Content:
- Alprazolam: general description of the drug: 1.1. Mechanism of action. 1.2. Indications for use. 1.3. Contraindications and features of use. 1.4. Why Alprazolam is dangerous: side effects and symptoms of overdose.
- How does addiction to Alprazolam develop?
- How to relieve addiction to Alprazolam: principles of treatment.
Alprazolam is a drug from the group of benzodiazepines, hypnotics and sedatives that inhibit the activity of the central nervous system. Benzodiazepine tranquilizers became firmly established in medical practice several decades ago, but they are still very often prescribed in psychiatry and neurology. But at the same time
Alprazolam is more likely than other medications of this pharmacological group to cause drug dependence. And often a person continues to take pills even after completing the course of treatment, obtaining them fraudulently in pharmacies or on the illegal drug market. It is not easy to cope with the uncontrolled use of the drug without the help of a narcologist, because a sudden cessation of its use is accompanied by a real withdrawal syndrome. This condition requires mandatory detoxification, psychotherapy and subsequent rehabilitation.
Physiological effects
Alprazolam has anxiolytic, central muscle relaxant, anticonvulsant, sedative-hypnotic and antipanic effects. The anti-anxiety effect is manifested by the elimination of emotional tension, anxiety, anxiety and fear. A less pronounced sedative-hypnotic effect weakens symptoms of neurotic origin. The period of falling asleep is shortened, the duration of sleep increases, and the number of night awakenings is reduced. This is achieved by reducing the susceptibility of emotional, motor and vegetative (from internal organs) stimuli.
general description
Alprazolam has all the properties of “classical” tranquilizers. The spectrum of its pharmacotherapeutic activity includes the following effects:
- anxiolytic;
- sedative;
- hypnotic;
- muscle relaxant;
- anticonvulsant.
Due to the high affinity for specific endogenous benzodiazepine receptors, the effect of the drug develops faster. It differs from its analogues in less severe adverse reactions: it causes daytime drowsiness, sudden mood swings, and lethargy much less frequently. That is why it is very often used in outpatient practice.
Mechanism of action
The therapeutic effect of Alprazolam is associated with its selective effect on various classes of GABA receptors (GABA or γ-aminobutyric acid is the main “inhibitory” neurotransmitter). They are localized in the cerebellum, hippocampus, spinal cord and other parts of the central nervous system. By interacting with GABA receptors, Alprazolam indirectly affects the functions of the noradrenergic, serotonergic, cholinergic and opioidergic systems. This is what explains the effectiveness of the medication for anxiety and depressive symptoms.
The drug also has lipophilic properties, so it binds well to plasma proteins and easily penetrates the blood-brain barrier. Thanks to this, the therapeutic effect appears very quickly. Up to 75–80% of the drug is excreted unchanged from the body in the urine, the rest is metabolized in the liver.
Indications for use
As practice and clinical research data show, Alprazolam is most effective for pathologies accompanied by anxiety, fear and restlessness. This:
- panic, obsessive-compulsive, acute stress, generalized anxiety disorder;
- some forms of depression;
- phobias;
- alcohol or drug withdrawal (with caution due to the risk of complications);
- severe premenstrual syndrome;
- somatic diseases accompanied by anxiety syndrome.
Contraindications and application features
Based on the characteristics of metabolism, Alprazolam is prescribed with caution in chronic pathologies of the liver and kidneys. In such cases, individual dose selection is required. A gradual accumulation of the drug and a high risk of intoxication cannot be ruled out. Therefore, for such diseases, the medication is prescribed only according to strict indications and the impossibility of choosing a safer analogue.
During the course of treatment with Alprazolam, medications that reduce the activity of liver enzymes are contraindicated. These are the following:
- antiviral;
- antifungal;
- some antibacterials (in particular, erythromycin and ciprofloxacin);
- antidepressants;
- antiulcer (omeprazole), etc.
Due to the risk of overdose, narcotic analgesics, other sedative and hypnotic medications, and alcohol are strictly prohibited. Alprazolam is contraindicated in:
- respiratory failure, obstructive chronic pulmonary diseases;
- individual intolerance and allergic reaction;
- pregnancy due to the risk of severe congenital malformations of the fetus, you should also stop breastfeeding;
- in childhood and adolescence (up to 18 years);
- severe depression with suicide attempts (benzodiazepines increase the symptoms of the disorder).
Why Alprazolam is dangerous: side effects and overdose symptoms
The most common adverse reactions are of a neurological nature. This feeling of fatigue, dizziness, drowsiness, exercise intolerance, general malaise. They are most pronounced at the initial stage of the course of treatment, and then gradually disappear in most patients. Also possible:
- lack of appetite;
- stool disorders, heartburn, flatulence;
- weight gain;
- in women - irregular menstrual cycle.
Overdose is accompanied by severe symptoms:
- slurred speech;
- impaired coordination of movements;
- slowing down the reaction rate;
- respiratory depression.
However, exceeding the daily dose is especially dangerous if you are dependent on Alprazolam, when the person no longer follows the doctor’s recommendations. When combined with alcohol or drugs, an overdose can be fatal.
Experience of using alprazolam in complex therapy of mental disorders
Tranquilizers (benzodiazepines) constitute one of the main classes of psychotropic drugs and have been used in clinical medicine for more than 50 years.
Currently, about 30 different drugs of benzodiazepine structure (anxiolytics and hypnotics) are used. Despite the fact that in 1983 the WHO recognized the ability of benzodiazepines to cause drug dependence, they are still widely used not only in psychiatry, but also in other areas of medicine, and in a number of cases they are irreplaceable. The development of antidepressants with a pronounced anxiolytic effect (especially selective serotonin reuptake inhibitors), anxiolytics and hypnotics of non-benzodiazepine structure contributed to some displacement of benzodiazepines from medical practice, however, due to a specific mechanism of action that ensures high and rapidly developing psychotropic activity and good tolerability, they invariably occupy their niche in the treatment of mental disorders of the neurotic level.
In the spectrum of action of benzodiazepines, several main effects are traditionally distinguished: anxiolytic (anti-anxiety), sedative, hypnotic, muscle relaxant, anticonvulsant and amnestic. Currently, their anxiolytic and hypnotic effects are most important for clinical practice, while the rest are almost not used or are considered as side effects [10].
Alprazolam, a typical representative of benzodiazepine anxiolytics, has all the properties of drugs in this group to varying degrees.
The main thing for it is an anxiolytic effect. Alprazolam is a high-potency benzodiazepine, that is, a pronounced anxiolytic effect develops when using low doses of the drug. This is explained by the fact that alprazolam has a higher affinity for specific benzodiazepine receptors [1].
There are other properties that distinguish alprazolam from other representatives of this group: average duration of action, less pronounced sedation and behavioral toxicity. These features allow alprazolam to be widely used, including in outpatient practice. In addition, the ability of alprazolam to reduce the symptoms of depression is used in the treatment of mental disorders. Alprazolam is believed to be the only benzodiazepine tranquilizer that exhibits antidepressant activity [44].
The spectrum of clinical effects of alprazolam, like other benzodiazepines, is based on the modulation of GABAA receptors, followed by secondary neurochemical and hormonal changes. It is discussed that stimulation of GABA receptors leads to changes in the activity of the monoaminergic system [10]. At the same time, a weakening of the activity of the hypothalamic-pituitary-adrenal system is described [57]. Long-term use of benzodiazepines, including alprazolam, leads to a decrease in the sensitivity of GABA receptors [34]. This is the basis for the development of the phenomenon of addiction. However, it is believed that tolerance does not develop to all effects of benzodiazepines. It is unconditional regarding its hypnotic, muscle relaxant and anticonvulsant effects and is controversial regarding its anxiolytic effect [10]. Indeed, many patients take alprazolam long-term to relieve anxiety without reducing the effectiveness of treatment.
It is assumed that due to the selective effect on the α2 and α3 subunits of GABA receptors, the antidepressant effect of alprazolam is realized, which is absent in the spectrum of psychotropic activity of other tranquilizers, the action of which is associated with stimulation of GABA receptors [44].
There are interesting data on the bipolarity of the neurochemical action of alprazolam depending on the initial emotional state: in depression, the drug enhances noradrenergic activity (especially in the prefrontal cortex and hippocampus), and in anxiety it weakens it [46].
Benzodiazepines do not have an affinity for dopamine, serotonin, cholinergic, adrenergic, histamine and other receptors of the central nervous system and the autonomic nervous system. This determines the absence of side effects during their use, which are so characteristic of other classes of psychotropic drugs.
The average time to reach the maximum concentration of alprazolam in the blood is 1.5 hours [35, 36]. Due to its high lipophilicity, the drug, like other benzodiazepines, penetrates well through the blood-brain barrier, which explains the rapid onset of its therapeutic effect. Alprazolam is an intermediate-acting benzodiazepine: the average half-life of the drug is 11 hours [19].
According to various literature sources, alprazolam has a unique spectrum of psychotropic activity compared to other tranquilizers [2, 11]. The drug is most effective in the treatment of disorders, the clinical picture of which is mainly determined by anxiety symptoms of varying degrees of severity. Such conditions include, first of all, panic disorder, generalized anxiety disorder, various anxiety-depressive states, including reactive and somatogenic. In addition, alprazolam has proven itself in the treatment of obsessive-compulsive disorder, isolated phobias, and withdrawal states.
The effectiveness of alprazolam in the treatment of panic disorder is evidenced by the results of numerous comparative studies [45]. A number of studies [11] indicate that in the treatment of panic disorder, compared with other benzodiazepine tranquilizers, alprazolam significantly reduces the frequency of panic attacks and reduces the severity of anxiety and depressive symptoms. If cases of partial improvement are taken into account, alprazolam is effective in 80% of cases [9, 15]. It is believed that in this regard the effect of alprazolam is comparable only to clonazepam [7,11]. It has been established that alprazolam at an average dose of 4 to 7 mg/day. more effective than placebo during 4 weeks of observation [12]. However, there was no direct relationship between the concentration of the drug in the blood and the effectiveness of therapy. This means that the effectiveness of treatment largely depends not on the dose of the drug, but on clinical and psychopathological factors. In addition, it is indicated that the drug acts not only on anticipatory anxiety, but also on the symptoms of panic attacks themselves, reducing their severity and preventing the development of repeated panic attacks [6]. The dose range of alprazolam for the treatment of panic disorder is wider than for the treatment of other anxiety conditions, and is up to 10 mg/day. (on average 2-6 mg/day) [1.47], divided into 3-4 doses.
Numerous studies have examined the use of alprazolam for generalized anxiety disorder (GAD). The symptoms of GAD are effectively reduced by treatment with alprazolam at an average daily dosage of 0.5-4.0 mg, divided into 3-4 doses, in different age groups of patients, which is confirmed by the results of numerous placebo-controlled studies [14, 24, 25, 26, 29 ]. It has been established that, compared with other benzodiazepine tranquilizers, the use of alprazolam is accompanied by fewer side effects [6, 14, 27, 32]. It should also be noted that the effect is relatively rapid, manifesting itself already during the first week of treatment [33]. Despite the high effectiveness of alprazolam in the treatment of GAD, antidepressants are currently preferred in the treatment of this pathology [3, 48, 49]. However, even in this case, the role of benzodiazepines in the treatment of GAD cannot be underestimated. Considering the fact that the effect of antidepressants appears only several weeks after the start of therapy, the use of benzodiazepines at the beginning of treatment to relieve anxiety and insomnia does not yet have an alternative. Due to the risk of developing drug dependence, it is recommended to use alprazolam for several weeks followed by gradual withdrawal. In cases where this period is not enough to develop a lasting therapeutic effect, longer use of the drug is possible, subject to careful follow-up.
In a study of the effectiveness of alprazolam in patients with GAD manifested by irritable bowel syndrome, after 4 weeks of therapy there was a significant reduction in both anxiety symptoms (in 98% of patients) and gastrointestinal complaints (in 89% of patients) [58]. The drug has also proven itself in the treatment of anxiety in alcohol withdrawal states [40].
It is repeatedly mentioned in the literature that, in addition to the anxiolytic effect itself, the drug also has an antidepressant effect, which has not been detected in other tranquilizers [6, 17, 41,60]. Its presence was discovered shortly after the active introduction of alprazolam into clinical practice and was confirmed in a number of further studies. There are indications of the effectiveness of alprazolam not only in neurotic, but also in endogenous depression [6]. Moreover, its effect is comparable to tricyclic antidepressants [17, 39, 53, 55]. Many authors indicate the preference of its use for syndromes in the structure of which there is a combination of anxiety and depressive symptoms [4, 5,10].
There is evidence indicating the effectiveness of alprazolam in the treatment of premenstrual syndrome [30, 37].
The successful use of alprazolam in the treatment of acute stress and obsessive-compulsive disorders has been described. In this case, the drug was prescribed either at the beginning of the course in addition to selective serotonin reuptake inhibitors (SSRIs) to relieve severe anxiety, or as monotherapy in cases of resistance or intolerance to SSRIs [16, 42]. However, despite speculation, alprazolam was ineffective in the treatment of post-traumatic stress disorder (PTSD) [23].
Data have been obtained on the use of alprazolam as a corrector of extrapyramidal symptoms (especially acute dystonia and akathisia) caused by taking antipsychotics [38]. However, in the presence of other highly effective means of correcting neuroleptic syndrome, alprazolam cannot be considered as a first-line drug.
The most common side effects during therapy with alprazolam are sedation and drowsiness [31], which is explained by the interaction of the drug with GAMKA receptors and during the course of treatment the above side effects decrease significantly.
Regular use of alprazolam should be discontinued gradually to avoid the development of withdrawal syndrome. During this period, lasting from several weeks to months, the daily dosage of the drug is gradually reduced until complete discontinuation [54]. A number of studies [43, 48, 54] note that reducing the dose of benzodiazepine tranquilizers may be accompanied by withdrawal syndrome and the return of clinical manifestations of the underlying disease, especially in cases of abrupt cessation of therapy.
Despite the widespread perception of the risk of drug dependence, data from numerous studies indicate that the incidence of dependence among patients receiving alprazolam is relatively low [50, 51, 52]. The authors note that dependence on benzodiazepines is a relatively rare phenomenon and occurs mainly in individuals who abuse alcohol or drugs.
There are some other side effects of alprazolam worth mentioning. A number of studies have revealed a deterioration in the processes of perception and reproduction of new information [28, 56]. This feature must be taken into account when driving a car [18]. It is also important to note the interaction of alprazolam with alcohol, because Many patients with anxiety symptoms independently resort to drinking alcohol to alleviate their condition. Their combined use leads to a significant deterioration in results when performing psychological tests [20], and in some patients it increases aggression and irritability [21,22].
Thus, as numerous data show, including recent years, alprazolam remains a fairly popular and effective tranquilizer. However, many issues require clarification and additional study. In particular, the place of alprazolam in the complex treatment of mental disorders along with new drugs from other psychopharmacological groups needs to be considered. Questions remain not entirely clear regarding the dosages of alprazolam used, the possible duration of its use, as well as the frequency and conditions for the formation of dependence.
Purpose of the study: to analyze the use of alprazolam in the complex treatment of various mental disorders to clarify the indications for its use.
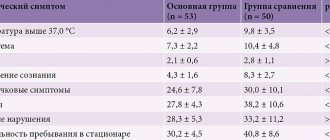
The medical histories of 124 patients who were undergoing inpatient (58 people - 46.8%) and outpatient (66 people - 53.2%) treatment in the psychiatric clinic named after. S.S. Korsakov First Moscow State Medical University named after. THEM. Sechenov and taking alprazolam at a certain stage of therapy. All patients underwent a thorough psychiatric and somato-neurological examination using the necessary paraclinical methods to assess the effectiveness of therapy and possible side effects.
Among the patients there were 74 women (59.7%) and 50 (40.3%) men aged from 26 to 70 years. The duration of the diseases ranged from 2 months to 40 years.
According to the results of the assessment of mental disorders according to ICD-10, patients were distributed as follows: schizophrenia F20 was diagnosed in 24 patients (19.4%), of which paranoid F20.0 - in 10 (8.1%), sluggish F21 - in 14 (11.3 %); affective disorders F3 - in 46 (37.2%), including a depressive episode of varying severity F32 - in 8 (6.5%), recurrent depressive disorder F33 - in 26 (21.0%), bipolar disorder F31 - in 12 (9.7%); organic brain lesions F06 - in 6 (4.8%), of which organic anxiety disorder F06.4 - in 4 (6.4%), organic personality disorder F07.0 - in 2 (1.6%); psychogenic disorders F4 - in 48 (38.7%), including panic disorder F41.0 - in 16 (12.9%), generalized anxiety disorder F41.1 - in 4 (3.2%), obsessive-compulsive disorder F42.2 - in 2 (1.6%), adaptation disorders in the form of depressive F43.21 and anxiety-depressive reaction F43.22 - in 26 (21.0%).
All patients received treatment with psychotropic drugs of various pharmacological groups in accordance with the leading psychopathological syndrome. As part of complex therapy, all patients were prescribed alprazolam as a main or auxiliary agent in a daily dose of 0.5 to 1.5 mg in 2-3 doses [1]. About half of the patients are 59 people. (47.6%) fell ill for the first time: they were diagnosed with a first-time depressive episode (8), adaptation disorders (26), neurotic anxiety-phobic disorders (14), organic disorders (4), low-grade schizophrenia (5) and paranoid schizophrenia (2 ). Before entering the clinic, these patients practically did not receive (with the exception of some recommendations from neurologists) psychotropic drugs, including tranquilizers. The remaining patients had previously taken various drugs, including benzodiazepines, but none of the patients had symptoms of established drug dependence at the time of their visit to the clinic.
When prescribing alprazolam, primarily its anxiolytic and antidepressant effects were taken into account. Weak sedative, hypnotic, muscle relaxant and amnestic effects, especially in small doses, made it possible to use it as a daytime tranquilizer in outpatients, including workers.
As is known, one of the main indications for the use of alprazolam is generalized anxiety disorder (GAD), but the diagnostic criteria for GAD are still controversial [3], and anxiety is often present in other forms of neuroses and depression. In our study, there were few patients with this diagnosis, and all of them took alprazolam in combination with SSRI antidepressants, mainly paroxetine. The anti-anxiety effect of these antidepressants is comparable to alprazolam [48], but it appears several weeks after the start of therapy. In the first weeks of treatment, anxiety may increase and sleep may be disrupted. It is during this period that the prescription of tranquilizers, and in particular alprazolam, has no alternative. The duration of treatment in patients with GAD is from two weeks to two months at an average dose of 0.75 mg per day (0.25 mg 3 times a day).
When treating patients with panic disorder, doses of up to 1 mg per day were used in 3-4 doses. The duration of therapy ranged from 3 to 8 months. Observation of patients over time shows that at first panic attacks disappear quite quickly, then the anxious anticipation of an attack gradually reduces, fears decrease and, accordingly, avoidant behavior disappears. In some cases, in the presence of symptoms of depression and in order to prevent panic attacks, antidepressants from the SSRI group, in particular Cipralex, were additionally prescribed.
For obsessive-compulsive disorder, alprazolam (dose 0.5 mg per day) was used in one case in combination with fluoxetine for 1 month, then due to insufficient effectiveness, therapy was changed. In another case, in a patient with various obsessions (fears, ideas, compulsions) in combination with panic attacks and avoidant behavior, alprazolam at a dose of up to 1.5 mg per day in combination with etaprazine up to 8 mg per day was successfully used for a long time (more 4 years) with almost complete reduction of symptoms and restoration of social functioning, in the absence of symptoms of addiction.
Patients with depressive disorders, including endogenous and neurotic depression, in our study made up more than half of all observations - 58.2%. In most cases, the structure of the depressive syndrome included symptoms of anxiety, which was an indication for the prescription of apprazolam, especially in the first weeks of therapy, before the onset of the anxiolytic effect of antidepressants. For primary depressive episodes and recurrent depression, alprazolam was used mainly as part of complex therapy along with antidepressants of various generations (maprotiline, azaphene, paroxetine, mirtazapine, Cymbalta, Valdoxan, etc.), and small doses of some antipsychotics (sulpiride). In some cases, hypnotics (zopiclone) were additionally prescribed for sleep disturbances. Treatment of depression in the context of bipolar disorder (BD) had its own characteristics, taking into account the possibility of transition to the manic phase, especially with BD-1. Antidepressants that do not cause an inversion of affect were used (azafen, valdoxan, fevarin). Already during the relief therapy, anticonvulsants (vaporates, carbamazepine) and antipsychotics (quetiapine, olanzapine) were prescribed, which the patients continued to take during the period of remission as maintenance therapy. In bipolar disorder-11, depressive symptoms were treated with antidepressants from the SSRI group, venlafaxine, valdoxan in combination with alprazolam, which has an anxiolytic effect, especially in the first weeks of therapy before the development of the antidepressants’ own effects, and potentiates their antidepressant activity [5]. Among anticonvulsants, preference was given to lamotrigine and valproic acid preparations, and among antipsychotics, preference was given to quetiapine. In almost half of the cases of neurotic depression (12 people), alprazolam was used as monotherapy, at a dose of 0.75-1 mg for 4-7 weeks with a good effect, i.e. almost complete recovery.
This once again indicates that alprazolam has an antidepressant effect.
Many patients with depression experienced symptoms of somatic anxiety (including somatized depression), which disappeared along with mental anxiety. Perhaps in this case we can talk about the vegetotropic effect of alprazolam, like other benzodiazepines (phenazepam, diazepam). Another explanation is possible: along with anxiety, its somato-vegetative “accompaniment” also goes away.
In the history of many patients with panic disorder, anxiety-phobic disorders, and recurrent depression, there were episodes of effective use of alprazolam with tianeptine with a fairly rapid reduction of symptoms and restoration of social functioning.
For organic brain lesions, alprazolam was used as an anti-anxiety and sedative in combination with small doses of sedative antipsychotics (clozapine, olanzapine), nootropics. The duration of therapy is no more than a month, daily doses are up to 0.75 mg. Antipsychotics in these cases were prescribed as behavior correctors, and alprazolam “mitigated” the side effects.
In case of sluggish schizophrenia, alprazolam was prescribed as part of a polymorphic neurosis-like syndrome, which included anxiety-phobic, panic, obsessive-compulsive and depressive disorders. As a rule, it was used in combination with antidepressants (rexetine, mirtazapine, amitriptyline), antipsychotics (sulpiride, sonapax, chlorprothixene, quetiapine), hypnotics (zopiclone, zolpidem), short courses from two to four weeks at a dose of 0.5-0. 75 mg per day.
A special group consisted of patients with paranoid schizophrenia, to whom alprazolam was prescribed in addition to antipsychotics (clozapine, olanzapine, paliperidone, risperidone) as an anti-anxiety agent and potentiating sedative effect. This made it possible to reduce doses of antipsychotics, which is especially important when conducting treatment on an outpatient basis in order to improve social adaptation and quality of life. Courses of therapy of varying durations, from two weeks to several months, depending on the indications, the dose of the drug is 1-1.5 mg per day.
Thus, the study confirmed that alprazolam has high anxiolytic activity even in small doses with insignificant sedative and hypnotic effects, which allows its use as a daytime tranquilizer and anxiolytic in patients with a wide range of anxiety-phobic and panic disorders of various origins. Alprazolam differs favorably from other benzodiazepines by having an antidepressant effect, so it can be used to treat not only anxiety, but also depressive disorders. There is good tolerability and high safety of the drug, as well as a virtual absence of the risk of drug dependence when using small doses and strictly observing the indications for use. Alprazolam can be prescribed in inpatient and outpatient settings, both in short courses and long-term, depending on the nature of mental disorders.
Bibliography
1. Arena D, Rosenbaum D. Pharmacotherapy of mental disorders. - M.: Binom, 2004. - 416 p. 2. Bondarev V.G., Shiryaev G.L., Pavlova E.Ya. Alprazolam as an emergency treatment for acute stress disorders [practical observations] // Modern therapy of mental disorders. - 2007. - No. 4. P. 32-33. 3. Vepttsev D.Yu., Marchenko A.S. Generalized anxiety disorder: epidemiology, pathogenesis, diagnosis and pharmacotherapy [literature review] // Mental 34. disorders in general medicine. - 2011. - No. 1. - P. 56-64. 4. Gubsky Yu.I., Shapovalova VA, Kugko IM, etc. Medicines in psychopharmacology. — Kyiv: Health; Kharkov: Torsing, 1997. - 288 p. 5. Danilov D.S. Optimization of depression therapy at the current stage of development of psychopharmacology // Neurology, neuropsychiatry, psychosomatics. 2013; 1:22-27. 6. Kalinin V.V. The drug Xanax (Alprazolam): Application in clinical practice // New drugs. 1998; 12:15-28. 7. Kalinin V.V. New achievements in the treatment of mental illnesses / Ed. S.N. Mosolova. - M.: Binom, 2002. - P. 409-431. 8. Kalinin V.V., Zasorina M.A., Voloshin V.M. and others. Symptoms of panic disorder, alexithymia and the effectiveness of alpraeolam therapy // Social and clinical psychiatry. - 1993; 3[3]:100-106. 9. Kalinin 8.8., Maksimove MA. Modern ideas about phenomenology, pathogenesis and treatment of anxiety states // Social and clinical psychiatry. -1993; 3(2) 1:128-142. 10. Clinical pharmacology according to Goodman and Gilman. / Ed. A.G. Gilman. M.: Praktika, 2006. - 1648 p. 11. Mashkovsky MD. Medicines. - Kharkov: Torsing, 1997. - T. 1 - 560 p. 12. Mosolov S.N. Alprazolam is the first benzodiazepine with a thymotranquilizing effect. Vrach. 1999; 8:23-24. 13. Fursov B.V., Pvlsuev 0.0. Application of apprazolam in clinical practice // Social and clinical psychiatry. - 2012; 22(1 ]:95-100. 14. Aden GC, Thein SG Alprazolam compared to diazepam and placebo In the treatment of anxiety // J. Clin. Psychiatry. 1980; 41:245-248. 15. Ballenger J., Burrows G., DuPont R. et al. Outcome of panic disorder // Archives General Psychiatry. - 1988; 45(5): 413-421. 16. Bandelow V. The medical treatment of obsessive-compulsive disorder and anxiety // CNS Spectr. 2008; 9(Suppl 14]:37-46. 17. Banerji JR, Brantingham R, McEwan GD et al. A comparison of alprazolam with amitriptyline in the treatment of patients with neurotic or reactive depression // lrish J. Med. Sci. 1989; 158110-113 18. Barnone F., McMahon AD., Davey PG et al. Association of road-traffic accidents with benzodiazepine use // Lancet. 1998;352:1331-1336. 19. Baselt RS, Carvey RH Oisposition of Toxic Drugs and Chemicals in Man. - Foster City, CA: Chemical Toxicology Institute, 1995. 20. Bond A., Silveira JC, Lader M. Effects of single doses of alprazolam and alcohol alone and in combination psychological performance / /Hum. Psychopharmacol. 1991; 6:219-228. 21. Bond AJ, Silveira JCThe combination of alprazolam and alcohol behavioral aggression // J. Stud. Alcohol. 1993; 11(Suppl]:30-39. 22. Bond AJ, Curran HV, Bruce MS et al. Behavioral aggression in panic disorders after 8 weeks' treatment with alprazolam // J. Affect. Disord. 1995; 35: 117-123. 23. Brousse TJ, Spiegel DA, Gregg SF, Nuuarello A. Predictors of alprazolam discontinuation with and without cognitive behavior therapy in panic disorder// Am. J. Psychiatry.1995; 152:1156-1160. 24. Chouinard GF, Apnable L., Fontaine R. Alprazolam in the treatment of generalized anxiety and panic disorders: a double-blind placebo-controlled study // Psychopharmacology. - 1982;7713]:229-233. 25. Cohn J.V. Long-term comparison of alprazolam, lorazepam and placebo in patients with an anxiety disorder // Current Therapeutic Research.- 1984;35:100-112. 26. Cohn J.B. Double-Blind Efficacy and Safety Study Comparing Alprazolam, Diazepam and Placebo in Clinical Anxiety Patients // Journal Clinical Psychiatry.- 1981; 42(9):347-351. 27. Cohn J.V., Wilcox CS Low-sedation potential of buspirone compared with alprazolamand and lorazepam in the treatment of anxious patients: A double-blind study // J. Clin. Psychiatry. 1986; 47:409-412. 28. Curran HV Benzodiazepines, memory and mood: A review // Psychopharmacology. 1991; 105:1-8. 29. Davison K., Farquharson RG, Khan M.S.A douYe blind comparison of alprazolam, diazepam and placebo in the treatment of anxious out-patients // Psychopharmacology. - 1983; 8014):308-310. 30. Diegoli MSC., da Fonseca A.M., Diegoli S.A. et a/. A double-blind trial of four medications to treat severe premenstrual syndrome // lnt. J. Gynecol. Obstet. 1998; 62:63-67. 31. Edwards JG, Inman WHW, Pearce GL et al. Prescription-event monitoring of 10895 patients treated with alprazolam // Br. J. Psychiatry. 1991; 158:387-392. 32. Elie R., Lamontagne Y. Alprazolam and diazepam in the treatment of generalized anxiety // J. Clin. Psychopharmacol. 1984; 4:125-129. 33. Enkelman R. Alprazolam versus buspirone in the treatment of outpatients with generalized anxiety disorder // Psychopharmacology. 1991; 105:428-432. 34. Galpern WR, Milleg LG, Ggeenblatt OJ et al. Differential effects of chronic lorazepam and alprazolam on benzodiazepine blinding and GABA-A-receptor function // British Journal Pharmacology. - 1990; 101(4):839-842. 35. Greenblatt OJ, von Moltke LL, Harmatz JS et al. Alprazolam pharmacokinetics, metabolism, and plasma levels: clinical implications // Journal Clinical Psychiatry. - 1993; 54 [Suppl].J:4-11. 36. Greenblatt OJ, Wright S.E. Clinical pharmacokinetics of alprazolam.Therapeutic implications // Clinical Pharmacokinetics. - 1993;24[6]:453-471 37. Harrison WM, Endicott J, Nee J. Treatment of dysphoria with alprazolam. A controlled study // Arch.Gen. Psychiatry. 1990; 47:270-275. 38. Jordan HW, Wiffiams V.S. Tardive dyskinesia successfully treated with alprazolam // Journal National Medical Association. - 1990; 82[9]: 673-675. 39. Keller M.V., Lavori PW, Goldenberg I.M. et al. Influence of depression on the treatment of panic disorder with imipramine, alprazolam and placebo // Journal Affective Disorders. - 1993; 28[1]:27-38 40. Kolin IS, Linet OJ Double-blind comparison of alprazolam and diazepam for subchronic withdrawal from alcohol // J. Clin. Psychiatry. 1981;42:169-173. 41. Laakman G., Faltermaier-Temize/ M., Bossert-Zaudig S. et al. Treatment of depressive outpatients with lorazepam, alprazolam, amitriptyline and placebo // Psychopharmacol ogy. 1995; 120:109-115. 42. Marazitti D., Carlini M., Dell'osso L. Treatment strategies of obsessive-compulsive disorder and panic disorder/agoraphobia // Curr. Thor. Med. Chem.2012. Feb 1. 43. McLoad DR, Hoehn-Saric R., Zimmerli WD et al. Treatment effects of alprazolam and imipramine: Physiological v subjective changes in patients with generalized anxiety disorder // Biol Psychiatry 1990; 28 849-861. 44. Muhleg N. The GABA system in anxiety and depression and its therapeutic potential// Neuropharmacology. - 2012;62(1):42-53. 45. Moulan S., Giorlando F., Nordfjarn T. et al. The role of alprazolam for the treatment of panic disorder in Australia // Australian New Zealand Journal Psychiatry. - 2012; 46[3]:212-224. 46. Petty F., Trivedi M.N., Fulton M. et al. Benzodiazepines as antidepressants: does GABA play a role in depression? // Biological Psychiatry. - 1995;38[9]:578-591. 47. Physicians' desk reference. - Montvale, NJ: R. Medical Economics Data Production Company, 1995. 48. Rickels K., Schweizer E. Panic disorder: long-term pharmacotherapy and discontinuation // J. Clin. Psychopharmacol. 1998;2:12-18. 49. Rocca R., Fonzo V., Scotta M. et al. Paroxetine efficacy in the treatment of generalized anxiety disorder // Acta Psychiatrica Scandinavica.- 1997; 95(5):44-450. 50. Romach M.K., Busto UE., Sobell LCet al. Long-term alprazolam use: Abuse, dependence or treatment? // Psychopharmacol. Bull. 1991;27:391-395. 51. Ramach M., Busto I., Somer G. et al. Clinical aspects of chronic use of alprazolam and lorazepam // Am.J. Psychiatry. 1995; 152:1161–1167. 52. Sellers E.M., Cigaulo DA, DuPont RL et al. Alprazolam and benzodiazepine dependence // J. Clin. Psychiatry. 1993; 54[Suppl 10)64-75. 53. Singh AN, Nair NP, Suran - Cadotte B. et al. A double blind comparison of alprazolam and amitriptyline hydrochloride in the treatment of nonpsychotic depression // Canadian Journal Psychiatry. - 1988; 33(3):218-222. 54. Spiegel DA Psychological strategies for discontinuing benzodiazepine treatment // JClin Psychopharmacol 1999; 19:17S-22S. 55. Srisurapanont M., Boonyanaruthee V. Alprazolam and standard antidepressants in the treatment of depression: a meta-analysis of the antidepressant effect // Joumal Medical Association Thailand. - 1997; 80[3]:183-188. 56. Sumner DD Benzodiazepine-induced persistent amnestic disorder: Age older adults at risk? //Arch. Psychiat. Nursing. 1998; 12:119-125. 57. Surwit RS, McCubbln JA., Kuhn S.M. et al. Alprazolam reduces stress hyperglycemia in ob/ob mice // Psychosomatic Medicine. - 1986; 48(3-4):278-282 58. Tollefson GD, Luxenberg M, Valentine R. et al. An eagle label trial of alprazolam in co-morbid irritable bowel syndrome and generalized anxiety disorder // J. Clin. Psychiatry. 1991; 52:502-508. 59. Torres-Ruiz A.T. A double-blind study of alprazolam and lorazepam in the treatment of anxiety // J. Clin. Psychiatry. 1983; 44:60-62. 60. Weissman M.M., Prusoff V., Sholomskas AJ, et al. A double-blind clinical trial of alprazolam, or placebo in the depressed elderly // J. Clin. Psychopharmacol. 1992; 12:175-182.
Experience of alprazolam usage in a complex therapy of psychiatric disorders.
NA Tuvina, DS Danilov, VV Balabanova, SV Prochorova, IG Korobkova
Department of Psychiatry and Addiction
IM Sechenov First Moscow State Medical University
SUMMARY : Literary data, defining the peculiarities of alprazolam action, its psychotropic effects, tolerability, the possibility of its usage in various psychiatric disorders proven by numerous studies, were analyzed. Our own experience of alprazolam use, mainly in combination with drugs of other psychopharmacological groups [antidepressants, neuroleptics, anticonvulsants] in the treatment of psychiatric disorders: depressions of various genesis, disorders of anxiety and phobic spectrum, obsessions were represented. 124 psychiatric in- and outpatients showed high efficacy and good tolerability of small daily doses of alprazolam and the absence of dependence and withdrawal syndrome.
KEY-WORDS : alprazolam, panic disorder, generalized anxiety disorder, obsessive-compulsive disorder, acute stress disorder, schizophrenia, affective disorder.
CONTACT : NA Tuvina ( [email protected] ].
How does addiction to Alprazolam develop?
The standard daily dose of a tranquilizer is 0.75–4.5 mg, which is divided into three doses (it is recommended to take the tablets at the same time). The risk of developing psychological and physical dependence on Alprazolam is especially high if the course of treatment lasts longer than 4–6 weeks.
One of the prerequisites for the safe use of benzodiazepines is their gradual, slow withdrawal with a gradual reduction in the daily dosage. Quitting Alprazolam often takes longer than the therapy itself. Abrupt withdrawal of medication causes:
- recurrence of initial symptoms: feelings of anxiety, fear and other emotional and mental disorders reappear;
- “recoil syndrome”, which is accompanied by insomnia and panic attacks.
But the most difficult to tolerate is withdrawal syndrome, which manifests itself:
- irritability, depression, apathy;
- nausea, vomiting;
- malaise, weakness and weakness;
- increased sensitivity to bright light, loud sounds, strong odors;
- decreased concentration;
- convulsive seizures;
- hallucinosis;
- crazy ideas;
- depersonalization;
- pain syndrome;
- tremor of hands, tongue;
- tinnitus;
- slow speech and general lethargy.
It is these symptoms that force the patient to return to the pills, and often he takes the medicine in a higher dose than was prescribed by the doctor. At the same time, there is a fear of stopping treatment, because this is accompanied by a pronounced deterioration in well-being.
Alprazolam in Russia
Oddly enough, in Russia you can now easily get this drug. Of course, you can’t buy it just like that: by going to the pharmacy and begging the pharmacist to give you a pack. This drug belongs to the list of medicines subject to quantitative accounting. This means that the prescription for it (with all the stamps and signatures) is given and remains in the pharmacy. But, nevertheless, for a decent amount on the black market you can find several tablets of Xanax, so coveted by some fans of modern hip-hop culture. This means that it is quite possible to use it systematically. We wrote above what this entails.
How to break your addiction to Alprazolam
A strict indication for drug detoxification is symptoms of overdose. Cleansing therapy is carried out only in a hospital, it consists of the following stages:
- gastric lavage;
- use of high doses of adsorbents;
- use of medications from the group of benzodiazepine receptor antagonists;
- correction of concomitant somatic disorders.
If there is no effect from the procedures performed, hemodialysis and plasmapheresis are indicated.
However, the vast majority of patients started taking the medication for therapeutic reasons, and detoxification will inevitably lead to relapse. That is why the drug is continued, but in order to relieve dependence on Alprazolam, its dose is gradually reduced over several weeks.
In this condition, round-the-clock medical monitoring and timely pharmacological correction of possible complications are necessary. Therefore, until the end of treatment, the addict must remain in an inpatient drug treatment clinic.
A course of psychotherapy is mandatory. Experts suggest that consultations with a psychologist will help cope with the underlying disease, for the treatment of which Alprazolam was, in fact, prescribed. Sometimes, if psychotherapy is not enough, antidepressants and “mild” sedatives are additionally selected.
Undoubtedly, many diseases cannot be treated without benzodiazepines, but in order to avoid the development of dependence, it is important to strictly follow all the recommendations of the attending physician regarding the dosage regimen. Exacerbation of the condition, emotional discomfort, or any symptoms that bother the patient are mandatory indications for consulting a doctor.
Deaths from Xanax overdose
It is difficult to get a fatal overdose from alprazolam alone, but the thing is that it is often mixed with other, more potent substances: for example, opiates or alcohol. And such a “combo” can be very dangerous. This is often done in the West, and it is possible that the same fashion will come to Russia.
The most sensational case in recent times: the death of rapper Gustav Ara, better known as Lil Peep. At the peak of his popularity, at 22, he became heavily involved in drugs. Once, after mixing the powerful synthetic opioid fentanyl with Xanax, his breathing stopped because alprazolam significantly enhances the depressant effects of other drugs on the respiratory system, such as opiates or alcohol.
It is reported that Lil Peep had previously used drugs and was addicted to cocaine and alprazolam; He regularly mentioned the topic of drugs in his texts and messages on social networks. In one Instagram post, Gustav declared himself a "productive drug addict" and called for abstinence from drugs.
Do you want to know about the cost of services?
8 call our specialist
Literature:
- Fursov B.B., Papsuev O.O. Use of alprazolam in clinical practice. - Special clinical psychiatry, 2012. - vol. 22, no. 1.
- Mosolov S.N. Alprazolam is the first benzodiazepine with a thymotranquilizing effect. - Doctor, 1999. - No. 8
- Kalinin V.V. New data on the use of alprazolam in psychiatry (literature review). - Psychiatry and psychopharmacotherapy, 2000. - T.2, No. 4.
- Sychev D.A., Zhuchkov A.V., Tereshchenko O.V. Gradual withdrawal (deprescribing) of benzodiazepine tranquilizers. — Neurology, neuropsychiatry, psychosomatics, 2021. — 11(1).
The text was checked by expert doctors: Head of the socio-psychological service of the Alkoklinik MC, psychologist Yu.P. Baranova, L.A. Serova, a psychiatrist-narcologist.
CAN'T FIND THE ANSWER?
Consult a specialist
Or call: +7 (495) 798-30-80
Call! We work around the clock!