What can cause an attack?
Infections that cause fever. The infection can be caused by bacteria, but more often febrile attacks occur with viral diseases (for example, roseola and influenza).
Vaccinations that cause fever. There is a small chance of febrile seizures after vaccination against measles, rubella and mumps, and diphtheria, tetanus and whooping cough. But the risks from incomplete vaccination are higher than the risk from a febrile attack after vaccination.
Heredity. If either parent has had a febrile seizure, the child is more likely to have seizures with fever.
A febrile attack, especially one occurring for the first time in life, is very frightening for parents. In fact, most of these attacks are not dangerous and do not lead to complications or brain damage. A child with simple febrile seizures is only slightly more likely to develop epilepsy than children who have never had a febrile seizure.
Literature:
- ICD-10 (R68.83), 2021, https://www.icd10data.com/ICD10CM/Codes/R00-R99/R50-R69/R68-/R68.83
- Litvitsky P.F. Disturbances in the body's thermal balance. Fever. Issues of modern pediatrics. 2009, volume 8, no. 6, pp. 55-63. https://cyberleninka.ru/article/n/narusheniya-teplovogo-balansa-organizma-lihoradka
- Zakharova I.N. Fever in children: from symptom to diagnosis. Medical Council, 2021, No. 1, pp. 212-218. https://cyberleninka.ru/article/n/lihoradka-u-detey-ot-simptoma-k-diagnozu-1
- Korovina N.A. Fever. Variety of reasons and complexity of solutions. Medical Council, 2013, No. 2, pp. 82-90. https://cyberleninka.ru/article/n/lihoradka-mnogoobrazie-prichin-i-slozhnost-resheniya
- Verbovoy A.F., Sharonova L.A. Hypothyroidism syndrome: lecture. Journal for continuing medical education of doctors. Endocrinology: news, opinions, training, 2015, No. 4, pp. 71-75. https://cyberleninka.ru/article/n/sindrom-gipotireoza-lektsiya
- Starostina E.G. Hypoglycemia and hypoglycemic coma. Medical Council, 2013, No. 5-6, pp. 6-10. https://cyberleninka.ru/article/n/gipoglikemiya-i-gipoglikemicheskaya-koma-1
- Autonomic dysfunction syndrome in children and adolescents: clinical manifestations, diagnosis and treatment. Part 2. Methodological recommendations No. 25, Moscow 2015, Moscow Government, Moscow Health Department
- Polyakova A.S. and others. The meaning of fever in children. Issues of modern pediatrics, 2015, volume 14, no. 2, pp. 272-276. https://cyberleninka.ru/article/n/znachenie-lihoradki-u-detey
- Instructions for use of Rinzasip for children. https://grls.rosminzdrav.ru/Grls_View_v2.aspx?routingGuid=3fe093f9-82a1-468b-ad1b-1c52f75b3c7e&t=
- Pikuza O.I., Zakirova A.M. Fever in children. Educational and methodological manual for students of medical universities, Kazan, KSMU, 2013, 56 p. https://kazangmu.ru/files/prop_det_bol/Lichoradka.pdf
- Urinary tract infection in children. Clinical recommendations 2018 Union of Pediatricians of Russia
- Avkhimenko M. M. Cold injury: emergency medical care, prevention // Nurse / No. 1. – 2014. – P. 33-39.
- Differential diagnosis of infectious diseases: textbook. In 2 parts. Part 1 / comp.: D. Kh. Khunafina, O. I. Kutuev, A. N. Burganova, A. T. Galieva, L. R. Shaikhullina, T. A. Khabelova, V. I Starostina, G. R. Syrtlanova, R. S. Sultanov. – Ufa: Publishing house of the State Budgetary Educational Institution of Higher Professional Education BSMU of the Ministry of Health of Russia, 2012. – 153 p.
How to help a child during an attack?
- Place your baby on his side on a flat surface and make sure he won't fall or hit anything during the cramp (such as crib bars).
- Record the time and tell the doctor when the attack began and how long it lasted.
Attention! Do not try to open the jaw, do not put anything into the child’s mouth during an attack, this can lead to injuries (broken teeth of the child and injured fingers of the person providing assistance). Do not try to restrict the child's movements during seizures, do not restrain him.
The child may be even more afraid of the attack than the parents. Try to calm him down and support him.
If the attack occurs for the first time in life, lasts longer than 5 minutes, the child is unusually sleepy and lethargic before or after the attack, call an ambulance.
In other cases, immediately show the child to the pediatrician. The doctor should examine the child after the attack to make sure there are no signs of a central nervous system infection (meningitis or encephalitis).
How to treat fever in a child who has previously had febrile seizures?
If the child does not have an increase in temperature during illness or after vaccination, it is not recommended to give antipyretic drugs! This does not reduce the risk of an attack.
If the temperature has risen, medications to reduce it make you feel better overall, but do not help with attacks.
The harm from anticonvulsants for the prevention of febrile seizures outweighs the benefits; they are almost never prescribed.
If a child’s febrile convulsions are prolonged, at the beginning of the attack it is recommended to administer a drug from the benzodiazepine group in the form of an enema, a spray in the nose or a gel on the cheek. Unfortunately, none of these forms are registered in Russia. Therefore, if an attack lasts longer than 5 minutes, an emergency doctor may give an injection of such a medicine.
For antipyretic drugs, children can be given ibuprofen at a dose of 10 mg/kg every 8 hours or paracetamol at a dose of 15 mg/kg every 6 hours. Don't give children aspirin!
It is important to know
Parents often mistake normal chills associated with fever for febrile seizures. With such chills, the child's arms and legs may shake rhythmically. This is similar to a seizure, but the child is conscious and reacts if spoken to. So that the doctor can better determine whether what happened was a seizure, and if so, what kind, try to clearly record the duration of the seizure, describe it as specifically as possible, and ideally, record what is happening on video (one person helps the child, the other films it on the phone).
Tics in children
Tics, or hyperkinesis, are repeated, unexpected short stereotypical movements or statements that are superficially similar to voluntary actions. A characteristic feature of tics is their involuntary nature, but in most cases the patient can reproduce or partially control his own hyperkinesis. With a normal level of intellectual development in children, the disease is often accompanied by cognitive impairment, motor stereotypies and anxiety disorders.
The prevalence of tics reaches approximately 20% in the population.
There is still no consensus on the occurrence of tics. The decisive role in the etiology of the disease is given to the subcortical nuclei - the caudate nucleus, globus pallidus, subthalamic nucleus, and substantia nigra. Subcortical structures interact closely with the reticular formation, thalamus, limbic system, cerebellar hemispheres and the frontal cortex of the dominant hemisphere. The activity of subcortical structures and frontal lobes is regulated by the neurotransmitter dopamine. Insufficiency of the dopaminergic system leads to disturbances of attention, lack of self-regulation and behavioral inhibition, decreased control of motor activity and the appearance of excessive, uncontrolled movements.
The effectiveness of the dopaminergic system can be affected by intrauterine developmental disorders due to hypoxia, infection, birth trauma, or hereditary deficiency of dopamine metabolism. There are indications of an autosomal dominant type of inheritance; However, it is known that boys suffer from tics approximately 3 times more often than girls. Perhaps we are talking about cases of incomplete and sex-dependent penetration of the gene.
In most cases, the first appearance of tics in children is preceded by external unfavorable factors. Up to 64% of tics in children are provoked by stressful situations - school maladjustment, extracurricular activities, uncontrolled watching of TV shows or prolonged work on the computer, conflicts in the family and separation from one of the parents, hospitalization.
Simple motor tics can be observed in the long-term period of a traumatic brain injury. Vocal tics - coughing, sniffing, expectorating throat sounds - are often found in children who often suffer from respiratory infections (bronchitis, tonsillitis, rhinitis).
In most patients, there is a diurnal and seasonal dependence of tics - they intensify in the evening and become aggravated in the autumn-winter period.
A separate type of hyperkinesis includes tics that arise as a result of involuntary imitation in some highly suggestible and impressionable children. This happens in the process of direct communication and under the condition of a certain authority of the child with tics among his peers. Such tics go away on their own some time after the cessation of communication, but in some cases such imitation is the debut of the disease.
Clinical classification of tics in children
By etiology
Primary, or hereditary, including Tourette's syndrome. The main type of inheritance is autosomal dominant with varying degrees of penetration; sporadic cases of the disease are possible.
Secondary or organic. Risk factors: anemia in pregnant women, maternal age over 30 years, fetal malnutrition, prematurity, birth trauma, previous brain injuries.
Cryptogenic. They occur against the background of complete health in a third of patients with tics.
According to clinical manifestations
Local (facial) tic. Hyperkinesis affects one muscle group, mainly facial muscles; frequent blinking, squinting, twitching of the corners of the mouth and wings of the nose predominate (Table 1). Blinking is the most persistent of all local tic disorders. Closed eyes are characterized by a more pronounced disturbance of tone (dystonic component). Movements of the wings of the nose, as a rule, are associated with rapid blinking and are among the unstable symptoms of facial tics. Single facial tics practically do not interfere with patients and in most cases are not noticed by the patients themselves.
| Table 1 Types of motor tics (V.V. Zykov) |
Common tic. Several muscle groups are involved in hyperkinesis: facial muscles, muscles of the head and neck, shoulder girdle, upper limbs, abdominal and back muscles. In most patients, a common tic begins with blinking, which is accompanied by opening the gaze, turning and tilting the head, and lifting the shoulders. During periods of exacerbation of tics, schoolchildren may have problems completing written assignments.
Vocal tics. There are simple and complex vocal tics.
The clinical picture of simple vocal tics is represented mainly by low sounds: coughing, “clearing the throat,” grunting, noisy breathing, sniffing. Less common are high-pitched sounds such as “i”, “a”, “oo-u”, “uf”, “af”, “ay”, squealing and whistling. With an exacerbation of tic hyperkinesis, vocal phenomena may change, for example, coughing turns into grunting or noisy breathing.
Complex vocal tics are observed in 6% of patients with Tourette syndrome and are characterized by the pronunciation of individual words, swearing (coprolalia), repetition of words (echolalia), and rapid, uneven, unintelligible speech (palilalia). Echolalia is an intermittent symptom and may occur over several weeks or months. Coprolalia usually represents a status condition in the form of serial utterance of swear words. Often, coprolalia significantly limits the child’s social activity, depriving him of the opportunity to attend school or public places. Palilalia is manifested by obsessive repetition of the last word in a sentence.
Generalized tic (Tourette's syndrome). Manifests itself as a combination of common motor and vocal simple and complex tics.
Table 1 presents the main types of motor tics depending on their prevalence and clinical manifestations.
As can be seen from the table presented, as the clinical picture of hyperkinesis becomes more complex, from local to generalized, tics spread from top to bottom. Thus, with a local tic, violent movements are noted in the facial muscles; with a widespread tic, they move to the neck and arms; with a generalized tic, the torso and legs are involved in the process. Blinking occurs with equal frequency in all types of tics.
According to the severity of the clinical picture
The severity of the clinical picture is assessed by the number of hyperkinesis in the child during 20 minutes of observation. In this case, tics can be absent, single, serial or status. Severity assessment is used to standardize the clinical picture and determine the effectiveness of treatment.
With single tics, their number during 20 minutes of examination ranges from 2 to 9; they are more common in patients with local forms and in remission in patients with widespread tics and Tourette's syndrome.
With serial tics, during a 20-minute examination, from 10 to 29 hyperkinesis are observed, after which many hours of breaks occur. A similar picture is typical during exacerbation of the disease and occurs in any localization of hyperkinesis.
With tic status, serial tics follow with a frequency of 30 to 120 or more per 20 minutes of examination without a break during the day.
Similar to motor tics, vocal tics can also be single, serial and status, intensifying in the evening, after emotional stress and overwork.
According to the course of the disease
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), there are transient tics, chronic tics and Tourette's syndrome.
A transient , or transient , course of tics implies the presence of motor or vocal tics in a child with complete disappearance of symptoms of the disease within 1 year. Characteristic of local and widespread tics.
Chronic tic disorder is characterized by motor tics lasting more than 1 year without a vocal component. Chronic vocal tics in isolated form are rare. There are remitting, stationary and progressive subtypes of the course of chronic tics.
In a remitting course, periods of exacerbation are replaced by complete regression of symptoms or the presence of local single tics that occur against the background of intense emotional or intellectual stress. The relapsing-remitting subtype is the main variant of the course of tics. With local and widespread tics, exacerbation lasts from several weeks to 3 months, remissions last from 2–6 months to a year, in rare cases up to 5–6 years. With drug treatment, complete or incomplete remission of hyperkinesis is possible.
The stationary type of the disease is determined by the presence of persistent hyperkinesis in various muscle groups, which persist for 2–3 years.
The progressive course is characterized by the absence of remissions, the transition of local tics to widespread or generalized ones, the complication of stereotypes and rituals, the development of tic status, and resistance to therapy. A progressive course predominates in boys with hereditary tics. Unfavorable signs are the presence of aggressiveness, coprolalia, and obsessions in the child.
There is a relationship between the localization of tics and the course of the disease. Thus, a local tic is characterized by a transient-remitting type of course, a widespread tic is characterized by a remitting-stationary type, and Tourette's syndrome is characterized by a remitting-progressive type.
Age dynamics of tics
Most often, tics appear in children aged 2 to 17 years, the average age is 6–7 years, the frequency of occurrence in the pediatric population is 6–10%. Most children (96%) develop tics before age 11. The most common manifestation of a tic is blinking the eyes. At the age of 8–10 years, vocal tics appear, which account for approximately a third of the cases of all tics in children and occur both independently and against the background of motor ones. Most often, the initial manifestations of vocal tics are sniffing and coughing. The disease is characterized by an increasing course with a peak of manifestations at 10–12 years, then a decrease in symptoms is noted. By age 18, approximately 50% of patients become free of tics spontaneously. At the same time, there is no relationship between the severity of the manifestation of tics in childhood and in adulthood, but in most cases in adults the manifestations of hyperkinesis are less pronounced. Sometimes tics first appear in adults, but they are characterized by a milder course and usually last no more than 1 year.
The prognosis for local tics is favorable in 90% of cases. In the case of common tics, 50% of children experience complete regression of symptoms.
Tourette's syndrome
The most severe form of hyperkinesis in children is, without a doubt, Tourette's syndrome. Its frequency is 1 case per 1,000 children in boys and 1 in 10,000 in girls. The syndrome was first described by Gilles de la Tourette in 1882 as a “disease of multiple tics.” The clinical picture includes motor and vocal tics, attention deficit disorder, and obsessive-compulsive disorder. The syndrome is inherited with high penetrability in an autosomal dominant manner, and in boys, tics are more often combined with attention deficit hyperactivity disorder, and in girls - with obsessive-compulsive disorder.
The currently generally accepted criteria for Tourette's syndrome are those given in the DSM III revision classification. Let's list them.
- A combination of motor and vocal tics that occur simultaneously or at different intervals.
- Repeated tics throughout the day (usually in series).
- The location, number, frequency, complexity and severity of tics changes over time.
- The onset of the disease is before 18 years of age, duration is more than 1 year.
- Symptoms of the disease are not associated with the use of psychotropic drugs or central nervous system disease (Huntington's chorea, viral encephalitis, systemic diseases).
The clinical picture of Tourette's syndrome depends on the age of the patient. Knowledge of the basic patterns of disease development helps to choose the right treatment tactics.
The onset of the disease develops at 3–7 years. The first symptoms are local facial tics and shoulder twitching. Then hyperkinesis spreads to the upper and lower extremities, shuddering and turning of the head, flexion and extension of the hand and fingers, throwing the head back, contraction of the abdominal muscles, jumping and squats appear, one type of tics is replaced by another. Vocal tics often join motor symptoms for several years after the onset of the disease and intensify during the acute stage. In a number of patients, vocalisms are the first manifestations of Tourette's syndrome, which are subsequently joined by motor hyperkinesis.
Generalization of tic hyperkinesis occurs over a period lasting from several months to 4 years. At the age of 8–11 years, children experience a peak in clinical manifestations of symptoms in the form of a series of hyperkinesis or repeated hyperkinetic states in combination with ritual actions and auto-aggression. The tic status in Tourette's syndrome characterizes a severe hyperkinetic state. A series of hyperkinesis is characterized by the replacement of motor tics with vocal ones, followed by the appearance of ritual movements. Patients note discomfort from excessive movements, for example, pain in the cervical spine that occurs when turning the head. The most severe hyperkinesis is a throwing back of the head - in this case, the patient can repeatedly hit the back of the head against the wall, often in combination with simultaneous clonic twitching of the arms and legs and the appearance of muscle pain in the extremities. The duration of status tics ranges from several days to several weeks. In some cases, exclusively motor or predominantly vocal tics are noted (coprolalia). During status tics, consciousness in children is completely preserved, but hyperkinesis is not controlled by patients. During exacerbations of the disease, children cannot attend school and self-care becomes difficult for them. It is characterized by a remitting course with exacerbations lasting from 2 to 12–14 months and incomplete remissions from several weeks to 2–3 months. The duration of exacerbations and remissions is directly dependent on the severity of tics.
In most patients, at the age of 12–15 years, generalized hyperkinesis goes into a residual phase , manifested by local or widespread tics. In a third of patients with Tourette's syndrome without obsessive-compulsive disorders in the residual stage, a complete cessation of tics is observed, which can be considered as an age-dependent infantile form of the disease.
Comorbidity of tics in children
Tics often occur in children with pre-existing central nervous system (CNS) conditions, such as attention deficit hyperactivity disorder (ADHD), cerebrasthenic syndrome, and anxiety disorders including generalized anxiety disorder, specific phobias, and obsessive-compulsive disorder.
About 11% of children with ADHD have tics. Mostly these are simple motor and vocal tics with a chronic recurrent course and a favorable prognosis. In some cases, the differential diagnosis between ADHD and Tourette's syndrome is difficult when hyperactivity and impulsivity appear in a child before the development of hyperkinesis.
In children suffering from generalized anxiety disorder or specific phobias, tics can be provoked or intensified by worries and worries, unusual surroundings, prolonged anticipation of an event and a concomitant increase in psycho-emotional stress.
In children with obsessive-compulsive disorder, vocal and motor tics are combined with compulsive repetition of a movement or activity. Apparently, in children with anxiety disorders, tics are an additional, albeit pathological, form of psychomotor discharge, a way of calming and “processing” accumulated internal discomfort.
Cerebrasthenic syndrome in childhood is a consequence of traumatic brain injuries or neuroinfections. The appearance or intensification of tics in children with cerebrasthenic syndrome is often provoked by external factors: heat, stuffiness, changes in barometric pressure. Typically, tics increase with fatigue, after long-term or repeated somatic and infectious diseases, and increased educational loads.
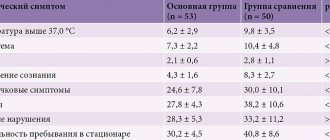
Let us present our own data. Of the 52 children who complained of tics, there were 44 boys and 7 girls; the ratio “boys: girls” was “6:1” (Table 2).
| Table 2 Distribution of children with tics by age and gender |
So, the largest number of calls for tics was observed in boys aged 5–10 years, with a peak at 7–8 years. The clinical picture of tics is presented in Table. 3.
| Table 3 Types of tics in group patients |
Thus, simple motor tics with localization mainly in the muscles of the face and neck and simple vocal tics imitating physiological actions (coughing, expectoration) were most often observed. Jumping and complex vocal expressions were much less common - only in children with Tourette syndrome.
Temporary (transient) tics lasting less than 1 year were observed more often than chronic (remitting or stationary) tics. Tourette's syndrome (chronic stationary generalized tic) was observed in 7 children (5 boys and 2 girls) (Table 4).
| Table 4 Distribution of patients by type of treatment for tics |
Treatment
The main principle of treatment for tics in children is an integrated and differentiated approach to treatment. Before prescribing medication or other therapy, it is necessary to find out the possible causes of the disease and discuss methods of pedagogical correction with parents. It is necessary to explain the involuntary nature of hyperkinesis, the impossibility of controlling them by willpower and, as a consequence of this, the inadmissibility of comments to a child about tics. Often the severity of tics decreases when the demands on the child from the parents are reduced, attention is not focused on his shortcomings, and his personality is perceived as a whole, without isolating “good” and “bad” qualities. Streamlining the regimen and playing sports, especially in the fresh air, have a therapeutic effect. If induced tics are suspected, the help of a psychotherapist is necessary, since such hyperkinesis can be relieved by suggestion.
When deciding whether to prescribe drug treatment, it is necessary to take into account factors such as etiology, age of the patient, severity and severity of tics, their nature, and concomitant diseases. Drug treatment must be carried out for severe, pronounced, persistent tics, combined with behavioral disorders, poor performance at school, affecting the child’s well-being, complicating his adaptation in the team, limiting his opportunities for self-realization. Drug therapy should not be prescribed if the tics only bother the parents but do not interfere with the child's normal activities.
The main group of drugs prescribed for tics are antipsychotics: haloperidol, pimozide, fluphenazine, tiapride, risperidone. Their effectiveness in the treatment of hyperkinesis reaches 80%. The drugs have analgesic, anticonvulsant, antihistamine, antiemetic, neuroleptic, antipsychotic, and sedative effects. The mechanisms of their action include blockade of postsynaptic dopaminergic receptors of the limbic system, hypothalamus, trigger zone of the gag reflex, extrapyramidal system, inhibition of the reuptake of dopamine by the presynaptic membrane and subsequent deposition, as well as blockade of adrenergic receptors of the reticular formation of the brain. Side effects: headache, drowsiness, difficulty concentrating, dry mouth, increased appetite, agitation, restlessness, anxiety, fear. With prolonged use, extrapyramidal disorders may develop, including increased muscle tone, tremor, and akinesia.
Haloperidol: the initial dose is 0.5 mg at night, then it is increased by 0.5 mg per week until a therapeutic effect is achieved (1-3 mg/day in 2 divided doses).
Pimozide (Orap) is comparable in effectiveness to haloperidol, but has fewer side effects. The initial dose is 2 mg/day in 2 divided doses; if necessary, the dose is increased by 2 mg per week, but not higher than 10 mg/day.
Fluphenazine is prescribed at a dose of 1 mg/day, then the dose is increased by 1 mg per week to 2–6 mg/day.
Risperidone belongs to the group of atypical antipsychotics. Risperidone is known to be effective for tics and related behavioral disorders, especially those of an oppositional defiant nature. The initial dose is 0.5–1 mg/day with a gradual increase until positive dynamics are achieved.
Tiaprid (Tiapridal): children 7–12 years old are recommended 50 mg (1/2 tablet) 1–2 times a day.
When choosing a drug to treat a child with tics, you should consider the dosage form that is most convenient for dosing. Optimal for titration and subsequent treatment in childhood are drop forms (haloperidol, risperidone), which allow you to most accurately select a maintenance dose and avoid an unjustified overdose of the drug, which is especially important when carrying out long courses of treatment. Preference is also given to drugs with a relatively low risk of side effects (risperidone, tiapride).
Metoclopramide (Reglan, Cerucal) is a specific blocker of dopamine and serotonin receptors in the trigger zone of the brain stem. For Tourette's syndrome in children, it is used in a dose of 5–10 mg per day (1/2–1 tablet), in 2–3 doses. Side effects include extrapyramidal disorders that occur when the dose exceeds 0.5 mg/kg/day.
In recent years, valproic acid preparations have been used to treat hyperkinesis. The main mechanism of action of valproate is to enhance the synthesis and release of γ-aminobutyric acid, which is an inhibitory neurotransmitter of the central nervous system. Valproates are the first choice drugs in the treatment of epilepsy, but their thymoleptic effect, manifested in a decrease in hyperactivity, aggressiveness, irritability, as well as a positive effect on the severity of hyperkinesis, is of interest. The therapeutic dose recommended for the treatment of hyperkinesis is significantly lower than for the treatment of epilepsy and is 20 mg/kg/day. Side effects include drowsiness, weight gain, and hair loss.
When hyperkinesis is combined with obsessive-compulsive disorder, antidepressants - clomipramine, fluoxetine - have a positive effect.
Clomipramine (Anafranil, Clominal, Clofranil) is a tricyclic antidepressant whose mechanism of action is inhibition of the reuptake of norepinephrine and serotonin. The recommended dose for children with tics is 3 mg/kg/day. Side effects include transient visual disturbances, dry mouth, nausea, urinary retention, headache, dizziness, insomnia, excitability, extrapyramidal disorders.
Fluoxetine (Prozac) is an antidepressant, a selective serotonin reuptake inhibitor with low activity in relation to the norepinephrine and dopaminergic systems of the brain. In children with Tourette's syndrome, it effectively eliminates restlessness, anxiety, and fear. The initial dose in childhood is 5 mg/day once a day, the effective dose is 10–20 mg/day once in the morning. The drug is generally well tolerated, side effects are relatively rare. Among them, the most significant are anxiety, sleep disturbances, asthenic syndrome, sweating, and weight loss. The drug is also effective in combination with pimozide.
Literature
- Zavadenko N. N. Hyperactivity and attention deficit in childhood. M.: ACADEMA, 2005.
- Mash E., Wolf D. Child mental disorders. SPb.: Prime EUROZNAK; M.: OLMA PRESS, 2003.
- Omelyanenko A., Evtushenko O. S., Kutyakova et al. // International Neurological Journal. Donetsk. 2006. No. 3(7). pp. 81-82.
- Petrukhin A. S. Neurology of childhood. M.: Medicine, 2004.
- Fenichel J.M. Pediatric neurology. Fundamentals of clinical diagnosis. M.: Medicine, 2004.
- L. Bradley, Schlaggar, Jonathan W. Mink. Movement // Disorders in Children Pediatrics in Review. 2003; 24(2).
N. Yu. Suvorinova , Candidate of Medical Sciences, Russian State Medical University, Moscow