentious nature (patients make faces, grimace, distort words, dance, jump, tumble), accompanied by unmotivated fun and ridiculous statements.
Depressive agitation occurs due to the increase in anxiety and fear in patients against the background of low mood and the absence of motor inhibition, which is manifested by motor agitation, reaching the point of violence. Typically, such arousal is characteristic of manic-depressive psychosis and schizophrenia, but can also occur in a number of other mental disorders. Clinical manifestations of agitated depression are characterized by a combination of pronounced melancholy and anxious anxiety. Patients rush about, experience “terrible” mental anguish, express ideas of self-accusation and self-abasement. They often believe that only death will bring relief to them and those around them, and therefore the danger of suicidal acts, usually sophisticatedly and carefully prepared, is extremely high. Melancholic raptus is the highest form of depressive arousal, with the development, against a background of pronounced and acute painful melancholy and confusion, of sudden “explosions” - attacks of frantic motor excitement and despair, with an expression of horror on the face, groans, sobs, wringing of hands, throwing of patients (they cannot “ find a place for yourself"), are capable of self-harm, even suicide.
Manic excitement is accompanied by elevated mood, a desire for constant vigorous activity and speech agitation. Manic agitation is characteristic of manic-depressive psychosis, schizophrenia, organic diseases of the brain, during treatment with steroid hormones and quinine poisoning. Such patients are unreasonably cheerful, are in constant motion, experience a physical feeling of vivacity, are inexhaustible and tireless in their activities, easily make contact, take on any task, but do not complete anything. When talking, they easily switch from one topic to another without finishing the discussion of the previous one. When excitement reaches its maximum, patients cannot “sit still”; they constantly talk loudly and even scream; all attempts to calm them down remain unsuccessful. Persistent insomnia is added. During this period, a cheerful mood can be replaced by irritable anger, patients do not tolerate objections, openly express their dissatisfaction, showing violent angry and aggressive reactions with destructive actions when others try to interfere with the implementation of their plans. Patients' overestimation of their own capabilities and inability to control their actions, combined with attacks of aggressiveness, sometimes lead to dangerous actions (for example, rape, murder).
Panic (psychogenically caused) agitation represents meaningless motor agitation in the form of a so-called “motor storm.” The cause of such excitement is usually sudden strong emotional shocks from psychotraumatic situations that pose a direct threat to people's lives (transport accidents, industrial accidents, fires, earthquakes, floods, etc.). Against the background of emerging disorders of consciousness, from affectively narrowed to deep twilight states, motor excitation predominates - from monotonous to randomly chaotic. Characterized by senseless movements and actions (patients rush around, strive somewhere, run away in panic, often towards danger), do not respond to questions from others, can cause harm to themselves, and try to commit suicide. In emergency situations, when the emotion of horror and fear predominates in the crowd, one of the tasks, in addition to providing medical assistance, is to identify the “leader” (one person or group of people) creating panic and immediately remove him (them) with the help of police officers from the outbreak .
Psychopathic agitation is characteristic of psychopathy and psychopathic behavior against the background of organic brain damage. Like psychogenic, psychopathic arousal is caused by some psychological reasons, but the difference is its purposefulness. Characterized by a discrepancy between an excessively violent emotional reaction and a stimulus that is minimal in strength and quality. Such patients are extremely agitated, loud, angry, swear (often obscenely), resist examination and interview, are prone to aggressive, destructive actions, and can demonstratively injure themselves. Their anger is usually targeted against a specific person - the imaginary offender. When trying to restrain such persons, excitement increases; the content of speech (demands, threats, abuse) changes depending on the actions of others and the situation. Often psychopathic arousal is of a “theatrical” nature; patients strive to attract attention to themselves, “working for the public.” The excitation is initially targeted (realization of drive or attitude), then global, with a narrowing of consciousness, sometimes to hysterical twilight states.
Epileptic excitation occurs suddenly and is accompanied by a pronounced affect of anger, aggressive and destructive actions against the background of hallucinations and delusional experiences of a frightening nature. Occurs during twilight stupefaction, before or after convulsive seizures, with epileptic psychoses and organic diseases of the brain. Epileptic agitation usually occurs against the background of a twilight disorder of consciousness (excluding the possibility of contact with patients and the patient’s criticism of his actions) and in its intensity exceeds all other options encountered in psychiatric practice. The strength of affect is determined by vivid, frightening hallucinations with pictures of world catastrophes, raging fires, massacres; the patient hears threats, screams, moans, sees blood pouring. An extreme degree of aggressiveness (as a discharge of affect) directed at others is characteristic; serious consequences are possible (murder, injury, auto-aggression, etc.).
Fussy (senile) agitation is observed with severe atherosclerosis of cerebral vessels and atrophic processes in the brain in elderly people, often with the increase of acquired dementia (dementia). It develops gradually against the background of senile insomnia and is a manifestation of the patient’s “exciting” anxious thoughts and fears. Accompanied by aimless actions and motor restlessness (patients rush out of bed and room, fussily get ready somewhere, look for and pack things, strive to go outside, and when trying to hold them they show quite active resistance, even aggression).
The actions of the doctor of the linear EMS team on a call are shown schematically in the figure.
Typically, diagnosing psychomotor agitation does not present any particular difficulties. In these cases, it is important to assess the degree of possible aggression of the patient.
During the examination, the doctor's behavior must obey certain rules.
- A dismissive, bewildering, blaming, threatening or judgmental tone of conversation may cause or increase the patient's aggression. The conversation should be conducted calmly, with reasonable persistence, non-contradiction with the patient, and compliance with his permissible demands. In some cases, the patient can be calmed down with a properly conducted conversation.
- Establishing contact is facilitated by creating in the patient the impression that the doctor can take his place (“I understand that you are very nervous...”).
- You should not get too close to the patient. This may be perceived as a threat.
- At the same time, it is important not to give the patient the opportunity to harm the doctor. It is advisable to have employees nearby. Consideration should be given to how to protect your face, neck and head. First you need to take off your glasses, tie, necklaces, etc. During the conversation, the doctor must take care of a possible “retreat” and be closer to the door of the office or ward than the patient.
If the manifestation of psychomotor agitation is sufficiently pronounced, there may be no need to ask questions to the patient, especially if the patient behaves aggressively. In some cases (manifestation of intoxication with various substances, with traumatic brain injury, etc.), the doctor’s questions should be aimed at identifying anamnestic information important for differential diagnosis (the possibility of taking poisonous drugs, trauma, etc.).
First of all, the doctor’s attention should be directed to identifying the most characteristic symptoms of agitation - acceleration and intensification of manifestations of motor (motor) and mental (thinking, speech) anxiety.
Patients with psychomotor agitation are subject to emergency hospitalization in a specialized hospital. To do this, the psychoneurological ambulance team should be immediately called, whose doctor will determine further tactics for managing the patient.
While carrying out all the above measures, you must not give up trying to establish contact with the patient, calm him down, and explain what is happening.
Treatment
When providing assistance to an agitated patient, the main task of the EMS doctor is to ensure the safety of the patient and others. Often, to control anxiety, it is enough to create a calm environment and establish contact with the patient so that he feels safe.
For psychotic disorders (delusions, hallucinations), antipsychotic antipsychotics are used to relieve agitation. The main indication for injections of psychotropic drugs is the lack of patient consent to treatment, since the differences between tablet and injectable forms of drugs relate mainly to the speed of development of the therapeutic effect and, to a lesser extent, the level of sedation achieved. The optimal route of drug administration is intramuscular; intravenous administration of drugs is not necessary, and in some cases physically impossible.
Modern standards of therapy suggest the use of tablets (for example, risperidone, olanzapine) and injectable forms of atypical antipsychotics (for example, Rispolept Konsta) as first-line agents in all groups of patients, while traditional antipsychotics remain reserve drugs. In case of decompensation of mental illness in a somatically healthy patient, maximum doses of drugs are used to relieve agitation, if necessary. Typically, olanzapine (Zyprexa) at a dose of 5–10 mg or zuclopenthixol (Clopixol-Acufaz) at a dose of 50 mg is administered intramuscularly. The introduction of some antipsychotics (haloperidol, zuclopenthixol, olanzapine, trifluoperazine) is often accompanied by the development of extrapyramidal disorders and requires the parallel use of correctors - antiparkinsonian drugs, such as trihexyphenidyl (Cyclodol, Parkopan, Romparkin). In the absence of atypical antipsychotics, 100–150 mg (4–6 ml of a 2.5% solution) of chlorpromazine (Aminazine) or levomepromazine (Tizercin) can be administered intramuscularly. The administration of antipsychotics requires monitoring blood pressure levels due to the risk of collapse. To prevent orthostatic reactions, the use of antipsychotics in doses exceeding the minimally effective ones should be accompanied by an intramuscular injection of 2.0–4.0 ml of a 25% solution of Cordiamine (into the other buttock).
Of the tablet drugs, preference is given to risperidone (Rispolept) at a dose of 1–4 mg or clozapine (Azaleptin, Leponex), which has a strong antipsychotic and sedative effect, at a dose of up to 150 mg once.
Temporary fixation of a patient with severe agitation is allowed, subject to mandatory documentation of this procedure by the EMS doctor. In this case, the patient should be under constant supervision of medical personnel. It is important to prevent pinching of blood vessels, for which the fixing bandages must be wide enough.
According to the Law “On the Police” (1991) and the order of the Ministry of Health of the Russian Federation and the Ministry of Internal Affairs of the Russian Federation “On measures to prevent socially dangerous actions of persons suffering from mental disorders” No. 133/269 of April 30, 1997, law enforcement agencies must provide assistance to doctors in such cases.
Tranquilizers (in particular, benzodiazepines) are most effective for neurotic disorders, in particular panic attacks; their use is also recommended in cases where the diagnosis is unclear. From the group of benzodiazepines, it is optimal to use drugs with a shorter half-life and maximum anxiolytic effect, for example, lorazepam. For agitation that develops as a result of deep metabolic disorders (during intoxication, severe infection, etc.), it is also preferable to use benzodiazepine tranquilizers - diazepam at a dose of 10-30 mg (2-6 ml of 0.5% solution) or lorazepam at a dose 5–20 mg (2–8 ml of 0.25% solution). It is better not to use neuroleptics in such cases, and if necessary, the dose of the drugs should be reduced.
For agitated depression (with prolonged speech motor excitation), melancholic raptus, intramuscular administration of antidepressants with a sedative effect (in order to potentiate the calming effect), for example, amitriptyline at a dose of 40–80 mg (2–4 ml of a 2% solution) is possible. Dosages of psychotropic drugs available in injectable form and used for emergency treatment of mental disorders are shown in the table.
The drugs of choice for the treatment of psychomotor agitation are sedative neuroleptics, including in combination with diphenhydramine (Diphenhydramine) or promethazine (Diprazine, Pipolfen), or tranquilizers. Tranquilizers should be preferred in the elderly, in the presence of severe somatic diseases, severe hypotension.
Drugs are administered parenterally, but they should not be neglected when administered orally, thereby affecting the speed of onset of action of the drug.
It is necessary to adjust the doses of drugs upward if the patient has previously received psychopharmacotherapy.
Haloperidol, zuclopenthixol, olanzapine, trifluoperazine must be prescribed with a corrector - trihexyphenidyl (Cyclodol) at a dose of 2 mg.
To a greater extent, the choice of the drug used will be determined by the availability of the necessary drugs (including in the arsenal of emergency physicians) and the minimum of possible negative consequences. According to our observations (data from a large multidisciplinary hospital in a metropolis), a greater number of cases of severe side effects of therapy at the prehospital stage are associated with the prescription of incorrectly selected doses of such an available “unaccounted” tranquilizer as Phenazepam.
The doctor of the linear EMS team should know certain provisions of the Order of the Ministry of Health of the Russian Federation “On emergency psychiatric care” No. 108 of 04/08/98 in order to better navigate the management of patients with mental disorders.
Common errors:
- Leaving a patient without proper observation and control over his behavior.
- Underestimation of the danger of psychomotor agitation for the patient himself and those around him (including failure to attract help from police officers).
- Neglect of physical restraint methods.
- Confidence in the need for only intravenous administration of sedatives, excluding intramuscular and oral routes.
- Non-use of correctors when administering neuroleptics that can cause side extrapyramidal disorders.
When carrying out any drug intervention, the EMS doctor must remember that doses of psychotropic drugs are selected based on the patient’s physical condition (body weight, age, concomitant somatoneurological pathology).
In addition, it should be taken into account that the use of psychotropic drugs “erases” the severity of psychopathological symptoms, which subsequently creates difficulties for the psychiatrist in making a decision on the patient’s involuntary hospitalization. Accordingly, prehospital psychopharmacological intervention is appropriate only in cases where the patient's mental state would interfere with safe transport; the exception is long-term transportation from remote locations. Specialized psychiatric teams follow the same tactics.
V. G. Moskvichev , Candidate of Medical Sciences MGMSU, NNPOSMP, Moscow
Clinical picture
Manic-depressive syndrome is manifested by significant mood swings - from unusually “good” to irritation, sadness and even hopelessness. Such fluctuations can be repeated cyclically. An episode of “elevated” mood is called mania, while an episode of sad mood is characterized by depression.
Symptoms of manic syndrome:
- unusually good, high spirits;
- increased energy, activity, restlessness;
- significant irritation;
- very fast thinking and speech, “jumping” from one thought to another;
- impaired concentration;
- low need for sleep;
- unrealistic ideas about your abilities;
- excessive material costs;
- increased sexual need;
- use of drugs, alcohol;
- provocative and aggressive behavior;
- denial, not accepting any refusal.
Manic tendencies exist if an excessively good mood in combination with at least 3 other symptoms persists for a week (at least).
Types of mania
Mood disorders have been studied since the 5th century BC. Hippocrates identified borderline states - mania and melancholy. At the end of the 19th century, E. Kraepelin put forward the concept according to which all behavioral disorders were classified as manic-depressive psychosis (MDP).
Throughout the twentieth century, this concept was considered basic, and only recently have behavioral disorders received a more detailed classification. First of all, it was pointed out that there are two main types of TIR:
- Episodes of depression are replaced by mania and inappropriately elevated mood, which entails mental disorders.
- Depression can alternate with hypomania, in which mood elevations are not associated with serious mental disorders.
The modern classification of diseases ICD-10 distinguishes three degrees of mania, the mildest of which is hypomania. It is followed by mania without psychotic symptoms and mania that is manifested by psychotic symptoms.
Hypomania, in turn, is also classified according to several criteria:
- Based on the degree of predominance of some symptoms of the disorder, hypomania can be simple, it is also called cheerful, irritable or angry, as well as expansive;
- division into types can be carried out based on the type of disorders accompanying an episode of mild mania. When there is a tendency to litigiousness, hypomania is called querulant; there is also an opportunistic and dysphoric form of pathology;
- Based on their severity of symptoms, hypomania is divided into obvious or pure, as well as hidden, when the symptoms are less pronounced.
Hypomania can affect the psychosomatic sphere, in which case euphoric hypochondria develops. A person in such a state directs all his energy to actively fight an imaginary illness.
What does a manic personality look like?
A person in a hypomanic period has a chronically elevated good mood, excess energy, increased mental and physical activity, and generally feels in good shape. He is very talkative and easily establishes contacts with other people, communicates without barriers.
This period of increased activity can also be reflected in a person’s sexual life, which can lead to superficial and reckless sexual relationships, and frequent changes of partners.
The onset of this period comes completely unexpectedly, without any warning signals and, as a rule, is well tolerated by the person.
The manic phase can be described as a period of excessively good mood and noticeably increased activity. A person feels absolute strength in all directions, in the eyes of himself he is invincible and unsurpassed.
As the number of ideas, pace and productivity increases, a person does not want to waste time on the opinions of others. If someone or something interrupts his activities, this increases his irritation, and the slightest irritation ignites his aggressiveness; a person may act inappropriately and dangerously.
Sometimes the manic personality is full of gaiety and tells jokes, often with vulgar or sexual overtones, even in socially unacceptable situations.
A person refutes any social taboos, which makes his behavior irresponsible, inappropriate and risky, endangering not only himself, but also those around him. He immediately implements his ideas and thoughts, without realizing the consequences in the personal, social and financial spheres. For example, you can note frequent excessive expenses when purchasing unnecessary items, entering into unprofitable or even fraudulent contracts.
Serious consequences are fraught with mania with psychotic symptoms (psychomanic syndrome), when a person simultaneously experiences a delusional disorder and hallucinations. These people often have “grand” ideas in which they are pathologically convinced, and they do not doubt their importance and superiority.
Megalomaniacal delusions can affect the mental aspect, which is manifested, for example, by a person’s belief that he speaks all the languages of the world, as well as the physical aspect of the personality. For example, a person considers himself the strongest in the world, immortal, not susceptible to any disease.
Other psychotic symptoms include paranoid symptoms, characterized by pathological resentment, suspicion and morbid thoughts.
Spectrum of disorders
Symptoms of mania can vary in intensity:
- hypomania – mild form; the disorder does not cause significant harm to a person's psychosocial functioning and is characterized by moderately elevated mood that persists for at least 4 consecutive days, increased energy, activity, and a feeling of increased productivity;
- classic mania – elevated mood and agitation lasting more than a week, increased self-esteem, loss of social inhibitions, risky behavior;
- manic disorder with psychotic symptoms often requires hospitalization, the disease is characterized by the presence of delusions and hallucinations; this form affects about 1/3 of patients (manias, usually expansive, religious, erotic, etc.).
Manic syndrome is divided into 3 types:
- euphoric syndrome - a feeling of bliss, contentment without significant hyperactivity;
- stuporous mania – complete absence of psychomotor symptoms;
- resonant mania - irritability, anxiety, sometimes aggression.
Symptoms
Mania is characterized by an elevated mood, with a feeling of euphoria, lightness, “special clarity in the head,” a feeling that “everything is working out easily,” and optimism. Such people speak quickly and a lot, are “easy-going”, and look younger than their age. They easily form ideas of their own greatness, superiority and even power. Often because of this, they give up their usual activities (study, work, projects), leave their families, change their religion and even their appearance (dye their hair, have plastic surgery). Mania is always accompanied by hyperactivity: patients are restless, active, constantly busy with something, and do not feel tired. Sleep is disturbed: it shortens or stops altogether.
During a manic state, patients take out loans, commit irrational actions, make expensive purchases, and enter into marriages that quickly break up.
Diagnostic criteria
The diagnosis is made based on the medical history and interview with the patient. The exact type of mania is determined and appropriate treatment is decided. If necessary, tests are carried out to determine what type of mania the patient has developed.
Rorschach test
The Rorschach test (inkblot test) is one of the psychological methods used to analyze personality. This is a projective test that uses the projection of thinking processes and personal qualities onto undefined objects.
Altman scale
The Altman Scale is a self-report diagnostic scale that can be used to assess the presence and severity of manic and hypomanic symptoms, most commonly in patients suspected of having bipolar disorder.
This scale can assess differences in “normal” or baseline levels from mania in 5 subjective and behavioral areas:
- positive mood;
- self confidence;
- need for sleep;
- speech;
- activity.
Diagnostic features
In our clinic, psychiatrists make a diagnosis based on the entirety of available data.
They take into account:
- Developing clinical picture.
- Information received from relatives during client interviews.
- Diagnostic test results.
- Opinion of other experts.
Particular attention is paid to differential diagnosis.
TIR should be distinguished from:
- Variants of schizophrenia.
- Neurotic disorders.
- Substance addiction.
- Symptoms of mental disorders observed against the background of pathology of internal organs and the thyroid gland.
Establishing a diagnosis sometimes requires time and special medical responsibility.
Therapy methods
In the treatment of manic syndrome, 2 main groups of medications are used: mood stabilizers and antipsychotics.
The patient may also be prescribed medications that have auxiliary effects, for example, for insomnia, anxiety and restlessness, etc.
The main drugs used in therapy:
- Mood stabilizers : a group of drugs intended for preventive treatment. Their long-term use reduces the risk of relapse of depression or mania. Drugs in this group are also used in acute cases of mania or depression.
- Antipsychotics (antipsychotics) : drugs used to treat mania or depression. Some of the newer antipsychotic drugs have also demonstrated effectiveness in long-term, prophylactic use, thus resembling the effects of mood stabilizers.
Additional (auxiliary) drugs:
- Antidepressants are used to treat depression. It is not recommended to use drugs in this group without a mood stabilizer - this can lead to a worsening of the disease.
- Sleeping pills and tranquilizers are intended only for short-term use in the treatment of insomnia, anxiety, in cases of tension or excitement.
How dangerous is a maniac for himself and for people?
In about half of the cases, there is an increase in the consumption of alcohol or drugs by the manic person.
Manic syndrome also carries various social risks. A person can cause inconvenience to himself, for example, with inappropriate jokes or arrogant behavior. The public, as a rule, is not sufficiently informed about a person’s mental state, and associates such behavior with the characteristics of his character. This significantly complicates the personal and social life of a manic person.
The significant financial losses that accompany reckless behavior in the manic phase often lead to subsequent social problems, logically related to the partner or marital relationship, which may also be negatively affected by this mental disorder.
Mania is a mental disorder that, unfortunately, cannot be prevented because... such disorders are mainly associated with hereditary transmission.
A healthy lifestyle, sufficient physical activity, avoidance of stressful and emotionally difficult situations and factors, regular and high-quality sleep, avoidance of alcohol and other psychoactive substances (marijuana, LSD, cocaine, methamphetamine, etc.) can bring certain benefits.