Ventriculomegaly is a pathology that affects the ventricles of the brain. The function of these parts of the organs is to maintain intracranial pressure and ensure normal blood circulation to the human cerebral cortex.
Most often, the disease occurs in unborn babies, less often in children of preschool and school age. Ventriculomegaly in adults develops in exceptional cases, since the disease is congenital.
Let's take a closer look at what ventriculomegaly is, the causes of its occurrence and how it is treated.
Causes and prerequisites for the development of ventriculomegaly in the fetus
According to medical research, ventriculomegaly of the lateral ventricles occurs due to the following reasons:
- Hereditary prerequisites. If any of the child’s close relatives (mother, father, siblings/cousins) suffered from a similar disease, the likelihood of its occurrence in the newborn increases to 25% compared to a baby in whom no one in the family had such a disease;
- Ventriculomegaly in the fetus often develops as a side disease along with another disease, such as Down syndrome;
- Pathology is provoked by intrauterine infections, as a result of which the ventricles of the brain enlarge.
General concept of the disease
Ventriculomegaly in the fetus is a pathology characterized by an increase in the size of the cerebral ventricles. Such a change can cause damage to the central and autonomic nervous system, heart and blood vessels.
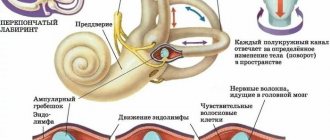
Normally, any person, including a developing fetus, has 4 cerebral ventricles in the brain. Two of them (lateral ones - first and second) are located in the white matter of the brain.
Using the interventricular foramen, the lateral ventricles are connected to the third. It, in turn, has an anatomical connection with the fourth ventricle located in the bottom of the rhomboid fossa.
The entire ventricular system of the brain performs one of the most important functions - it synthesizes cerebrospinal fluid (CSF), which then collects in the fourth ventricle and from there enters the subarachnoid space.
If there are certain disturbances in the outflow of cerebrospinal fluid, then part of it accumulates in the ventricles and causes their expansion, that is, ventriculomegaly. Normally, the size of the ventricles should not be more than 10 mm.
According to statistics, the frequency of ventriculomegaly in the fetus is 0.6%. The pathology is usually diagnosed between 17 and 34 weeks of pregnancy using an ultrasound scan. In case of pathology, fetal death at the time of birth or in utero cannot be ruled out.
Pathology is sometimes detected in adults when performing a computed tomography scan. However, in such cases, ventricular enlargement is normal and does not require treatment.
The course of fetal ventriculomegaly in pregnant women after 35 years
Ventriculomegaly in the fetus most often develops if the child’s mother is over 35 years old. This happens for the following reasons:
- The risk of genetic disorders (for example, Down syndrome) increases;
- Intrauterine infections occur more often;
- A pregnant woman over 35 years of age is susceptible to complications while bearing a child.
Thus, if the mother is under 35 years old, ventriculomegaly in the child occurs only in exceptional cases.
Why is ventriculomegaly dangerous?
Ventriculomegaly in a child can lead to the development of serious disorders in the functioning of the central nervous system and brain. In an isolated form, when the deviation is observed on its own, the prognosis is usually favorable.
Ventriculomegaly, the causes of which are genetic disorders, is often combined with abnormalities in mental development. In particularly severe cases, the child may not be viable. It is important not to skip an ultrasound during pregnancy, when it is already possible to detect many developmental disorders, in particular, ventriculomegaly. What is dangerous about this situation is that by starting the process, you can miss precious time.
Ventriculomegaly, caused by prolonged exposure to infection on the fetus, hypoxia during gestation or childbirth can cause consequences from various kinds of psychoneurological disorders to severe forms of cerebral palsy. Such consequences of ventriculomegaly are difficult to treat. It has its effect, but requires a huge amount of time and effort from doctors and parents.
Diagnosis of lateroventriculoasymmetry of the brain
Ultrasound procedure of a child’s brain
Depending on the age of the patient, various methods for diagnosing pathology are used:
- The disease can be detected in the fetus starting from the 17th week of pregnancy. For diagnosis, the doctor performs an ultrasound of the mother’s abdominal cavity;
- Ventriculomegaly in an infant is confirmed after an ultrasound of the head;
- To diagnose an adult, an MRI of the brain is prescribed.
All procedures are aimed at examining the ventricles of the brain and identifying lateroventriculoasymmetry (violation of ventricular symmetry).
Diagnostics
The first signs of ventriculomegaly in the fetus during pregnancy can be detected at 17-34 weeks during a routine examination and ultrasound.
To confirm the diagnosis, karyotyping of the fetus is prescribed - studying the indicators of the set of chromosomes.
Perinatal diagnostic procedures should consist of those examinations that will help study all the anatomical systems of the fetus, especially the brain.
If dilation of the cerebral ventricles is suspected, a transverse scan of the fetal head is required to determine the size of the lateral cerebral ventricles.
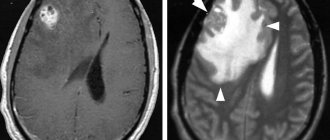
Echography is also prescribed; during its implementation, the accuracy of detecting ventriculomegaly reaches 80% of cases. After birth, the child may be prescribed a CT scan or MRI - computer scans that examine the structures of the brain layer by layer.
The diagnosis is made only after evaluating all the data obtained during the examination. In approximately 9% of cases, the diagnosis gives false results.
Severity of ventriculomegaly of the lateral ventricles
Doctors distinguish three degrees of severity of pathology:
- First: an increase in the ventricles of the brain to 11-12 mm. Patients are diagnosed with “ventriculodilation” - a slight expansion of the ventricles of the brain in newborns and preschool children;
- Second: enlargement of the ventricles up to 15 mm. Against this background, asymmetry of the lateral ventricles of the brain and impaired blood flow to the affected areas are often observed;
- Third: enlargement of the ventricles up to 20 mm. At this stage, irreversible changes occur in the structure of the brain.
In addition, the child may be diagnosed with “borderline ventriculomegaly,” which means an increase in the lateral ventricles by no more than 9 mm.
Ventriculomegaly 1st degree
At the first stage of development of the disease, there are no pronounced symptoms. Only a neurologist can detect it after diagnosis. Most parents notice that the child becomes excitable and irritable. Unfortunately, no other symptoms appear.
Moderate ventriculomegaly
The second stage of the disease is also called “moderate ventriculomegaly.” As a rule, it is combined with other ailments, for example, ventriculomegaly and agenesis of the corpus callosum often occur together. Also in this case, lateroventriculoasymmetry of the brain (asymmetry of the ventricles) occurs. The following symptoms are also observed:
- Periodic convulsions, similar to epileptic seizures;
- Increase in head size;
- The presence of bulging veins on the forehead;
- Slow physical development;
- Mental retardation.
Severe ventriculomegaly
In addition to abnormal expansion of the ventricles of the brain, the following symptoms are present:
- Increased intracranial pressure due to the asymmetric shape of the ventricles;
- Recurrent headaches;
- Speech disorders.
Additional diseases are often added to the pathology: cerebral palsy, Down syndrome or hydrocephalus.
Ventriculomegaly in a child: what is it? Causes, signs, treatment, consequences, reviews
Ventriculomegaly is an enlargement of the ventricles of the brain.
The diagnosis is made based on the results of an ultrasound examination. The risk of consequences for the child is determined by the degree of enlargement and the presence of other neurological abnormalities. In this article: The term ventriculomegaly refers to a slight enlargement (dilatation) of the ventricles with a diameter of 10 mm or more. Prevalence: 0.5-1.5 per 1000 births (according to other sources, 1:500), on average, about 1% of children have this condition at some point in life. The most common cause of ventriculomegaly is a change in the structure of brain tissue due to damage or developmental abnormalities.
Brief dictionary:
- Ventricles are cavities in the structure of the brain filled with CSF (cerebrospinal fluid).
- CSF or cerebrospinal fluid is a liquid substance produced by the choroid plexuses of the ventricles, serves to cushion and regulate the environment in the empty (unfilled with cells) space, demarcates the brain and spinal cord from the hard bone membranes.
In ventriculomegaly, cerebrospinal fluid accumulates in the ventricular system of the brain due to increased production or impaired outflow. It is important to classify ventriculomegaly into types depending on concomitant findings on NSG or MRI:
- isolated - an independent anomaly, not combined with other developmental defects;
- associated - accompanies other pathologies of the nervous system.
Is ventriculomegaly dangerous?
No, a slight enlargement of the ventricles of the brain is not dangerous. Pathologies that cause changes in the process of cerebrospinal fluid circulation are harmful to health and an obstacle to full development. Asymmetric ventriculomegaly is unequal enlargement of the ventricles or an excess of cerebrospinal fluid in only one of them: right or left. For example, the size of the first (left) ventricle is 9.5 mm, and the second (right) is 12 mm. Asymmetry is recognized if one ventricle is 2 mm or more larger than the diameter of the other. Asymmetric (or unilateral) ventriculomegaly accounts for about 60% of all cases. Bilateral occurs in only 40% of diagnosed children. Asymmetry is also observed with unequal enlargement of both ventricles. Right- or left-sided asymmetry of the lateral ventricles is not necessarily a bad sign. With an isolated (mild) form of ventriculomegaly, it occurs more often than with an associated (statistically more dangerous) form. Degrees of ventriculomegaly:
- light - 10-12 mm;
- moderate (average) - up to 15 mm;
- heavy - more than 15 mm.
Isolated mild or grade 1 ventriculomegaly has a favorable prognosis; the newborn will most likely not have developmental abnormalities.
Slight enlargement of the cerebral ventricles is usually random and benign, but can occur in genetic disorders and neurocognitive deficits, and is sometimes associated with structural abnormalities due to impaired neuronal migration in the fetus during embryogenesis. Mild ventriculomegaly is more common in boys (up to 75%) than in girls. Moderate ventriculomegaly also does not compromise survival, but increases the risk of neurological complications.
Severe ventriculomegaly is often associated with cerebrospinal fluid (CSF) obstruction and represents hydrocephalus, an increase in cerebrospinal fluid in the ventricular system accompanied by increased intracranial pressure.
The presence of ventriculomegaly indicates that something may be wrong in the structure of the brain, but without taking into account other pathologies detected visually or using instrumental diagnostics, this is simply a discrepancy with the standard norm. It may go away on its own. Understanding the cause of ventriculomegaly facilitates differential diagnosis. Enlargement of the ventricles can be considered as a variant of normal development (short-term failure), but sometimes it is a sign of mild, moderate and severe disorders, and the severity of pathologies of the nervous system cannot always be determined by the diameter of the cerebrospinal fluid spaces. For example, a mild degree of ventriculomegaly is one of the signs of not only mild, but also some severe pathologies of the central nervous system. The mark of 10-12 mm is most likely a normal development option, if the examination does not reveal other anomalies. It is important not only a postpartum examination, but also the diagnosis of pathologies of the central nervous system and/or other diseases during the period when ventriculomegaly is detected. You can refuse further diagnostics if there are no unexplained problems bothering the child. Only 10% of fetuses with a slight enlargement of the cerebral ventricles (up to 1.2 cm) are diagnosed with concomitant anomalies after birth. The fact that ventriculomegaly is isolated can only be detected after birth. At prenatal screening, the doctor can only make assumptions that there are no other disorders. Benign macrocrania (an enlargement of the brain portion of the skull without developmental abnormalities) is associated with mild ventriculomegaly and is characterized by rapid head growth, but does not require treatment. Disturbances in the structure of the brain that provoke the development of ventriculomegaly:
- agenesis of the corpus callosum;
- Dandy-Walker syndrome;
- defects in the development of the fetal neural tube;
- neuronal migration disorders;
- gray matter heterotopia;
- stenosis of the Sylvian aqueduct (a common cause of severe ventriculomegaly);
- a brain tumor;
- bleeding (posthemorrhagic ventriculomegaly);
- choroidpapilloma (tumor formed from the epithelium lining the ventricles of the brain);
- Choroid plexus cysts may cause transient dilatation of the ventricles, but due to their benign nature, ventriculomegaly is minor).
Some other developmental disorders of the central nervous system should not be confused with ventriculomegaly. They can be combined, but are not themselves accompanied by ventricular enlargement:
- dysembryogenetic stigmas;
- holoprosencephaly;
- hydranencephaly;
- schizencephaly;
- porencephaly;
- cerebellar hypoplasia;
- arachnoid cerebrospinal fluid cyst;
- Syringomyelia.
Congenital infections cause many cases of moderate ventriculomegaly:
- cytomegalovirus;
- toxoplasmosis;
- Zika virus;
- syphilis;
- chicken pox.
In rare cases, the ventricles become enlarged under the influence of the activity of other viruses:
- parotitis;
- enterovirus type 71;
- parainfluenza virus type 3;
- parvovirus B19;
- lymphocytic choriomeningitis.
Infection can cause isolated ventriculomegaly due to atrophy or fibrosis (overgrowth) of the soft tissue of the brain. Some cases of mild and moderate ventriculomegaly are caused by an abnormal karyotype (often Down syndrome). Approximately 15%, according to foreign studies, are associated with chromosomal mutations. Ventricular enlargement accompanies some congenital malformations associated with defects of the spinal cord, heart, or kidneys. Newborns with ventriculomegaly do not usually experience symptoms specific to this condition. If the ventricles continue to enlarge, some of the signs listed below may appear:
- head growth exceeds the age norm;
- the contours of the skull are disproportionate (hydrocephalic head shape);
- protruding fontanel;
- prominent veins are visible on the forehead and temples;
- difficult to look up;
- The child always seems to be looking down (sunset syndrome);
- developmental delays;
- increased excitability or severe drowsiness;
- poor appetite;
- nausea, vomiting.
Based on the MR signs of ventriculomegaly (size of the ventricles) and changes in other cerebrospinal fluid spaces of the brain, one can assume the type of CNS anomaly. Probable group of pathologiesWhat do the ventricles look like? Associated findings on MRI
| Gross malformations of the brain | Moderate to severe asymmetric ventriculomegaly | Narrowing of the septum transparent to 0.5-1 mm when the norm is more than 5 mm, expansion of the retrocerebellar space 2 times compared to the norm (6-7 mm) |
| Dysfunction of the midline and stem structures of the brain | Moderate enlargement of the ventricles, no or insignificant asymmetry | Narrowing of the septum pellucida and expansion of all structures containing cerebrospinal fluid: cerebral aqueduct, cistern magna, subarachnoid (subarachnoid) space |
| Isolated vascular disorders | Significant asymmetry of the cerebral ventricles with a moderate degree of enlargement | MRI signs of hemorrhages in the brain parenchyma, possible edema |
| Cysts, tumors of the posterior cranial fossa | Ventriculomegaly may be absent, but if present it is mild | Rapid expansion of the retrocerebellar space (can be tracked if an ultrasound, CT or MRI was done with a short break) |
| Arnold-Chiari malformation | 40% of patients have severe ventriculomegaly, asymmetry is uncharacteristic | Narrowing of the retrocerebellar space to 0.2 mm and the convexital parieto-occipital subarachnoid space (the area in the angular gyrus of the left hemisphere in right-handers, and vice versa in left-handers) to 0.5 mm (normal value: 3-4 mm) |
Treatment is prescribed only if there are neurological abnormalities or severe developmental delay.
Which doctors' consultations can help?
A radiologist, a genetic counselor (geneticist), a pediatric neurologist or neurologist, or a neurosurgeon with experience in diagnosing and treating ventriculomegaly can offer help. Pharmacological groupsSpecific drugs
| Diuretics (reduce brain swelling and reduce the amount of fluid in the ventricles) | For ventriculomegaly, Diacarb is often prescribed. Popular treatment regimen: 1 tablet/day. or 1/2 table. We drink twice a day on the principle of 3 days, skipping the fourth for several months. More information about the drug (indications, contraindications, what is best to combine with to reduce the risk of side effects). Analogues - Furosemide, Veroshpiron, Lasix |
| Antivirals and immunomodulators | Amiksin, Cerebrum compositum, Timalin |
| Angioprotectors (prescribed if ventriculomegaly is caused by vascular disorders) | Emoxipin, Instenon, Neuromultivit |
| Nootropics | Cereton, Pantogam, Cortexin, Encephabol, Pantocalcin (for delayed speech development), Glycine |
| Antihypoxants | Actovegin, Cytoflavin |
| Drugs that promote myelination (protection of nerve cells) | Glycine, Gliatilin, Dibazol, magnesium preparations, Neuromultivit, Multi-tabs or vitamins A, B, E and C separately |
The reason for consulting a neurosurgeon is head growth that is faster than normal (more than 1.4 cm per week).
With a constant slow increase in the volume of the ventricles, they no longer speak of ventriculomegaly, but of hydrocephalus (a consequence of the continuous accumulation of fluid with difficulty in its outflow or due to increased secretion). Neurological and neurosurgical examination, measurement of head circumference and NSG for rapidly progressing ventriculomegaly/hydrocephalus are carried out 2 times a month. On a note! For occlusive hydrocephalus, diuretics are inappropriate.
You can quickly reduce intracranial pressure (without surgery) using several procedures (performed by a doctor in a treatment room or ward):
- ventricular (access through the fontanel) or lumbar puncture;
- external ventricular drainage (subject to antibiotic therapy can be used for 1-2 weeks);
- subgaleal drainage (creating a pocket between the bone and external soft tissues, draining cerebrospinal fluid into the resulting cavity through a silicone tube, periodically withdrawing the contents using a syringe).
All these procedures are carried out under local or general anesthesia, are low-traumatic, and allow you to achieve the desired result - evacuation of cerebrospinal fluid, but temporarily. The best and most reliable way to relieve severe ventriculomegaly that has developed into hydrocephalus is shunt surgery. An additional pathway for the outflow of cerebrospinal fluid is artificially created. Operation options:
- ventriculoperitoneal shunting (diversion of cerebrospinal fluid into the abdominal cavity);
- ventriculoatrial shunt (CSF diversion into the right atrium).
If doctors recommend surgery for a child, it is worth checking whether it is possible to perform endoscopy - the creation of natural ducts in the brain without implanting shunts. The most gentle method of surgical correction of progressive ventriculomegaly with a minimum of complications. The prognosis of infants with ventriculomegaly varies significantly and depends on the presence of structural or genetic disorders, infections, and the degree of dilatation of the cerebral ventricles. With mild isolated ventriculomegaly, a favorable outcome can be expected. A meta-analysis in the journal Ultrasonography in Obstetrics and Gynecology showed that the incidence of neurological abnormalities in children with this diagnosis is no more than 8%, which is similar to the average level in the population. With moderate isolated ventriculomegaly, a favorable prognosis, according to various sources, has 75-90% of children. If, after a comprehensive examination, no other pathologies are identified, one can count on the absence of problems in the future, however, such children require periodic monitoring of the state of the central nervous system due to the risk of neurological consequences. The prognosis for ventriculomegaly combined with other anomalies depends primarily not on the degree of ventricular dilatation, but on the nature and course of the diseases that caused the accumulation of cerebrospinal fluid. The lack of progression and development of the child by age casts doubt on the real risk associated with the characteristics of brain development, since more than 90% of children in this case do not suffer from the consequences of early age pathologies. The best result (no consequences in 98% of cases) is observed under the following conditions:
- the ventricles are slightly enlarged (up to 15 mm);
- there are no echo signs of other anomalies;
- satisfactory results of genetic testing.
Whether panic over the diagnosis of ventriculomegaly is justified, you can decide if you read the reviews. Initial dataCharacteristics
| When was the diagnosis made? | In the 2nd trimester of pregnancy, confirmed in the newborn |
| Child's age | 6 years |
| Associated anomalies | None |
| Complaints | No specific complaints |
The doctor suggested terminating the pregnancy after NSG at 21 weeks. The cause was ventriculomegaly. I was worried, but decided to keep the child. They advised me to have a caesarean section, but in the end I chose a natural birth. A completely healthy baby was born, the ventricles were slightly enlarged. Over the course of 3 years, we periodically visited a neurologist for testing, but during the entire period there were no deviations in neurology. When I look at my healthy child now, I remember the doctor’s words about terminating the pregnancy and I am horrified at how much unjustified anxiety and abortions were possible due to a misunderstanding of ultrasound terms. Initial dataCharacteristics
| When was the diagnosis made? | In the 2nd trimester, an ultrasound scan, then an amniocentesis (not informative), the diagnosis was confirmed after birth |
| Child's age | 3 years |
| Associated anomalies | Missing toenails, corneal clouding, crinodactyly (crooked little fingers) |
| Complaints | Delayed speech and psychomotor development |
My daughter has severe developmental disabilities, but I still feel warm towards her and encourage all parents to do the same. The child grows up cheerful and is expected to go to a regular school. Classes with a speech pathologist and numerous physiotherapeutic procedures and massages give good results. Initial dataCharacteristics
| When was the diagnosis made? | At 3 months |
| Child's age | 7 years |
| Associated anomalies | Ventriculomegaly disappeared by 6 weeks, but cerebellar hypoplasia was discovered |
| Complaints | Developmental delay, decreased muscle tone in right leg, social and emotional problems |
Problems with muscle tone in the baby appeared when he was 6 months old, but with the help of massage and physiotherapy we solved them.
The child is very cheerful and mischievous, although there is something that upsets me. The boy reacts negatively to loud noises (gets scared, then cries for a long time), interacts poorly with other children, and does not want to participate in games. You may need to improve your communication skills.
Treatment of ventriculomegaly in the fetus
The disease is most often congenital, so it can be detected even before the birth of the child. To do this, the expectant mother undergoes an ultrasound of the abdominal cavity, based on the results of which the degree of pathology is determined. In the third degree, the woman is offered an abortion, since the risk of miscarriage is high.
In other cases, doctors begin searching for the cause of the pathology:
- A woman must be tested for infectious diseases;
- The fetus is checked for the presence of congenital pathologies (cerebral palsy, Down syndrome, etc.);
- If no abnormalities are found, the pregnant woman is prescribed potassium tablets. It saturates the fetus with oxygen, which improves its condition.
With ventriculomegaly in the fetus, the consequences depend on the promptness of treatment at the stage of pregnancy.
Etiology
The brain contains four ventricles, the main function of which is to produce cerebrospinal fluid (CSF). When disruption and stagnation of fluid occurs, ventriculomegaly develops.
A pathology is considered to be a process when the ventricles enlarge from 15 to 20 millimeters (the norm is no more than 15 millimeters). This condition may be isolated or may be accompanied by other developmental defects.
The main cause of the disease is gene and chromosomal mutations in women with pathological abnormalities during childbearing.
The causes of ventriculomegaly in the fetus are as follows:
- woman’s age – after 35 years the risk increases several times;
- intrauterine infections;
- physical damage;
- oxygen starvation;
- dropsy of the brain;
- hemorrhage or hemorrhage;
- fetal hypoxia;
- lissencephaly;
- destructive brain damage;
- hereditary predisposition.
Ventriculomegaly in the fetus can have consequences in the form of the following diseases:
- Down syndrome;
- Bonnevie-Ulrich syndrome;
- Edwards syndrome.
The pathological size of the ventricles negatively affects the heart, the musculoskeletal system, and the structural elements of the pituitary gland are disrupted.
Treatment of ventriculomegaly in a newborn
With a mild degree of pathology, no therapy is prescribed: the mother only needs to carefully monitor the child’s condition and, at the slightest deviation from the norm, contact a neurologist.
The second stage is treated with medication: the child is prescribed drugs that accelerate processes in the brain:
- Vitamin B tablets;
- Diuretics are drugs that remove excess fluid from the body;
- Medicines to improve blood circulation.
To enhance the effect, it is recommended to walk with your child in the fresh air more often and perform minimal physical exercise with him.
Surgery
The third degree of pathology is treated surgically, since taking medications will not give any results. The asymmetric shape of the ventricles is corrected by performing ventriculo-peritoneal shunting.
This is an operation during which shunts are installed to remove excess fluid. After surgery, children recover quite quickly: insomnia disappears and appetite returns.
Consequences of congenital ventriculomegaly
Perinatal mortality caused by severe intrauterine growth retardation, premature birth or intrauterine infection is 4%.
Also, in 4% of cases, newborns have various kinds of chromosomal abnormalities.
9% of newborns are born with vascular malformations of the brain.
In another 11% of cases, mental and physical developmental delay is diagnosed against the background of congenital ventriculomegaly, the severity of which can vary from mild to moderate severity.
Moreover, the risks of developing an unfavorable neurological outcome of ventriculomegaly for a female fetus are higher than similar risks for a male fetus.
Possible complications
Ventriculomegaly is a severe pathological process that leads to irreversible consequences, causing severe complications:
- Down syndrome - will be acquired due to defects in the structure of the brain;
- Edwards syndrome - mutational changes in chromosomes are observed, which leads to a whole group of pathological abnormalities in development;
- Turner syndrome - physical abnormalities occur in development;
- problems with the musculoskeletal system;
- hydrocephalus, when cerebrospinal fluid accumulates in the head.
Moreover, if the child is in the womb, such disorders can contribute to the baby's freezing or miscarriage, and pathological processes can cause premature birth.
Classification
Ventriculomegaly of the lateral ventricles is classified by type, cause, course and location.
Due to the occurrence:
- idiopathic, when the cause of the pathological process has not been identified and all indicators in the pregnant woman are normal;
- symptomatic - a woman suffered from an infectious disease during pregnancy, abused alcoholic beverages, or suffered severe stress.
Type:
- right-sided;
- isolated – has a favorable prognosis, recovery occurs in 80% of cases;
- asymmetric – with a severe course, the prognosis for recovery is low.
According to the severity of ventriculomegaly in newborns and preschool children, it is:
- mild degree, when the ventricles are small in size - up to 12 millimeters, the child becomes irritable and easily excited;
- moderate degree, when the ventricles increase to 15 millimeters - an asymmetric anomaly and a change in blood flow in the area of the disturbance are observed;
- severe - the ventricles increase to 20 millimeters, which leads to irreversible consequences in the structure of the brain;
According to the location of ventriculomegaly, it can be:
- with lateral dilatation of the ventricles (left and posterior);
- pathological changes affect the third ventricle (in the front, on the forehead);
- changes in the fourth ventricle (in the occipital part, in the cerebellum and medulla oblongata).
Moderate ventriculomegaly is a borderline condition when the size of the ventricles is 10–15 millimeters, which is a high risk, since there is a high probability of developing a pathological process. Such cases are monitored and constantly checked to eliminate the risk of further growth.