Find out more information about neurological diseases starting with the letter “F”: Phakomatoses; Phantom pain; Fibromyalgia; Focal cortical dysplasia; Focal epilepsy; Funicular myelosis.
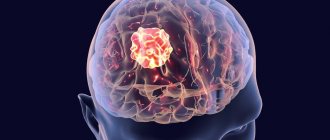
Focal epilepsy: what is it?
This pathology is characterized by epileptic seizures caused by a clearly localized limited zone of increased paroxysmal activity. Most often they are secondary in nature. Paroxysms can be partial complex or simple. The clinical picture depends on the location. Diagnosed by clinical data. EEG and MRI are also indicated. Therapy includes antiepileptic drugs and treatment of the primary disease. According to indications, resection of the epi-zone is possible.
What can trigger a seizure in a patient with epilepsy?
Seizures usually occur without antecedent factors (randomly) and are completely unpredictable. However, some patients notice certain conditions that may trigger attacks. After identifying provoking factors, measures can be taken to avoid them, which will help reduce the frequency of epileptic seizures in the future. Examples of factors that trigger attacks in some patients include flashing lights, sleep restriction, stressful situations, and the use of alcohol or certain medications.
Women with epilepsy often report an increase in the frequency of seizures during menstruation, which is likely due to hormonal changes and fluid retention.
general information
Focal epilepsy refers to all cases of epileptic paroxysms if they arise due to a local focus of increased epi-activity in cerebral structures. The source of excitation begins focally. Gradually spreads to the surrounding brain tissue. This provokes secondary generalization of the attack. It should be differentiated from paroxysms of unrealized epilepsy with a primary diffuse nature of excitation. There is a multifocal form. It is distinguished by the presence of several local zones of excitation.
FE accounts for approximately 82% of all epileptic syndromes. In 75% of cases, the onset occurs in childhood. Most often, the root cause is a violation of brain development of infectious, traumatic or ischemic origin. Such secondary focal epilepsy appears in 71% of patients.
ONGOING SEIZURES.
Generalized status epilepticus.
- Status of generalized tonic-clonic seizures
- Status of clonic seizures
- Absence status
- Tonic seizure status
- Myoclonic seizure status
Focal status epilepticus
- Kozhevnikovskaya epilepsy
- Continued aura
- Status of limbic seizures (psychomotor status)
- Hemiconvulsive status with hemiparesis
Etiology and mechanism of development
Etiological factors include:
- Traumatic brain injuries.
- Malformations of the brain. These include: congenital cerebral cysts, cortical dysplasia, arteriovenous malformations.
- Infections: abscess, encephalitis, neurosyphilis, cysticercosis.
- Genetically determined or acquired metabolic disorders of neurons in a certain area of the cerebral cortex. It is not accompanied by morphological changes.
- In children, perinatal lesions of the central nervous system predominate. These are intracranial birth trauma, fetal hypoxia, asphyxia of the newborn, intrauterine infections.
- Early onset in childhood is associated with impaired cortical maturation. Such epilepsy is temporary and age-dependent.
The pathogenesis of FE is associated with an epileptogenic focus, which has several zones. The area of damage corresponds to the localization of the morphological change. Most often visualized using magnetic resonance imaging. The primary zone is the area that generates epi-excitation. The area of the cortex, the epi-activity of which leads to an attack, is the symptomogenic zone. The irritative region generates epi-activity during the interictal period. Excitation is recorded on the EEG. The zone of functional deficit is the area responsible for concomitant neurological disorders.
Classification
There are three forms of focal epilepsy:
- Idiopathic. Develops against the background of absence of changes in the central nervous system. It is caused by genetically determined membrane and channelopathies, disorders of the maturation of the cerebral cortex. This pathology is benign. These are Panagiotopoulos syndrome, Rolandic epilepsy, Gastaut childhood occipital epilepsy and infantile episyndromes.
- Sympathetic. It is characterized by the presence of a cause. Morphological changes in most cases are visualized on tomography.
- Cryptogenic. It is secondary in nature, but morphological changes are not detected by neuroimaging. Another name for this type of FE is probably sympathetic.
Characteristic symptoms
The leading symptom complex is represented by repeated partial epileptic paroxysms. It is divided into:
- Simple, i.e. without loss of consciousness. There are motor, sensory, somatosensory, autonomic, with mental disorders or with hallucinations. The hallucinatory component is represented by visual, auditory, olfactory or taste disturbances.
- Complex ones with loss of consciousness can be supplemented by automatisms. During an attack there is confusion.
In epi-attacks, secondary generalization is possible. It starts out as complex or simple focal. As arousal occurs, it diffuses to other parts of the cortex. The paroxysm takes on a clonic-tonic character. One patient may have attacks of different forms.
Symptomatic FE is accompanied by additional clinical manifestations. They correspond to the underlying brain lesion. Leads to mental retardation, cognitive impairment, and decreased intelligence in children. Idiopathic FE is benign. It is not characterized by neurological deficits and intellectual and mental disorders.
SELF-TERMINATED SEIZURES
Generalized.
- Tonic-clonic (including variants of the onset from the clonic or myoclonic phase)
- Clonic (with or without a slight tonic component)
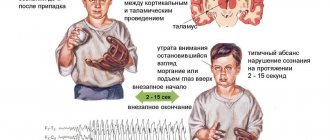
- Typical absence seizures
- Atypical absence seizures
- Myoclonic absence seizures
- Tonic
- Epileptic spasms
- Epileptic myoclonus
- Eyelid myoclonus (with or without absence seizures)
- Myoclonic – atonic (myatonic)
- Negative myoclonus
- Atonic
- Reflex generalized
Focal.
- Focal sensory (with simple symptoms associated with irritation of the occipital or parietal lobe or with complex symptoms associated with irritation of the temporo-parietal-occipital cortex)
- Focal motor: clonic, asymmetric tonic (associated with irritation of the additional motor area), with typical automatisms, with hyperkinetic automatisms, with focal negative myoclonus, inhibitory
- Gelastic
- Hemiclonic
- Secondary – generalized
- Reflex focal
Clinical picture depending on location
- Parietal. This is the rarest variant of epi-focus localization. Damage occurs with cortical dysplasia and tumors. Accompanied by simple somatosensory paroxysms. At the end of the attack, Todd's palsy or short-term aphasia may occur. If the focus of excitation is in the postcentral gyrus, Jacksonian seizures occur.
- Paroxysms in the occipital lobe are accompanied by visual impairment. Most often these are visual hallucinations lasting up to 13 minutes. Possible: narrowing of visual fields, transient amaurosis, illusions, hiccup blinking.
- A lesion in the frontal lobe causes short-term stereotypic paroxysms. They tend to be serial. No aura is noted. Unusual motor phenomena are characteristic: pedaling, complex automatic gestures, turning the head and eyes. Accompanied by emotional symptoms - agitation, screaming, aggression. Localization in the pericentral gyrus gives rise to Jacksonian epilepsy with movement disorders. In most patients, attacks occur during sleep.
- The temporal lobe is the most common location of the epileptogenic focus. Characterized by sensorimotor seizures with loss of consciousness, aura and automatism. The duration of the attack is on average 30-60 minutes. Children are characterized by oral automatisms, while adults - gestural ones. In 50% of cases, epileptic seizures have secondary generalization. If the dominant hemisphere is affected, post-ictal aphasia occurs.
Diagnostics
A patient with a first-time partial attack should be carefully examined. It is necessary to exclude cerebral pathologies: vascular malformations, tumors, cortical dysplasia. The neurologist collects anamnesis. Finds out the frequency, sequence, duration of an epileptic attack. Clarifies the neurological status. With the symptomatic nature of FE, it helps to establish the approximate localization of the source of excitation.
Instrumental diagnostics include:
- Electroencephalography. This form of epilepsy is recorded even during the interictal period. If the information content of a regular EEG is low, an examination with provocative tests and testing at the time of an attack is indicated.
- Subdural corticography allows you to establish the exact localization of the affected area.
- MRI helps to identify the morphological substrate. To diagnose the slightest structural changes, a minimum thickness of sections is required. With symptomatic FE, it is possible to establish the underlying disease and note dysplastic transformations. If there are no abnormalities during magnetic resonance imaging, cryptogenic or idiopathic focal epilepsy is diagnosed.
- PET of the brain helps to identify the area of hypometabolism in cerebral tissue corresponding to the lesion.
- Area SPECT examines the area of hyperdiffusion during attacks and hypoperfusion in the interictal period.
DISCUSSION (K.Yu. Mukhin).
Replacing the definition of “cryptogenic forms” with “probably symptomatic forms”. In the definition of syndromes, replace the word “convulsions” with “attacks”. The concept of “seizures” is much broader than “convulsions”, and not all seizures manifest themselves as convulsions. For example, it is more accurate to call the syndrome “benign infantile seizures” rather than “benign infantile seizures,” since the disease does not necessarily involve seizures. The term “partial seizures and partial epilepsies” has been replaced by “focal seizures and focal epilepsies.” The division of focal seizures into simple and complex, depending on the impairment of the level of consciousness, has been abolished. This is due to the fact that in most cases the doctor is not able to test the patient’s consciousness in detail during an attack, and therefore the assessment of the level of consciousness is always very tentative. The classification raises many questions, in particular, the classification of attacks such as atonic, atypical absences and spasms exclusively as generalized. In most cases, these attacks have a focal onset, and they are often based on the phenomenon of secondary bilateral synchronization. The classification of epileptic syndromes does not include pseudolennox syndrome, which is more common in pediatric practice than Lennox–Gastaut syndrome.
Therapy
A neurologist or epileptologist should prescribe treatment for the disease. The therapy is long-term and requires constant use of anticonvulsants. These are drugs valproic acid, carbamazepine, topiramate, phenobarbital, levetiracetam. If FE is symptomatic, the main thing is to eliminate the root cause. Taking medications is most effective for parietal and occipital epilepsy. When the pathology is localized in the temporal regions, after 1-2 goals the patient develops resistance to anticonvulsants. If conservative treatment does not bring results, the question of surgery may arise. They are performed by neurosurgeons. There are several intervention options:
- Resection of the epileptogenic area. It is advisable to operate on the patient only if FE is well localized.
- Removal of focal formation. These may be malformations, cysts or tumors.
- Extended resection is indicated if individual cells adjacent to the epileptogenic area also become a source of epi-activity.
To clarify the individual structure of the cortex, corticography is performed.
Medical prognosis
The prognosis of the disease depends primarily on its type. In symptomatic epilepsy, cerebral disorders have the greatest impact. If there are severe brain malformations and tumors, the prognosis is threatening. This type of epilepsy in children is complicated by mental retardation. Its severity depends on the age at which the disease debuted. With idiopathic PE, the prognosis is favorable. In most cases, it occurs without the appearance of cognitive pathologies. Spontaneous cessation of paroxysms in adolescence is possible.
With surgical intervention, in 60-70% of patients, epileptic seizures disappear or occur much less frequently. In the long-term period, stable remission is possible in 30% of patients.
Epilepsy in children and adolescents is the most important socio-medical problem of our time. Despite the wide range of available antiepileptic drugs (AEDs), seizures continue in more than 25% of children with epilepsy [30]. Traditional AEDs are not always effective enough [56]. Therefore, a large number of works have now appeared in the literature on the therapeutic effectiveness of new AEDs [36].
In the treatment of focal forms of epilepsy, AEDs of different generations are used. In 1912, the first anticonvulsant drug phenobarbital was synthesized, which remained the only AED on the pharmaceutical market for more than 30 years. Since the 60s, it has been the first and second choice drug for various types of epileptic seizures. However, its use in children is currently limited due to its pronounced sedative effect [50]. Nevertheless, phenobarbital still occupies a certain place in the treatment of children with epilepsy, especially at an early age [24]. Phenobarbital is used for all forms of epilepsy accompanied by generalized seizures [35]. It is more effective for simple partial seizures and less effective for complex partial seizures. It should not be prescribed for absence seizures, myoclonic-astatic seizures and West syndrome. Phenobarbital is often prescribed for neonatal seizures [19, 21, 29], with the exception of use in children born weighing less than 1800 grams [65], as well as for typical febrile seizures [46, 51]. It is a second-line drug for the relief of status epilepticus [43, 60]. Valproate and carbamazepine are also widely used in the treatment of epilepsy in children.
In the treatment of focal forms of epilepsy in childhood, new generation AEDs are often used - topiramate (Topamax, Janssen-Silag) and lamotrigine (Lamictal, GlaxoSmithKlain). It should be noted that these drugs have appeared on the domestic pharmaceutical market since the 90s and are used in pediatric practice when traditional AEDs are ineffective and, as a rule, in combination with them [48].
Topiramate (Topamax) is a new highly effective drug with a wide therapeutic spectrum [17, 41]. It belongs to the class of sulfamate-substituted monosaccharides and has a complex mechanism of action [18, 37]. Topiramate is indicated for partial and generalized seizures, both in monotherapy and in combination with other AEDs [39]. It is used in the treatment of seizures associated with Lennox-Gastaut syndrome [38, 40] and West syndrome [14, 57], and can be prescribed to adults and children with newly diagnosed epilepsy.
Lamotrigine (Lamictal) is a broad-spectrum drug for the treatment of all types of seizures [10, 12, 26], with the exception of myoclonic ones [22]. It is recommended for focal and generalized, idiopathic and symptomatic epileptic syndromes in adults and children [59]. Lamotrigine prevents the effect of secondary seizure generalization by inhibiting the diffuse spread of epileptiform activity [10]. It is also the drug of choice in the treatment of Lennox-Gastaut syndrome [42], West syndrome [13], and Angelman syndrome [25].
The purpose of this study was to analyze the effectiveness of AEDs of different pharmacological groups in the treatment of focal forms of epilepsy in children in a city epileptology center.
Material and methods
The study included 96 patients, 55 (57%) boys and 41 (43%) girls, with a verified diagnosis: symptomatic focal epilepsy or presumably symptomatic (cryptogenic) focal epilepsy. The age of the patients varied from 1 month to 17 years. Patients were observed from the age of 6 months to 4 years 6 months.
The diagnosis of epilepsy and determination of the nature of seizures were carried out in accordance with the International Classification of Epilepsy, Epileptic Syndromes and Related Diseases (New Delhi, 1989).
In each case, a detailed collection of anamnestic data was carried out and the neurological status was assessed.
EEG was recorded over time (in some cases, video-EEG monitoring was performed including the sleep period). The study was carried out according to the standard 10-20 method on a 19-channel Neuron-spectrum device (Ivanovo) or an Encephalan-131-03 device, modification 11, (Taganrog). Neuroimaging included computed tomography of the brain or MRI on 0.5-1.5 Tesla tomographs. General and biochemical blood tests were also monitored to exclude side effects of therapy.
The main reasons for including patients in the study were the lack or loss of effect from previous therapy and the persistence of attacks, as well as the occurrence of undesirable side effects when using traditional AEDs; in isolated cases, new AEDs were used in initial monotherapy.
According to the recommendations of the International League Against Epilepsy (1998), in recent years restrictions have been introduced on the use of phenobarbital in childhood due to possible side effects on the development of cognitive functions in children. Therefore, the source of information about patients receiving phenobarbital was the medical records of inpatients treated for epilepsy in a neurological clinic in 2000-2005. They made up the 1st group of patients. This group included 34 patients aged from 1 month to 11 years 9 months. In 94% of cases, phenobarbital was used as initial monotherapy. Subsequently, 18% of patients received combination therapy with phenobarbital and other AEDs. Doses of the drug in the study ranged from 12 to 300 mg per day, with an average of about 170 mg per day. Per kilogram of body weight, doses of phenobarbital were prescribed in wide therapeutic ranges from 1.5 to 12 mg/kg per day, averaging 6.4 mg/kg per day. The 2nd group of patients consisted of 31 patients aged from 24 months to 16 years and received topiramate therapy. In 12 (39%) patients, the drug was used as starting or alternative monotherapy. Topiramate was prescribed in combination with one AED to 13 (42%) patients. Combination therapy of topiramate with 2 AEDs was performed in 6 (19%) patients. Doses of the drug in the study ranged from 56 to 500 mg per day, averaging about 165 mg per day. Per kilogram of body weight, doses of topiramate were prescribed in wide therapeutic ranges from 2.8 to 17 mg/kg per day, with an average of 6.6 mg/kg per day.
Group 3 patients were treated with lamotrigine. It was used in 31 patients ranging in age from 1 year 10 months to 17 years. In all cases, the drug was prescribed as additional therapy to one or two other AEDs. During treatment, 3 (10%) patients were switched to alternative monotherapy with this drug. Lamotrigine was prescribed in doses ranging from 25 to 250 mg per day, with an average of 116 mg per day. Based on the amount of drug per child's body weight, doses varied in the range from 0.5 to 6 mg/kg per day, averaging 3.6 mg/kg per day. In all three groups, drug titration was carried out according to generally accepted recommendations for drug administration.
The general characteristics of patients in each group are given in Table. 1.
The clinical criterion for the effectiveness of therapy is the cessation of seizures or a change in their frequency during antiepileptic therapy. Therefore, the result was assessed by the effect on the frequency of attacks according to standard criteria: complete clinical remission (100% relief of attacks for 12 months or more); reduction in the frequency of attacks by 50% or more; reduction in the frequency of attacks by less than 50% or no effect; aggravation of attacks. The impact of the studied AEDs after their introduction on the quality of attacks was assessed: their nature, duration and intensity.
results
In each group, the majority were children with symptomatic focal forms of epilepsy - 77, 85 and 86% of cases. Accordingly, the proportion of patients with cryptogenic focal forms of epilepsy was significantly smaller - 23, 15 and 14%, respectively. In all three groups, symptomatic focal frontal lobe epilepsy was more often detected - 20, 26, 39%; multifocal epilepsy - 12, 19, 22.5%. Since before 2005 there was no technical ability to conduct EEG monitoring, in the group of patients treated with phenobarbital, a non-localized form of epilepsy was diagnosed in 35% of cases.
Analyzing and comparing the history of the development of the disease, it was revealed that epilepsy most often debuted before the age of 7 years and, on average across groups, the onset was at the age of: 3 years 11 months in the 1st group of patients receiving phenobarbital; 3 years 1 month in the 2nd group receiving Topamax; 4 years 6 months in the 3rd group receiving Lamictal. It has been reliably proven that an earlier onset of the disease was detected in children (p <0.01) whose mothers had aggravating factors during pregnancy (threatened miscarriage, intrauterine infections) and pathology during childbirth. The earlier onset of epilepsy was in the group of patients with pronounced focal disorders in the neurological status (p<0.05) and with severe developmental delay in the first year of life (p<0.05).
Patients receiving phenobarbital had the shortest disease duration from the onset of seizures to the start of taking the drug - on average 1 month 24 days, and in 94% of patients phenobarbital was the first drug in the treatment of epilepsy; 6% of patients switched to phenobarbital after unsuccessful treatment with other AEDs.
The disease history looked different in the other two groups. In the group of patients taking topiramate, the average duration of illness before inclusion of the drug in the treatment protocol was 4 years 8 months, and almost all patients (94%) had already received previous therapy with other AEDs. In 61% of cases, combination antiepileptic therapy was used. In the group of patients taking lamotrigine, the average duration of the disease was 5 years 2 months and all patients also had previous antiepileptic therapy before taking the drug. In 90% of cases in the study, lamotrigine was used in combination with other AEDs. It has been statistically proven that the longer the duration of the disease, the more different AEDs were used in the treatment of patients (p <0.05).
In all three groups, the majority of all patients had severe neurological pathology in the form of spastic paresis, pathology of cranial nerve function, cerebellar symptoms, mental retardation - from 71 to 87% of patients. Consequently, a delay in the development of children in the first year of life was observed in 65-76% of patients (see Table 1). Analyzing the observed seizures, it was revealed that secondary generalized seizures predominated in all groups, which accounted for 40-50% of all types. They were more often recorded in children with an earlier onset of the disease (p <0.01).
When assessing the effectiveness of the studied drugs, results were obtained that are summarized in table. 2.
Complete cessation of attacks when using drugs of the old generation (phenobarbital) and the new generation (Lamictal and Topamax) occurred in the same number of patients in each of the study groups - in 26% of cases. However, there were differences in rates of reduction in seizure frequency of 50% or more. The highest result was obtained in patients taking topiramate - 19 (61%). In patients taking lamotrigine, this figure was slightly lower - 14 (45%) patients. And in only 4 (12%) patients treated with phenobarbital, attacks were reduced by 50% or more. Accordingly, this group had the highest percentage of cases in which the effect was absent or minimal - 21 (62%) patients.
From the data presented it is clear that the most pronounced positive effect in the form of complete relief of attacks or their cessation by 50% or more was achieved in the group of patients receiving topiramate - 87% (27 patients). In the group of patients taking lamotrigine, this figure was 71% (22 patients). And the effect was the smallest in patients treated with phenobarbital - 38% (13 patients). We did not find any significant differences in the registration of positive dynamics on the EEG in all three groups. A decrease in the epileptiform activity index was noted in 8 (24%) patients taking phenobarbital, 8 (26%) patients taking Topamax, and 11 (35%) patients taking Lamictal. The presence of differences in the effectiveness of treatment in the three study groups was statistically confirmed.
Discussion
We compared the results of our study with the data available in the literature. In this regard, we recall that during treatment with phenobarbital, we noted persistent clinical remission or complete cessation of attacks in 26% of cases and a reduction in the frequency of attacks by 50% or more in 12% of patients. Thus, a positive effect was achieved in the overall group in 38% of patients. Low effectiveness of treatment was observed in 62% of patients. Our results correlate with the studies of many authors. In his observation, S.R. Boldyreva [2] notes complete control of seizures in 33% of patients. In the review by O.A. Pylaeva et al. [11] compared the effectiveness and tolerability of barbiturates and valproate in children aged 6 months to 15 years. Valproates were used in doses of 30-50 mg/kg per day, barbiturates - in an average therapeutic dose of 2-5 mg/kg per day. The therapeutic effect in monotherapy was registered in 65% of cases when taking valproate and only in 30% of cases when taking barbiturates. In 75% of cases, the improvement in the patients' condition while taking barbiturates was temporary, and subsequently the frequency of attacks increased again. In the work of A.A. Dautova et al. [5] conducted a comparative analysis of monotherapy for epilepsy with phenobarbital and diphenine in patients with different forms of epilepsy. Phenobarbital was used at an average daily dose of 2.0-2.5 mg/kg per day, and diphenin at a dose of 4-5 mg/kg per day. As a result, attacks stopped in 7 (16%) of 44 people receiving phenobarbital, and in 35 (out of 60) receiving diphenine. In a study by W. Wang et al. [58] included 2455 patients. After 24 months from the start of treatment with phenobarbital, 26.2% of patients were seizure-free and 31.3% of patients had a reduction in seizures of 75% or more.
Meanwhile, some authors note higher efficiency in treatment with phenobarbital. Thus, in a study by D. Pal et al. [45] phenobarbital was used in the treatment of children with different types of seizures at an average therapeutic dose of 3 mg/kg per day, and within 6 months complete clinical remission was achieved in 68% of cases. In the observation of C. Valvi et al. [54] good seizure control was achieved in 84.8% of children treated with phenobarbital. In a study by K. Nimaga et al. [44] phenobarbital was used in the treatment of children at doses of 50 mg/day and in adults at a dose of 200 mg/day. After 1 year from the start of treatment, 80.2% of patients were seizure-free for 5 months. And 15.7% of patients had a significant reduction in seizure frequency. In the work of S. Ismael [31], phenobarbital was used in the treatment of children aged 5 months to 12 years. A good treatment result was observed in 62.4% of children, a reduction in seizures by 50% was registered in 7.69% of children. In a study by N. Thilothammal et al. [52] compared the effectiveness and tolerability of phenobarbital, diphenine and valproic acid preparations. It was shown that the effectiveness of treatment was relatively similar in all three groups.
We have not identified a preferential effect of phenobarbital in relation to different forms of epilepsy and different types of epileptic seizures (p>0.05). There were no significant differences in its effectiveness between symptomatic focal forms and cryptogenic (presumably symptomatic) focal forms of epilepsy (p>0.05). It was found that the duration of the disease before starting phenobarbital also does not affect the effectiveness of therapy. In patients with a long duration of the disease, the effectiveness of treatment was comparable to patients with relatively recent illness (p>0.05). But S. Ismael [31] established the greater effectiveness of phenobarbital in generalized convulsive attacks (a positive effect was noted in 72.6% of patients); it was less effective for focal attacks - 43.75% and for focal attacks with secondary generalization - in 47.05% of patients.
In the group of patients receiving topiramate therapy, complete cessation of attacks was observed in 26% of patients and a decrease in the frequency of attacks by 50% or more was recorded in 61% of patients. We compared our results with those of other authors. In the study by K.Yu. Mukhina et al. [8] complete relief of seizures was noted in 19.5 and 16.5% (36% together, respectively) in patients with symptomatic focal forms of epilepsy. According to H. Bootsma et al. [20], this figure is up to 20% of patients. And in the work of Y. Cho et al. [23] clinical remission was noted in 30.4% of cases. Relatively low efficiency was noted in the study by K. Krakow et al. [34] - only 10% of patients over 12 years of age were completely free from seizures. S. Grosso et al. [27] also noted the cessation of seizures in 13% of patients out of 59 treated children under 2 years of age. In the work of S. Grosso et al. [28] studied the effectiveness of topiramate in children with refractory forms of epilepsy. Seizures were controlled in only 4% of children. On the contrary, a high therapeutic effect was noted in the work of domestic authors. In the observation of K.Yu. Mukhina et al. [7] high clinical efficacy was achieved in 46.5% of patients. A.B. Hecht et al. [4] noted drug remission lasting more than 1 year in 47.8% of patients. K.V. Voronkova et al. [3] recorded complete clinical remission in 48% of patients. In the study by S.R. Boldyreva [2] obtained complete control over attacks in 53% of patients.
A positive effect overall in our study was obtained in 87% of patients. In the work of K.V. Voronkova et al. [3] this figure was 92%. In the work of K. Krakow et al. [34] a good result was observed in 82%. In the observations of other authors, the positive effect of treatment was approximately the same - 58.5-73.2%. Increased frequency of attacks was registered in 3% of patients [2] and in 6% of cases [8], which is comparable to the results of our study - 3%.
Topiramate showed better results in the treatment of patients with cryptogenic focal forms of epilepsy. However, in the work of S. Al Ajlouni et al. [15] did not reveal any difference in the effectiveness of treatment for symptomatic and cryptogenic forms of epilepsy. We noted a positive result in the treatment of multifocal forms of epilepsy - 86% of patients had a complete cessation of seizures or a reduction in their frequency by 50% or more. In the group of patients with focal frontal epilepsy, 6 (75%) showed a reduction in seizures by 50% or more. In only 1 (12.5%) case the attacks stopped completely. In the study by K.Yu. Mukhina et al.[8] a positive effect when taking topiramate in patients with symptomatic frontal lobe epilepsy was observed in 63% of cases. A. Verrotti et al. [57], based on observations of a representative group of patients, also note the effectiveness of topiramate in the treatment of frontal lobe epilepsy in monotherapy.
Topiramate showed greater effectiveness in patients with frequent serial tonic axial spasms that occur during night sleep, with focal hypermotor seizures, as well as with secondary generalized convulsive seizures (p>0.05). Identical effectiveness was noted in their observation by K.Yu. Mukhin et al. [8]: the drug was highly effective against focal motor, tonic and secondary generalized seizures. In some cases, Topamax clearly reduced the frequency of atypical absence seizures. However, in monotherapy, its insufficient effectiveness was noted in myoclonic and automotor seizures. It has been proven that the effectiveness of therapy was higher in patients who had a short history of the disease before inclusion in Topamax therapy (p = 0.006).
In our study, 61% of patients were treated with topiramate in combination with other AEDs. In our observation, combination therapy with topiramate and valproic acid drugs turned out to be the most rational and effective. The literature also provides data on the effectiveness of topiramate in combination therapy with various AEDs. In the work of A. Schreiner et al. [47] used a combination of topiramate with valproic acid preparations. At the end of the study, 70% of patients were switched to Topamax monotherapy at a dose of 150 mg/day. In 51% of patients, the attacks stopped completely; in general, a positive effect was noted in 75% of patients. In comparison, the work of A. Kowalik et al. [33] topiramate has been successfully used in combination therapy with carbamazepine and oxcarbazepine. At the end of the study, 73% of patients were switched to alternative monotherapy with topiramate at a mean dose of 100 mg/day. A positive effect was noted in 91% of patients, of which 62% were completely free of attacks.
In the group of our patients receiving lamotrigine, stable clinical remission was achieved in 26% of cases and a reduction in the frequency of attacks by 50% or more was observed in 45% of children. In 6% of cases, an increase in seizures was observed. Overall, a positive effect was achieved in 71% of patients. Higher efficacy was observed in the group of patients who had a later onset of the disease (p=0.037). On the other hand, children who had a high seizure frequency (p=0.031) and had received prior treatment with multiple antiepileptic drugs (p=0.008) had less treatment benefit.
Similar results were obtained in the work of R. Jain et al. [32]: in 20 children (average age 90 months), lamotrigine was used in combination therapy with valproic acid drugs in an average therapeutic dose of 3.86 mg/kg. A significant positive result was observed in 72% of patients, of which 27.7% of patients had a complete cessation of attacks and 44.4% of patients had a significant reduction in the frequency of attacks by 50% or more. In a study by S. Zubcevic et al. [61] included 61 children who began receiving combination therapy with lamotrigine an average of 16 months after the onset of the disease. In 67.2% of cases, the seizures were focal and secondary generalized convulsive. As a result, a decrease in the frequency of attacks by 75-100% was noted in 37.7% of patients, and by 50-75% in 21.3% of patients. In general, summing up these data, we can indicate a positive effect in treatment in 59% of children. In a study by Ch. Song et al. [49] when using lamotrigine in additional therapy in 114 patients, seizure relief by 50% or more was observed in 57% of patients; subsequently, 22.8% of patients were transferred to monotherapy with this drug. In the publication by M.B. Mironova et al. [6] paid special attention to the use of lamotrigine in additional therapy to valproic acid drugs in 38 patients with various forms of epilepsy aged from 3 to 25 years (average age 14.3 years). A positive effect with the addition of lamotrigine was noted in 73.8% of cases: complete therapeutic remission in 36.9% of cases, a reduction in the frequency of attacks by 50% or more in 26.9% of cases. High efficiency while taking lamotrigine (100% relief of attacks in 54% of patients) was registered by H. Arif et al. [16]. Particular attention to the gender characteristics of the use of lamotrigine was paid to G.N. Avakyan et al. [1], emphasizing the positive effect of the drug on reducing the frequency of attacks.
In our work, lamotrigine showed good results in the treatment of frontal lobe epilepsy: in 58% of patients there was a significant decrease in the frequency of attacks and in 17% of cases the attacks were completely stopped. Lamotrigine showed greater effectiveness in patients with focal motor hemiclonic seizures, as well as in secondary generalized convulsive seizures (p>0.05). N.Yu. Perunova et al. [9] noted the effectiveness of therapy in patients with partial seizures in 8% of cases and with secondary generalized ones in 12% of cases. In their observation, E. Trevathan et al. [53] state the effectiveness of lamotrigine in children with partial seizures, absence seizures, and various types of seizures in Lennox-Gastaut syndrome. In a study by S. Zubcevic et al. [61] Lamotrigine was less effective in partial seizures. According to R. Jain et al. [32], lamotrigine showed a good effect in all types of seizures except myoclonic ones.
In our study, in 90% of cases, lamotrigine was used in combination therapy with other AEDs with high efficiency (p = 0.01). In 52% of cases, a combination of lamotrigine with valproic acid drugs (Depakine) was prescribed. A similar observation was noted in the work of N.Yu. Perunova et al. [9]: during combination therapy with lamotrigine and valproate, a reduction in the frequency of attacks by 50% or more was observed in 48.5% of patients.
Thus, new generation AEDs, having a complex mechanism of action on the processes of epileptogenesis, have shown higher effectiveness in the treatment of focal forms of epilepsy in children. If we take into account that the main goal of pharmacotherapy for epilepsy is the complete cessation of seizures without the appearance of neurological, cognitive and somatic side effects and ensuring educational, professional and social adaptation of patients, then the creation of new broad-spectrum AEDs allows expanding therapeutic options in the treatment of epilepsy, especially focal and pharmacoresistant forms.