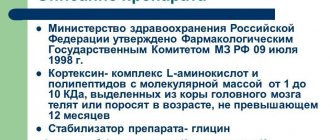
We begin the comparison of Cerebrolysin and Cortexin by describing basic information about each drug. Cortexin is produced by a Russian pharmaceutical company in the form of ampoules with lyophilisate. The medicine contains proteins and one auxiliary component - a stabilizer. Each package of Cortexin contains 10 ampoules with dry substance. The main pharmaceutical substance is obtained by extraction methods from the central nervous system of pigs and cows.
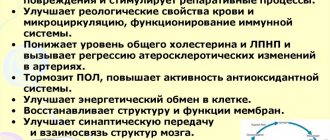
The main property of Cortexin is the ability to improve metabolism in brain tissue, protect nerve cells from adverse external and internal factors, regeneration and neuromodulation. As a result, the synthesis of peptides in the central nervous system accelerates, metabolism, cognitive functions, memory, thinking, attention, physical and mental activity improve. Indications for use of Cortexin :
- acute cerebrovascular accident and rehabilitation period;
- brain diseases of various etiologies;
- VSD;
- inflammation of the brain substance in acute and chronic form;
- epileptic seizures;
- injuries with damage to the central nervous system;
- cerebral palsy;
- mental retardation in children;
- disorders of thinking, short-term memory, attention and other cognitive functions.
There are 2 contraindications for the use of Cortexin : pregnancy and increased sensitivity of the body to the components of the drug.
To use Cortexin, the lyophilisate is first diluted in an isotonic solution or in a solution of novocaine, then 10 mg of the drug is administered intramuscularly. The duration of the course of treatment is prescribed individually and is usually one and a half weeks. For children, dosages are selected based on body weight (0.5 mg per kilogram). Courses of therapy can be repeated several times a year after consultation with your doctor.
Cortexin has virtually no side effects . Only allergic manifestations are possible in susceptible individuals. The price of the drug in pharmacies ranges from 800 to 1300 rubles, depending on the dosage and the number of bottles in the package.
pharmachologic effect
Cerebrolysin contains low molecular weight biologically active neuropeptides that penetrate the BBB and directly enter nerve cells.
The drug has an organ-specific multimodal effect on the brain, i.e. provides metabolic regulation, neuroprotection, functional neuromodulation and neurotrophic activity. Metabolic regulation:
The drug Cerebrolysin increases the efficiency of aerobic energy metabolism of the brain, improves intracellular protein synthesis in the developing and aging brain.
Neuroprotection:
the drug protects neurons from the damaging effects of lactic acidosis, prevents the formation of free radicals, increases survival and prevents the death of neurons under conditions of hypoxia and ischemia, and reduces the damaging neurotoxic effect of excitatory amino acids (glutamate).
Neurotrophic activity:
Cerebrolysin is the only nootropic peptidergic drug with proven neurotrophic activity similar to the action of natural neuronal growth factors (NGF), but manifested under conditions of peripheral administration.
Functional neuromodulation:
The drug has a positive effect in cases of cognitive impairment on memory processes.
Indications
Both drugs have common indications for use:
- Encephalopathy
- Brain infarction
- Cerebrovascular disease
- Intracranial trauma
There is a fairly large number of studies that prove the positive effect of neuropeptides (which contain Cortexin and Cerebrolysin) on the healing of nerve structures after damage.
However, there are also differences. Cortexin can be used if:
- Asthenic (emotionally labile) disorders.
- Disorders of speech, language, learning skills.
- Cerebral palsy.
- Intellectual-mnestic dysfunctions.
- Delayed developmental stages.
- Malaise and fatigue.
The fact is that Cortexin has a strong influence on cognitive processes associated with the transmission of impulses in the central nervous system.
Cerebrolysin is used in the following cases:
- Dementia of various etiologies.
- Alzheimer's disease.
- Depression.
- Excessive activity (pathological motor activity).
Studies have revealed the ability of Cerebrolysin to normalize the ratio of excitatory and inhibitory neurotransmitters, which is now actively used in medicine.
Speaking about indications for use, it is important to say that Cerebrolysin appeared quite a long time ago - in the 1970s. During its existence, a fairly large amount of information has accumulated about its effects in clinical trials and in practice.
Cortexin is a newer drug, it appeared about 20 years ago, but the experience of its use is already quite large and contains enough data on positive effects.
Dosage
The drug is used parenterally. The dose and duration of use depend on the nature and severity of the disease, as well as the age of the patient. A single administration of the drug in a dose of up to 50 ml is possible, but a course of treatment is more preferable.
The recommended course of treatment is daily injections for 10-20 days.
| Indication | Dose |
| Acute conditions (ischemic stroke, traumatic brain injury, complications of neurosurgical operations) | from 10 ml to 50 ml |
| In the residual period of cerebral stroke and traumatic injury to the brain and spinal cord | from 5 ml to 50 ml |
| Psychoorganic syndrome and depression | from 5 ml to 30 ml |
| Alzheimer's disease, dementia of vascular and combined Alzheimer's-vascular origin | from 5 ml to 30 ml |
| In neuropediatric practice | 0.1-0.2 ml/kg body weight |
To increase the effectiveness of treatment, repeated courses can be carried out as long as the patient's condition improves as a result of treatment. After the first course, the frequency of injections can be reduced to 2 or 3 times a week.
Cerebrolysin is used parenterally in the form of intramuscular injections (up to 5 ml) and intravenous injections (up to 10 ml). The drug in a dose of 10 ml to 50 ml is recommended to be administered only through slow intravenous infusions after dilution with standard solutions for infusion. The duration of infusions ranges from 15 to 60 minutes.
Side effects of drugs on the body
The development of side effects (Table 1) occurs in rare cases, and usually disappear on their own after a few days.
| Body systems | Negative effects |
| Blood flow system and cardiac organ |
|
| CNS |
|
| The immune system |
|
| Digestive system |
|
| Respiratory system |
|
| Leather |
|
| General negative reactions of the body |
|
Side effects
The frequency of adverse reactions was determined in accordance with WHO recommendations: very often: (≥1/10); often: (from ≥1/100 to <1/10); uncommon (from ≥1/1000 to <1/100); rare (from ≥1/10,000 to <1/1000); very rare, including isolated reports (<1/10,000).
From the immune system:
very rarely - increased individual sensitivity, allergic reactions.
Mental disorders:
rarely - the expected activation effect is accompanied by agitation, manifested by aggressive behavior, confusion, and insomnia.
From the nervous system:
rarely - too rapid administration of the drug can lead to dizziness; very rarely - isolated cases of generalized epilepsy and one case of seizures were associated with Cerebrolysin.
From the cardiovascular system:
very rarely - too rapid administration of the drug can lead to increased heart rate and arrhythmia.
From the digestive system:
very rarely - dyspepsia, diarrhea, constipation, nausea, vomiting; rarely - loss of appetite.
For the skin and subcutaneous tissues:
very rarely - skin reactions; rarely - with excessively rapid administration, a feeling of heat, sweating, and itching may occur.
General disorders and disorders at the injection site:
very rarely - redness, itching, burning at the injection site, pain in the neck, head and limbs, fever, mild back pain, shortness of breath, chills, collapsing state.
One study reported an association between rare use (>1/10,000 to <1/1,000) with hyperventilation, hypertension, hypotension, fatigue, tremor, possible depression, apathy and/or somnolence, and flu-like symptoms. (cold, cough, respiratory tract infections).
Since Cerebrolysin is used mainly in elderly patients, the above symptoms of diseases are typical for this age group and often also occur without taking the drug.
It should be noted that some undesirable effects (excitement, arterial hypertension, arterial hypotension, lethargy, tremor, depression, apathy, dizziness, headache, shortness of breath, diarrhea, nausea) were identified during clinical studies and occurred equally in patients treated with Cerebrolysin and in patients in the placebo group.
If any of the side effects indicated in the instructions are aggravated or any other side effects not specified in the instructions are noted, the patient should inform the attending physician.
Notification in case of suspected side effects
It is important to report side effects after drug approval to ensure ongoing monitoring of the drug's risk-benefit profile. Healthcare professionals are asked to report all cases of adverse reactions observed with the drug through national adverse reaction reporting systems and/or to the company's representative office.
Place of drugs in therapy in children
A common question that is asked when prescribing Cerebrolysin or Cortexin is which is better for children. The effectiveness of Cortexin has been confirmed by studies in the treatment of infants on the second day after birth with cervical trauma. The medication did not have a stimulating effect on the body, which distinguishes it from other nootropics.
For newborns, this medication is a priority in cerebroprotective therapeutic treatment.
Cerebrolysin is recommended for children with the following symptoms:
- frequent pain in the head and cervical region;
- increased feeling of fatigue;
- irritability and nervousness;
- impaired concentration and inattention;
- memory loss;
- sleep disturbance.
Drug interactions
Taking into account the pharmacological profile of the drug Cerebrolysin, special attention should be paid to possible additive effects when co-administered with antidepressants or MAO inhibitors. In such cases, it is recommended to reduce the dose of the antidepressant. The use of Cerebrolysin in high doses (30-40 ml) in combination with MAO inhibitors in high doses can cause an increase in blood pressure.
Cerebrolysin and balanced solutions of amino acids should not be mixed in the same solution for infusion.
Cerebrolysin is incompatible with solutions containing lipids and with solutions that change the pH of the medium (5.0-8.0).
What's best for a child?
Increased demands are placed on medications in pediatric practice in terms of safety and effectiveness. Both Cortexin and Cerebrolysin have found their use in children. Cortexin has shown the best effect for the treatment of epilepsy (as part of complex therapy), convulsive syndrome, cerebral palsy and delayed development of certain brain functions (speech, learning skills). Due to the risk of side effects of Cerebrolysin, the drug is contraindicated for status epilepticus in a child.
Each tool has its own strengths and weaknesses. It is necessary to choose a medicine strictly individually, taking into account the nature of the disease, concomitant pathologies and individual characteristics of the person. There is no ideal universal “pill”; any drug will be effective only in cases where the indications for its use are met.
special instructions
If injections are performed too quickly, a feeling of heat, sweating, and dizziness may occur. Therefore, the drug should be administered slowly.
The compatibility of the drug has been tested and confirmed (within 24 hours at room temperature and light) with the following standard solutions for infusion: 0.9% sodium chloride solution, Ringer's solution, 5% dextrose (glucose) solution.
The simultaneous use of Cerebrolysin with vitamins and drugs that improve cardiac circulation is allowed, but these drugs should not be mixed in the same syringe with Cerebrolysin.
Only clear Cerebrolysin solution should be used and only once.
Impact on the ability to drive vehicles and operate machinery
Clinical studies have shown that Cerebrolysin does not affect the ability to drive vehicles and use machinery.
Simultaneous use of Cortexin and Cerebrolysin
It is not advisable to prescribe Cortexin simultaneously with Cerebrolysin , since the drugs have similar pharmacological and pharmacokinetic properties; they will not complement each other, but will only excessively enhance the effect. Ultimately, this can lead to symptoms of overdose and increased excitability of the nervous system.
Cerebrolysin and Cortexin can be used simultaneously only by reducing the dosage of each drug by at least half. This combination must be discussed with your doctor.
Release form, composition and packaging
Injection
yellowish-brown, transparent.
| 1 ml | |
| Cerebrolysin concentrate (a complex of peptides* obtained from pig brain) | 215.2 mg |
* molecular weight not more than 10,000 daltons.
Excipients:
sodium hydroxide, water d/i.
- 1 ml - brown glass ampoules (10) - contour cell packaging (1) - cardboard packs.
- 2 ml - brown glass ampoules (10) - contour cell packaging (1) - cardboard packs.
- 5 ml - brown glass ampoules (5) - contour cell packaging (1) - cardboard packs.
- 10 ml - brown glass ampoules (5) - contour cell packaging (1) - cardboard packs.
- 20 ml - brown glass ampoules (5) - contour cell packaging (1) - cardboard packs.
- 30 ml - brown glass bottles (1) - cardboard packs.
- 30 ml - brown glass bottles (5) - cardboard packs.
Compound
Both drugs have a similar composition - they are polypeptides from the cerebral cortex of animals. Cerebrolysin is made from the nerve structures of pigs, and Cortexin is made from cattle.
There are some differences in the manufacturing process. Cerebrolysin is obtained by breaking down brain proteins into their components. The disadvantage of this method is that the likelihood of destruction of the necessary aminopeptides increases. In the manufacture of Cortexin, lyophilization (freezing and vacuum processing) is used. Due to this, a direct transition of a substance from a solid to a gaseous state is achieved, which reduces the destruction of proteins and amino acids.
Comparative analysis of the effectiveness of Cerebrolysin in the treatment of patients with chronic cerebral ischemia.
Comparative analysis of the effectiveness of Cerebrolysin in the treatment of patients with chronic cerebral ischemia. Pharmacoeconomic aspects
E.I. Chukanova. Department of Neurology and Neurosurgery, Faculty of Medicine, Russian State Medical University
Due to the prevalence of vascular diseases of the brain, the variety of their forms and characteristics of the course (cerebral vascular crises, transient ischemic attacks (TIA), strokes, sometimes combined disorders of cerebral and coronary circulation), the difficulty and not always effective treatment of cerebral circulatory disorders is becoming more and more Recently, attention has been paid to their prevention, that is, early diagnosis and treatment of chronic cerebrovascular insufficiency [2, 3, 5, 6, 11, 12, 14, 16].
The pathogenesis of dyscirculatory encephalopathy is caused by cerebral circulatory failure in a relatively stable form or in the form of repeated short-term episodes of dyscirculation, which can be asymptomatic or manifest clinically. The degree of structural changes in the brain during dyscirculation can range from changes in individual neurons, gliocytes and white matter fibers to infarctions of various sizes and localization [2, 8, 16], which ultimately manifests itself as focal changes in the brain substance, diffuse changes in the white matter and cerebral atrophy.
In conditions of chronic brain hypoperfusion, compensation mechanisms are depleted, the energy supply of the brain becomes insufficient, as a result of which functional disorders first develop, and then irreversible diffuse morphological changes in the brain, which prepare the brain tissue for the development of stroke. The formation of any focus of ischemic damage is accompanied by the synthesis and secretion of a wide range of regulatory peptides, directed migration of inflammatory cells, and activation of various signaling molecules. It has been shown that when changes occur in the infarction zone, an imbalance of cytokine status occurs with a deficiency of protective anti-inflammatory interleukins and trophic factors, in particular NRF [1, 2]. NRFs are physiologically active polypeptides that regulate the growth and differentiation of neurons in developing systems and their functional stability. In adulthood, NRFs protect neuronal structures from traumatic, hypoxic, ischemic and other damage [2].
One of the drugs with proven neuroprotective and neuroregenerative effects is Cerebrolysin [1, 6, 9, 10]. It is based on natural neuropeptide and growth factors isolated from the brain of pigs. The main mechanisms of action of Cerebrolysin are the regulation of brain energy metabolism, the actual neutrophic effect and modulation of the activity of endogenous growth factors, interaction with neuropeptide and neurotransmitter systems. Experimental studies have shown that Cerebrolysin reduces the brain's need for oxygen, creating its increased resistance to hypoxia factors, the antioxidant properties of the drug have been proven due to the inhibition of free radical oxidation and lipid peroxidation, as well as a positive effect on the homeostasis of microelements (magnesium, selenium, vanadium manganese) with antioxidant properties. Cerebrolysin has also been proven to have a positive effect on the state of cholinergic neurons, accompanied by a significant change in the level of acetylcholinesterase, which apparently is one of the mechanisms of the nootropic effect of the drug [9, 10].
A pharmacoeconomic study was conducted on the effectiveness of the drug Cerebrolysin in patients with chronic cerebrovascular insufficiency.
The purpose of the study was a pharmacoeconomic analysis of the effectiveness of treatment with Cerebrolysin in patients with different stages of chronic cerebrovascular insufficiency. The objectives of the study included: studying the clinical effectiveness of Cerebrolysin in patients compared to the control group, identifying features of the progression of discirculatory encephalopathy (DE) and its outcomes in patients of the main and control groups, comparative assessment of the economic effectiveness of Cerebrolysin.
Material and methods
The study group consisted of 154 patients with DE stages I, II and III, who were undergoing outpatient treatment and receiving the drug Cerebrolysin, prescribed in a dose of 5–10 ml for 10 days. In addition, patients in the study group received “basic therapy,” which was maximally unified and included aspirin (100 mg/day), dipyridamole (150 mg/day), glycine (900 mg/day) and Enap. Enap was prescribed in an individual dose, depending on the stage of hypertension and the level of initial pressure. Blood pressure correction reached a level of 120/70 mm Hg. Art. – 140/80–85 mm Hg. Art. depending on the duration of blood pressure, the severity of cerebral perfusion disorders and the initial level of blood pressure at the beginning of the study. If the effect of Enap on lowering blood pressure was insufficient, Enap was combined with Arifon at a dose of 2.5 mg/day. The control group included 118 patients with DE, clinically comparable to patients in the study group. Patients in the control group received “basic therapy”, similar to patients in the study group. All patients of the main and control groups were treated as outpatients and were observed for a year.
The neurological status of patients was recorded before inclusion in the study, and then at the end of the 1st, 6th, and 12th months. The main and control groups were comparable in gender, age, etiology, severity and predominant localization of the pathological process. The study was conducted openly. The randomization method was used to recruit patients.
The distribution by stages of DE was: DE I – 40 patients, DE II – 51, DE III – 63 patients. The etiological factors of DE were: arterial hypertension - in 57 (37.09%) patients, atherosclerosis - in 35 (22.7%), a combination of atherosclerosis and arterial hypertension - in 62 (40.3%) patients. For the purpose of a detailed assessment of the neurological status and the possibility of subsequent data processing, the following scales were used: MFI-20, MCA:FMA (Motor Club Assessment: Functional Movement Activities), Tinnetti scale (Functional Mobility Assessment in Eldery Patients), Spielberger anxiety scale (State-Trait Anxiety Inventory), Hamilton Depression Rating Scale, Mini Mental State Examination MMSE, Recovery Locus of Control questionnaire [7].
In view of the different scales and different directions of the scales used, for the convenience of presentation and perception of the material, we found it convenient to describe the dynamics of the mentioned indicators in terms of relative changes, speaking about the percentage of improvement (or deterioration) of the corresponding indicator in relation to its initial state. At the same time, the difference (95%) between the indicators of the study and control groups, differing by more than 2.5 times, was considered reliably significant; and at 90% - 2 times.
In addition to clinical examination, all studied patients underwent laboratory, instrumental and neuroimaging studies.
Research results
After the first course of treatment with Cerebrolysin in doses of 5 and 10 ml/day, a statistically significant effect of the drug on all studied scales was observed, with the exception of its effect on the score of “violent laughter and crying”. The use of Cerebrolysin at a dose of 5 ml/day for a course of 10 days showed a lesser clinical effect, however, when considering the effect of Cerebrolysin on the severity of asthenic syndrome and indicators of emotional status, it was noted that asthenic symptoms regressed by 59.6%, the prevalence of cephalgic syndrome decreased by 91 .2%. At the same time, scores on the anxiety (9.6±2.5 points) and depression (2.9±0.8) scales indicated the absence of anxiety-phobic and depressive disorders.
In table Figure 1 shows the severity of clinical manifestations of DE at the end of the first course of treatment with Cerebrolysin compared to the control group.
In addition to the effect on the severity of asthenic syndrome, anxiety, motivation and cognitive impairment in patients with stage I DE, Cerebrolysin was also effective against axial reflexes (16.9 and 23.7%), as well as vestibular ataxia (20.9 and 37. 8%). When analyzing the clinical picture in patients with DE II and DE III, a statistically significant effect of the drug on the score of the “movement” scale, amyostatic syndrome, cerebellar and frontal ataxia was noted.
By the beginning of the second course of treatment with Cerebrolysin in patients with DE I (6th month of observation), the “trace” effect remained during treatment at both a dose of 5 and 10 ml/day. In patients with DE II and DE III, the corresponding effect remained at a dose of 10 ml/day in relation to asthenic syndrome, anxiety and motivation.
After the second course of treatment with Cerebrolysin (7th month of observation), a statistically more significant effect of the drug on the scores of the selected scales was noted (Table 2), with the exception of the degree of influence of the drug on the severity of asthenic syndrome and neuropsychological characteristics in patients with stage I DE, which is most likely due to a good restoration of these functions as a result of complex treatment. The second course of treatment with Cerebrolysin statistically significantly improved the scores on the scales of movement, ataxia, pseudobulbar and amyostatic syndromes (CI 90–95%).
The “trace” effect of Cerebrolysin persisted until the 12th month of observation at all stages of the disease.
The study also assessed the risk of progression of DE and the occurrence of acute vascular episodes during treatment with Cerebrolysin compared to the control group. The number of patients with a stable condition, with a progressive course and with episodes of exacerbations - the development of TIA and strokes, compared with the control group, was taken into account. The risks of progression of DE and the occurrence of acute vascular episodes (TIA and stroke) during treatment with Cerebrolysin compared to control are presented in Table. 3. The risk of progression and development of complications during DE is calculated using the formula: A/(A+B)/C/(C+D) [4]. As can be seen from table. 3, when treated with Cerebrolysin at various dosage regimens with two courses per year for 10 days, a statistically significant effect of the drug on the progression of the disease in patients with DE stages I, II and III was noted. The odds ratio for progression when treated with Cerebrolysin at a dose of 5 ml/day was 0.1–0.2–0.3 according to the stages of the disease, respectively, and at a dose of 10 ml/day – 0–0.15–0.26 compared with the group control – 0.6–0.6–0.64. The effect of the drug on the occurrence of strokes was equally pronounced: with DE II in the control – 0.13, with treatment with Cerebrolysin at a dose of 5 ml – 0.04, at a dose of 10 ml/day – 0.04. With DE III in the control group, the OR for stroke development was 0.15, with treatment with Cerebrolysin at a dose of 5 ml/day – 0.07, with a dose of 10 ml/day – 0.03. No strokes were observed in stage I DE.
According to the results of the analysis, treatment with Cerebrolysin in the doses used was well tolerated by patients, the percentage of side effects was 2.6% (4 patients).
Pharmacoeconomic analysis
The above calculations took into account direct medical costs (excluding costs for the treatment of concomitant diseases): for inpatient treatment, which includes the cost of bed days, consultations with specialists, examinations and non-drug treatment; and direct non-medical costs. Interhospital differences in rates were not taken into account.
When selecting price parameters, the following sources were used: information bulletin “Medicine (medicines, equipment, , pharmaceutical bulletin”, “Tariffs for medical services provided to the adult population in accordance with the Moscow city compulsory health insurance program.” The above calculations took into account direct medical costs: prices for hospitalization, beds/days in the neurological department, the cost of specialist consultations, the cost of examinations and non-drug treatment; direct non-medical costs. Inter-hospital differences in tariffs were not taken into account. The cost of drug treatment was taken as a single time slice for December 2010 and converted to American dollars at the rate of 1 US dollar = 30.5 rubles. The cost of each unit of the drug (tablet, capsule, bottle, ampoule, etc.) was calculated to determine the costs of drugs in a hospital setting and for outpatient treatment. Then the cost of each drug unit was multiplied by the number of medicinal units used, then the cost of all medicines was added up and divided by the number of patients.
When determining the cost of treatment for patients with different stages of DE included in the main and control groups (without taking into account the costs of treatment of concomitant somatic pathology) per patient (completed case), the following were taken into account: the costs of basic therapy, the costs of treatment that arose when prescribing the “basic therapy" side effects, costs of treatment of TIA, cerebrovascular crises and strokes for the entire observation period; and calculation of direct non-medical costs. The main indicator in all cases was the cost of treatment per patient. The main indicator in all cases was the cost of treatment per patient. Determining the cost of basic therapy in patients of the main and control groups with different stages of DE showed that the average cost of basic therapy was $280.6 US.
The total cost of treatment of DE of different stages, including the cost of consultations, examinations, basic therapy, as well as the cost of treatment of strokes and other vascular episodes that occurred during the observation period, including the cost of direct non-medical costs, was: for DE I – $1315.92 US; with DE II – 1820.0$ US; with DE III – $2044.0 US. Taking into account the possibility of increasing treatment costs as the disease progresses, the given figures should be increased to the following values: for DE I – $2105.4 US; with DE II – 2912.0$ US; with DE III – $3352.2 US.
After calculating the cost of treatment for patients in the control group, it was determined under conditions of treatment with Cerebrolysin. The cost of drug treatment - the cost of basic therapy and Cerebrolysin was equal to $373.6 US for a dosage of 5 ml/day, and $466.6 US for a dosage of 10 ml/day. In table Table 4 shows a calculation of the cost of TIAs and strokes that developed in various subgroups in patients receiving Cerebrolysin.
By summing up all the cost terms, we can calculate the cost of direct medical costs for the treatment of one patient per year when prescribing Cerebrolysin at various dosage regimens (Table 5)
Knowing the cost of indirect medical costs per 1 patient with TIA and stroke per year (for patients in the study group and the control group), which was 35.89 and 634.5 US$, we can calculate the cost of direct medical and non-medical costs per 1 patient per year at treatment with Cerebrolysin (Table 6).
If the cost of disease progression and the development of strokes and other vascular episodes is taken into account, these figures increased.
By summing up the cost of consultations, examinations, basic therapy, the Cerebrolysin drug itself and additional funds required for the treatment of strokes and other complications that arose during observation (including non-medical costs) in patients with various stages of DE, we obtained the following cost indicators of direct medical and non-medical costs of treating one patient per year (Table 7).
Comparative indicators of pharmacoeconomic cost-effectiveness analysis are presented in Table. 8.
It should also be noted that in the study we did not take into account the indirect costs associated with establishing disability, which are many times higher than the medical (direct and indirect) costs of treatment (especially in patients of young, working age). In addition, the costs of rehabilitation treatment for patients with stroke can significantly increase the costs of preventive treatment.
Thus, the study showed that Cerebrolysin in daily doses of 5 and 10 ml for 10 days significantly improves cognitive function and reduces the severity of asthenic syndrome and depression in patients with DE. After completion of the course of treatment, Cerebrolysin has a long-lasting trace effect, lasting up to 3-4 months due to the dosage of the treatment used. The clinical effects of Cerebrolysin are confirmed by the identified significant reduction in the rate of progression of DE, as well as a statistically significant reduction in the risk of developing TIAs and strokes. Cerebrolysin has a low percentage of side effects and is well tolerated, including by patients in older age groups.
A cost-economic analysis showed that the administration of Cerebrolysin and “basic therapy” for all dosage regimens, despite the significant cost of neuroprotective therapy, turned out to be more cost-effective compared to the cost of managing patients who received only “basic therapy” aimed at correcting risk factors development of cerebrovascular pathology, which is associated with a decrease in the rate of progression of the disease and the occurrence of exacerbations during the course of the disease - the development of TIAs and strokes.
Literature
1. Gomazkov O.A. Neurotrophic and growth factors of the brain: regulatory specificity and therapeutic potential. Sat. "Advances in Physiological Sciences". 2005; 36 (2): 1–25. 2. Gusev E.I. Skvortsova V.I. Cerebral ischemia. M.: Medicine, 2001; 248. 3. Oganov R.G. Risk factors and prevention of cardiovascular diseases. G. Quality of life. Medicine. 2003; 2: 10–15. 4. Fletcher R.I. etc. Clinical epidemiology. Fundamentals of evidence-based medicine. M.: 1998; 347. 5. Fritas G.R., Boguslavsky J. Primary prevention of stroke F neurol and psych. Stroke. 2001; Issue 1: 7–21. 6. Chukanova E.I. Encephalopathy. Diss. Doctor of Medical Sciences M.: 2005. 7. Scales, tests and questionnaires in medical rehabilitation. Rukov. for doctors and scientists co-workers / Edited by A.N. Belova and O.N. Shchepetova. M.: Antidor, 2002; 439. 8. Akai F., Hiruma S. Neurotrophic factor-like effect of FPF 1070 on septal cholinergic neurons after transections of fimbria-fornix in the rat brain. Histol Histopathol. 1992; 7:213–221. 9. Albretch E. et al. The effects of Cereblysin on survival and sprouting of neurons from cerebral hemispheres and from the brainstem of chick embryons in vitro. Adv Biosci. 1993; 87:341–2. 10. Alvarez XA et al. Cerebrolysin protects against neurodegeneration induced by -amyloid implants in rats. The international Journal of neuropsycholpharmacology. 2000a; 3:S359. 11. Argentine C., Prencipe M. The Burden of stroke: a need for prevention. In: Prevention of Ischemic Stroke/ Eds.C. Fieschi, M. Fischer. London: Martin Dunitz 2000; 1–5. 12. Bogousslavsky J. On behalf of the European Stroke Initiative. Stroke prevention by the practitioner. Cerebrovasc Dis. 1999; 9:Suppl 4:1–68. 13. Brunner LL Kanter DS Manson JE Primary prevention of stroke. New Eng J Med. 1995; 333:1392–1400. 14. Goldstein LB, Adams R, Becker K et al. Primary prevention of ischemic stroke: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke. 2001; 32: 280–299. 15. Leppala JM, Virtamo J, Fogelholm R, et al. Different risk factors for different stroke subtypes. Stroke. 1999; 30:2535–2540. 16. Plum F. Neuroprotection in acute ischemic stroke. JAMA. 2001; 285:1–4.