Varieties
Sensitivity disorders are divided into two groups - increased or decreased.
Reduced ones include analgesia, hypoesthesia, and termanesthesia. With analgesia, a person does not feel pain; it can occur in many diseases and injuries of the nervous system. Hypoesthesia is manifested by a decrease in tactile sensitivity; the patient does not respond to skin punctures or insects crawling on the body. Thermaneesthesia is characterized by a violation of the perception of temperature conditions (warm and cold influences).
Increased sensitivity distinguishes terms such as hyperalgesia, hyperesthesia and hyperpathia. Hyperalgesia is a pathologically increased perception of pain; sharp or increased perception of stimuli is called hyperpathy. In this condition, the unpleasant sensations continue for quite a long time, the patient cannot determine the exact location and the sensations of irritation continue longer than contact with the irritant occurs. Hyperesthesia is an increased perception of stimuli, but at the same time the patient is able to sense the correct location of the stimulus and what type of impact.
Disorders in which the patient perceives a single effect as multiple are called polyesthesia. Allocheiria is a condition in which the patient feels irritation not at the site of its impact, but in the same areas on the opposite side of the body. With dysesthesia, there is a perverted perception of stimuli, that is, their confusion. When exposed to pain, the patient may feel warmth; when exposed to low temperatures, a tingling sensation. Paresthesia is a spontaneously occurring and short-term sensation of numbness, burning and a feeling of “crawling sensations”.
Clinical diagnostics in neurology
1.9. Peripheral variant of sensitivity disorders
A variant of sensitivity disorder is understood as a set of sensory disorders of a certain type and their localization when the sensory pathway is damaged at various levels. It is customary to distinguish the following types of sensory disorders: peripheral, spinal, cerebral and functional.
Rice. 1.3.
Distribution of skin sensitivity according to peripheral nerves (according to P. Duus)
The listed options, with the exception of the functional one, can, in turn, be divided by localization into several types, and some types (for example, the conductive cerebral type) into subtypes.
The peripheral variant is characterized by sensitivity disorders that occur when sensory pathways within the peripheral nervous system are damaged (peripheral nerves, plexuses, roots) (Fig. 1.3).
Types of Peripheral Sensory Disorders
1. Neural type of sensitivity disorders.
Occurs when sensory or mixed nerves (its main trunk or sensory branches) are damaged. Sensory disorders in neuritis (inflammatory processes) and neuropathies - non-inflammatory lesions (compression-ischemic, traumatic, toxic, etc. - see Chapter 11) do not fundamentally differ in the topical localization of sensory disorders and are characterized by the following main features:
— sensitivity disorders may have the nature of symptoms of irritation (pain, paresthesia, hyperpathia, pain in the nerve trunk during palpation, positive symptoms of tension, pain at the nerve exit points) and (or) symptoms of loss (anesthesia, hypoesthesia, etc.);
— symptoms of prolapse and irritation are most pronounced in the zone of autonomous innervation. Symptoms of irritation often predominate. It should be taken into account that in some pain syndromes (for example, at the repercussion stage of causalgia), pain can also occur outside the zone of innervation of the affected nerve;
— for pain due to nerve irritation, a special character is typical: shooting, burning, “tearing”, caused or intensified by palpation or tension of the nerve, they are accompanied by pronounced vegetative-trophic disorders. Such pain in combination with other symptoms of irritation without symptoms of prolapse determine the clinical picture of neuralgia, and the presence of symptoms of prolapse (in combination with or without symptoms of irritation) already suggests neuritis (neuropathy).
- the pathological process leading to the neural type of sensory disorders may be limited to one or involve several nerves (mono-, multi-, multiple neuritis or neuropathies - see subsection 2.16).
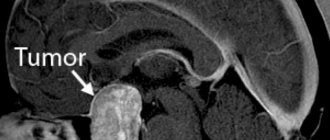
The main causes of neuralgia are irritation of the nerve due to its partial compression, which is most often caused by tunnel syndrome - compression of the affected nerve in the bone or fibrous canal (trigeminal neuralgia, etc.), as well as other local pathological processes (tumors, metastases, hematomas, adhesions and etc.).
The development of neuropathies with predominantly sensory disorders is observed with a concussion of the nerve (neuropraxia), as well as with some tunnel neuropathies and reflex-dystrophic syndromes (causalgia). In other forms of the above pathology of mixed nerves, sensory disorders are also observed, but they are usually combined with the neural type of movement disorders or are significantly inferior to the latter in severity.
2. Polyneuritic type of sensitivity disorders.
It occurs as a result of inflammatory (polyneuritis) or non-inflammatory (polyneuropathy) damage to predominantly distal parts of the peripheral nerves. Sensitivity disorders are characterized by the following symptoms:
- localization mainly in the distal parts of the extremities like “gloves” and (or) “socks”, symmetry, lack of a clear boundary of sensory disorders;
- among sensory disorders, symptoms of irritation may be observed - pain, paresthesia, hyperesthesia, hyperpathia, pain in the nerve trunks during palpation and tension and (or) symptoms of loss - hypoesthesia, anesthesia;
— symptoms of loss and (or) irritation affect, as a rule, all types of sensitivity, although their severity may vary depending on the nature of the pathological process and the stage of the disease;
- specific symptoms are often identified that arise as a result of deep sensitivity disorders: in the legs - sensitive ataxia, in the arms - pseudoathetosis and (or) false astereognosis;
— the above-described sensitivity disorders are often combined with vegetative-trophic disorders of predominantly distal localization.
The presence and nature of sensory disorders, as well as their severity, are determined primarily by the etiological factors of polyneuritis or polyneuropathy. Polyneuritis with a purely sensory variant of the polyneuritic syndrome is significantly more common only in tuberculosis, early neurosyphilis, and typhus. Polyneuropathies with predominantly sensory disorders include: alcoholic, diabetic, as well as polyneuropathies due to folic acid deficiency, endocrine diseases (hypothyroidism, pituitary pathology), drug intoxication (isoniazid, PAS, etc.), tumors of internal organs. Acute inflammatory demyelinating polyradiculoneuropathy Guillain-Barré may begin with polyneuritic sensory disorders, although motor polyneuritic disorders subsequently develop and predominate.
3. Radicular type of sensitivity disorders.
This type of peripheral variant is characterized by a violation of all types of sensitivity and radicular pain in the form of stripes, which are transverse on the body and longitudinal on the limbs (Fig. 1.4).
Rice. 1.4.
Segmental innervation of the skin (according to Hansen-Schliack)
They can occur with pathology of the dorsal root, the Babinsky-Nageotte radicular nerve (part of the root from the dura mater to the spinal ganglion), the spinal ganglion, the spinal cord of Sicard
(formed as a result of the fusion of the motor and sensory roots). The etiological factors of their damage are varied: infectious-toxic, infectious-allergic, compression-ischemic, traumatic, toxic, dysmetabolic, hereditary (see subsection 11.4).
Among them, the dominant one in frequency is the pathology of the spinal cord of a non-inflammatory nature (funiculopathy), which in the domestic literature is traditionally referred to as radiculitis. The clinical picture of radicular syndrome is characterized by the following symptoms:
- radicular sensitivity disorders, radicular pain and paresthesia in the area of the corresponding dermatome;
- symptoms of root tension in combination with reactive pain;
— muscular-tonic syndromes;
- local pain in the area where the roots exit the intervertebral foramina (Vallée's point);
- a combination of radicular sensory and radicular motor disorders of varying severity;
- when the spinal ganglion is involved in the pathological process (herpetic ganglionitis), the above clinical symptoms characteristic of the radicular type of sensitivity disorders are supplemented by herpetic rashes.
When establishing the nosology of the radicular type of sensory disorders, it should be borne in mind that in most cases various vertebrogenic pathologies can lead to its development:
- vertebrogenic pathology, predominantly of a degenerative-dystrophic nature (the main ones are pathology of the intervertebral discs, spondylosis deformans, spondyloarthrosis, ligamentosis ossificans, narrow spinal canal syndrome);
- inflammatory lesions of the vertebral bodies (purulent spondylitis, tuberculous, brucellosis, fungal, etc.);
- tumors of the vertebral bodies (primary benign and malignant, metastatic tumors, myeloma);
- developmental anomalies of the spine ( spina bifida
, additional cervical vertebra, anomalies of the craniovertebral junction, etc.);
- spinal dysplasia (fibrous dysplasia, Scheuermann-Mau disease, Paget disease, achondroplasia, spondyloepiphyseal dysplasia);
- endocrine-metabolic osteodystrophy (more often with hyperparathyroidism, hypothyroidism, diabetes mellitus);
- traumatic lesions of the spine (soft tissue bruise, sprain, ligament rupture, fractures of bodies, arches, processes, traumatic hernias).
In contrast to radicular syndromes of the lumbosacral and cervical regions, thoracic radicular syndromes are extremely rarely the result of degenerative processes in the thoracic spine. The development of radicular thoracalgia is usually associated with inflammatory (spondylitis), systemic (Bechterew's disease) and metastatic lesions. It should also be taken into account that radicular pain at the cervical and thoracic level may be of a reflected nature due to pathology of the thoracic or abdominal organs.
Sources
- Beck C.T. Effects of Fourth-Degree Perineal Lacerations on Women's Physical and Mental Health. // J Obstet Gynecol Neonatal Nurs - 2021 - Vol50 - N2 - p.133-142; PMID:33472041
- Mboua Batoum V., Ngo Um Meka E., Essiben F., Robinson M.E. Perineal body length and prevention of perineal lacerations during delivery in Cameronian primigravid patients. // Int J Gynaecol Obstet - 2021 - Vol - NNULL - p.; PMID:33404071
- El-Shafaey ES. Reconstruction of third-degree perineal lacerations in female camels (Camelus dromedarius) using a modified Goetz one-stage repair technique. // J Vet Med Sci - 2021 - Vol83 - N2 - p.195-200; PMID:33116026
- Ochiai AM., Araújo NM., Moraes SDTA., Caroci-Becker A., Sparvoli LG., Teixeira TT., Carvalho RR. The use of non-surgical glue to repair perineal first-degree lacerations in normal birth: A non-inferiority randomized trial. // Women Birth - 2021 - Vol - NNULL - p.; PMID:33071207
- Rocha BDD., Zamberlan C., Pivetta HMF., Santos BZ., Antunes BS. Upright positions in childbirth and the prevention of perineal lacerations: a systematic review and meta-analysis. // Rev Esc Enferm USP - 2021 - Vol54 - NNULL - p.e03610; PMID:32935765
- Hawkins NN., Lamon AM., Li YJ., Grotegut C., Habib AS. Analgesic use after vaginal delivery in women with perineal lacerations: a retrospective cohort study. // Curr Med Res Opin - 2020 - Vol36 - N6 - p.1009-1013; PMID:32268793
- Romina S., Ramezani F., Falah N., Mafi M., Ranjkesh F. Effect of Perineal Massage with Ostrich Oil on the Episiotomy and Lacerations in NULliparous Women: A Randomized Controlled Clinical Trial. // Iran J Nurs Midwifery Res - 2021 - Vol25 - N2 - p.134-138; PMID:32195159
- Nygaard CC., Tsiapakidou S., Pape J., Falconi G., Betschart C., Pergialiotis V., Doumouchtsis SK. Appraisal of clinical practice guidelines on the management of obstetric perineal lacerations and care using the AGREE II instrument. // Eur J Obstet Gynecol Reprod Biol - 2021 - Vol247 - NNULL - p.66-72; PMID:32070848
- Frietman SK., Compagnie E., Stout TAE., Jonker FH., Ter Braake F. Single-stage reconstruction of third-degree perineal lacerations in horses under general anesthesia: Utrecht repair method. // Vet Surg - 2021 - Vol48 - N7 - p.1299-1308; PMID:31282055
Numbness on the left and right sides of the body: what are the differences?
Numbness of the right arm or leg, simultaneous or sequential, occurs with osteochondrosis, scoliosis, herniated intervertebral discs, when the blood supply to tissues and the conductivity of nerve endings are disrupted. If this syndrome was preceded by a sensitive acute headache or injury, the cause may be much more serious - a stroke or a brain tumor.
When a sensitivity disorder is observed on the left side of the body, a person feels a tingling sensation, and the motor functions of the limbs suffer. If at the same time the facial muscles go numb, blood pressure rises, and dizziness appears, this suggests an ischemic or hemorrhagic stroke or serious pathologies of cerebral circulation. Therefore, numbness on the left is considered a more dangerous symptom than on the right.